
Abstract

Dear Editor,
We read with great interest the case report by Surana A et al describing refractory septic shock caused by phenotypically pandrug-resistant (PDR) Pseudomonas aeruginosa in a critically ill patient with chronic kidney disease and multiorgan failure. 1 The authors provide a careful clinical and microbiological account of a highly challenging infection, highlighting the urgent threat posed by advanced antimicrobial resistance. Such reports are important for understanding the real-world clinical consequences of diminishing anti-microbial options. We would like to offer an additional perspective that may further enrich the interpretation of this important case: the growing discordance between phenotypic antimicrobial susceptibility testing (AST) and underlying genotypic resistance mechanisms in P. aeruginosa, and how reliance on phenotype alone may oversimplify the designation of “pandrug-resistance” (non-susceptibility to all routinely tested antimicrobial agents across clinically relevant categories).2-4
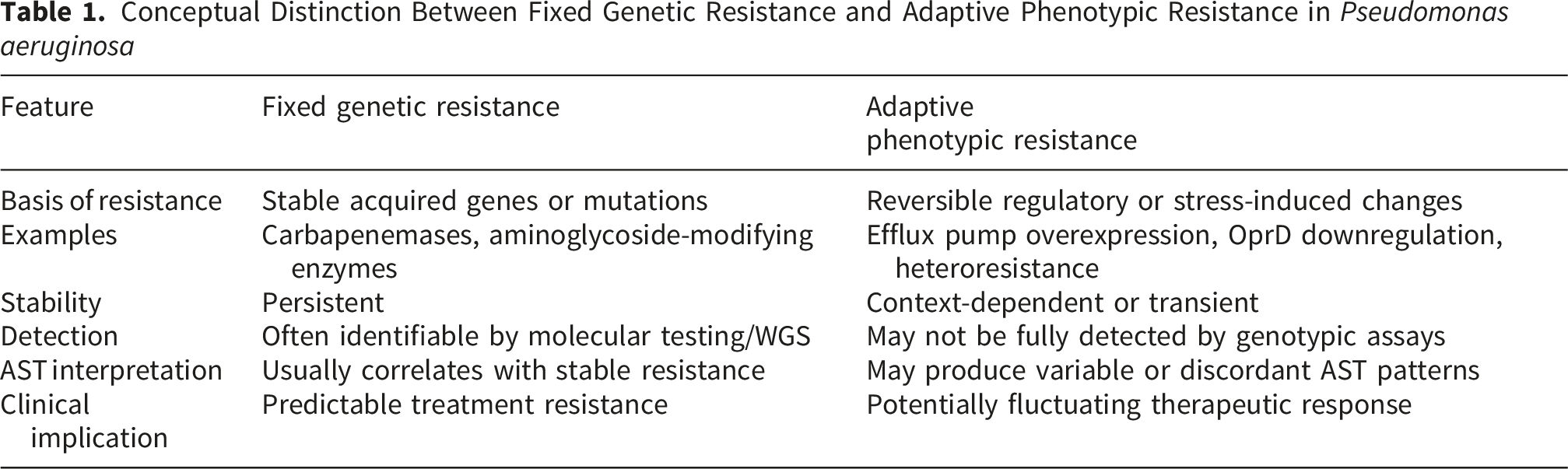
In P. aeruginosa, phenotypic resistance often reflects the combined effect of multiple, potentially reversible or context-dependent mechanisms, including efflux pump overexpression, porin loss (notably OprD), adaptive lipid A modification, and regulatory mutations affecting iron uptake pathways.3,5-7 These mechanisms may produce broad in-vitro resistance profiles even in the absence of horizontally acquired carbapenemases or other stable resistance determinants.5-7 Accordingly, phenotypic classification as PDR does not necessarily imply irreversible biological non-responsiveness. This distinction is particularly relevant when interpreting susceptibility to agents such as cefiderocol and colistin 8 and 9. Cefiderocol susceptibility is influenced by mutations in siderophore transport systems and iron-regulated pathways, which may not be constitutively expressed and are incompletely characterized by routine AST. 8 Similarly, colistin resistance in P. aeruginosa is often driven by adaptive and heteroresistant subpopulations rather than fixed genetic resistance, a phenomenon that standard broth microdilution may fail to detect. 9
Conceptual Distinction Between Fixed Genetic Resistance and Adaptive Phenotypic Resistance in Pseudomonas aeruginosa
The absence of genotypic characterization, such as whole-genome sequencing or targeted resistome analysis, therefore limits the interpretability of the “PDR” designation in this case. While we fully recognize the practical constraints in urgent clinical settings, genotypic data could have provided valuable insight into whether the observed resistance reflected fixed molecular determinants or potentially targetable adaptive pathways. Emerging rapid molecular diagnostics, including resistome profiling and real-time genomic sequencing, may further enhance future clinical workflows by enabling earlier differentiation between stable acquired resistance determinants and adaptive phenotypic resistance mechanisms. 10 However, implementation remains limited in many healthcare settings because of cost, infrastructure requirements, bioinformatics expertise, and variable turnaround times, particularly in low- and middle-income countries. Despite these limitations, progressive integration of molecular diagnostics into reference laboratories and tertiary-care centers may improve interpretation of complex resistance phenotypes in the future.
This distinction has implications not only for individual patient management but also for how such cases are extrapolated to guide policy, stewardship, and future therapeutic development. Importantly, our intention is not to challenge the clinical decisions made in an extraordinarily complex and rapidly evolving situation. Rather, we suggest that future reports of PDR P. aeruginosa may benefit from explicitly contextualizing phenotypic resistance within its genotypic framework, where feasible. As antimicrobial development advances toward mechanism-specific and precision-based strategies, integrating genotypic and phenotypic data will become increasingly important to avoid conflating microbiological resistance with complete therapeutic inaccessibility.
Footnotes
Acknowledgements
The authors acknowledge the continuous academic support and collaborative research environment provided by the Infectious Diseases Research Group, Squad Medicine and Research (SMR), India. The group’s commitment to advancing infectious diseases and antimicrobial resistance research through interdisciplinary collaboration and scientific discussion is sincerely appreciated.
Author Contributions
CRediT authorship contribution statement. Suvvari TK & Kocharlakota SVNS – Idea, conceptualization, supervision, resources, formal analysis writing & editing draft, approved final draft. Kandi V – Idea, Project Administration, formal analysis writing & editing draft, approved final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AI Statement
AI and AI-assisted technologies were not used to generate any content of this manuscript.