
Abstract
Pancreatic calculi are the sequelae of Chronic Pancreatitis and can occur in about 50% of patients. These calculi produce the typical pancreatic pain experienced by patients, and pain relief is the most important goal of therapy. Herein, we present two cases of 66- and 39-year-old male patients who had severe abdominal pain associated with calculi obstructing chronic pancreatitis. The two patients were successfully managed with distal pancreatectomy. The decision regarding the management of pancreatic duct stones should be made in a multidisciplinary fashion; it depends on multiple factors. The results of these cases showed that distal pancreatectomy with pancreatico-jejunostomy could be offered as curative treatment for selected patients with obstructive chronic pancreatitis.
Introduction
Chronic pancreatitis can be classified into three forms: chronic calcifying pancreatitis, chronic obstructive pancreatitis, and steroid-responsive pancreatitis. The result of chronic pancreatitis is destruction of the gland, which manifests as abdominal pain, exocrine and endocrine insufficiency, and secondary pancreatic cancer. 1 Pancreatic calculi (PC) are the sequelae of CP and can occur in about 50% of patients. These calculi aggravate or produce the typical pancreatic pain experienced by patients by obstructing pancreatic ducts and producing upstream ductal hypertension and subsequent parenchymal hypertension. 2 Pain relief is the most important goal of therapy in patients with chronic calculus pancreatitis. Ductal decompression of the main pancreatic duct (MPD), with clearance of calculi, leads to pain relief in most patients. This can be performed surgically or endoscopically. 3
We present two cases of male patients diagnosed with chronic calculous pancreatitis who were managed surgically.
Case 1
A 66-year-old male, with a history of Diabetes Mellitus (DM II), chronic pancreatitis, and chronic diffuse abdominal pain of several years, presented to our care for further investigation and management. The patient has a history of heavy alcohol intake of 20 years duration, stopped 10 years ago. The patient reported no associated symptoms, and his physical exam was unremarkable except for mild epigastric tenderness. Laboratory studies were unremarkable except for mildly disturbed liver function tests (Gamma-GT (GGT): 485 IU/L, Bilirubin D/T 0.7/1.2 mg/dL, Amylase: 85 IU/L, Lipase: 4 IU/L, SGOT: 47 IU/L, SGPT: 54 IU/L).
Computed Tomography (CT) scan of the abdomen and pelvis showed significant intrahepatic biliary ductal dilation predominating in the left hepatic lobe. The common bile duct (CBD) is dilated, measuring up to 2 cm. Distally, it shows enhancing walls and minimal surrounding fat stranding. A dilated pancreatic duct measuring up to 1 cm with a 9 mm stone is seen at the orifice along with proximal dilatation. This is accompanied by pancreatic atrophy (Figure 1). Abdomen/Pelvis CT scan showing dilated pancreatic duct with atrophic pancreas. Pancreatic stone (blue arrow)
Magnetic resonance cholangiopancreatography (MRCP) showed filling defects in the common bile ducts, with a stricture in the head of the pancreas (Figure 2). MRCP showing filling defects in the common bile ducts (blue arrow) with stricture in the head of the pancreas (yellow arrow)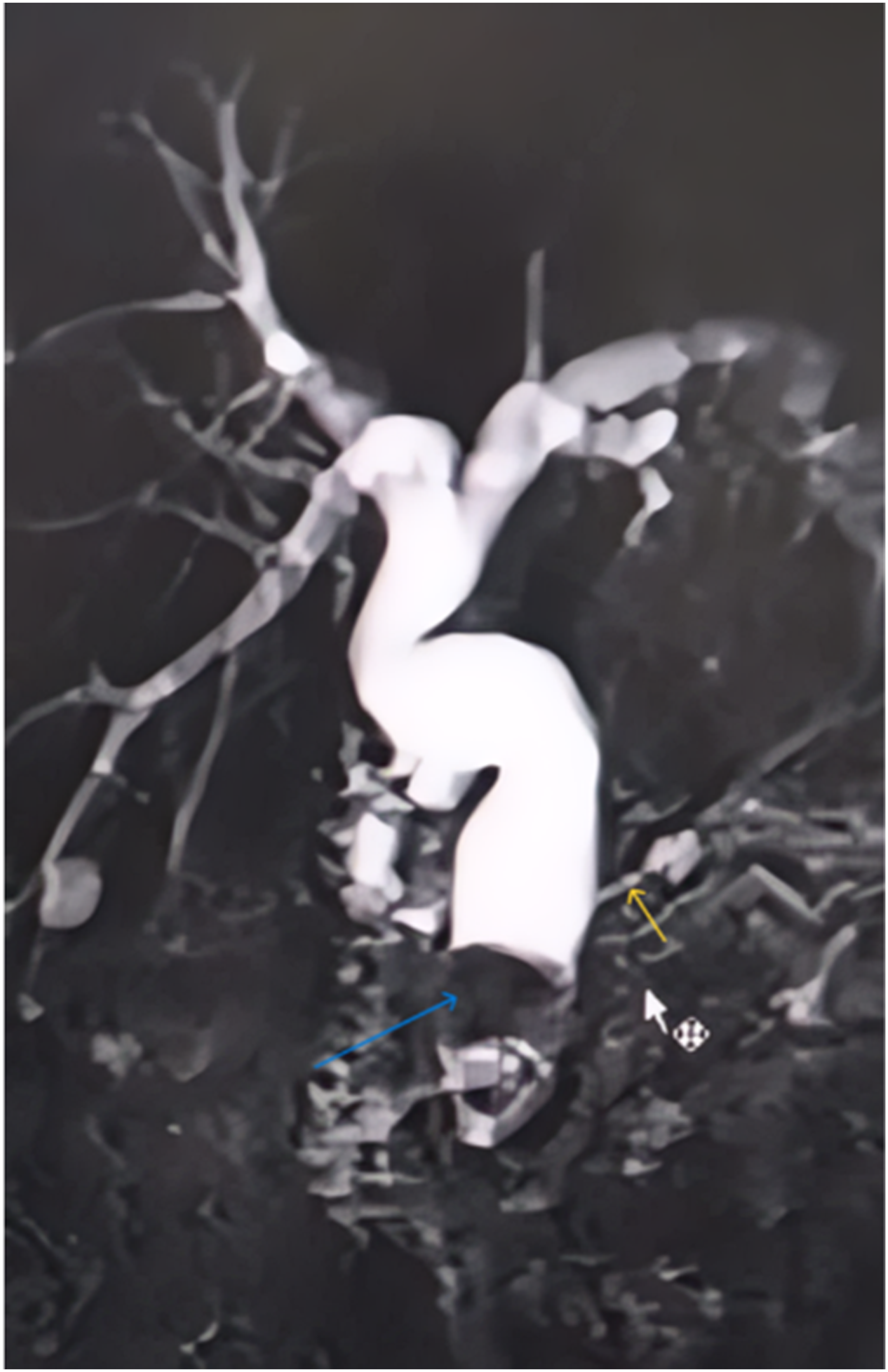
Endoscopic retrograde cholangiopancreatography (ERCP) revealed 10mm and 8mm CBD stones. Biliary sphincterotomy with sphincteroplasty and balloon sweeps with complete clearance of the CBD were achieved. It was noted that there was a long stricture in the head of the pancreas, along with a large stone and dilation of the main pancreatic duct downstream in the neck, body, and tail of the pancreas. Pancreatic sphincterotomy and minor papillary sphincterotomy were performed, but the stricture was not amenable to endoscopic resection (Figure 3). ERCP showing 10- and 8-mm CBD stones that were retrieved along with sphincteroplasty
After discussion with the gastroenterology team, a decision was made to proceed with surgical intervention, as the stones are larger than 5mm and there is limited expertise with lithotripsy.
The gastrocolic omentum was opened, exposing the lesser sac from the left of the hepatic flexure to the splenic flexure. The pancreas was fully exposed, and adhesions to the posterior wall of the stomach were removed. The pancreas was palpated, and the fibrosed distal pancreatic tail was identified. A very delicate dissection of the pancreatic tail was done to preserve the spleen. The pancreatic tail was completely excised. A radiologist was consulted intraoperatively to assess the exact location of the stone using ultrasound. A decision was made to proceed with spleen-preserving distal pancreatectomy and end-to-side pancreaticojejunostomy due to the normal appearing pancreas and fibrosis localized only to the tail of the pancreas. Following distal pancreatectomy, a needle was inserted into the duct of Wirsung after calcifications were removed. A 30cm jejunal loop distal to the ligaments of Treitz was divided. The distal limb was pulled through the mesocolon, and the pancreaticojejunostomy was completed. 50 cm distally, a side-to-side jejunojejunostomy was created mechanically. The mesentery was closed around the jejunojejunostomy. A liver biopsy was performed and sent to pathology; a lamellated drain was placed, and the abdominal layers were closed.
The patient had an uncomplicated hospital stay. On postoperative day 2, the patient passed flatus and was started on water and progressed to a regular diet. The diet was tolerated, bowel movements were normal, and the patient was discharged home on day 5 postoperatively on pancreatic enzyme supplement (Creon) and pain medication. The pathology result showed pancreatic atrophy with chronic pancreatitis and no malignant proliferation. The liver parenchyma was within normal limits.
Follow-up at one month postoperatively, the patient was very satisfied and reported complete resolution of the abdominal pain without pain management. One year post-surgery, the patient is still pain-free with no analgesic requirement and reports no complaints.
Case 2
A 39-year-old male, previously healthy, presented with severe epigastric pain and diaphoresis. 3 months prior to this presentation, he started experiencing epigastric pain that was relieved with pain medications. The patient is a heavy smoker of 40 packs/year, and does not drink alcohol. His review of systems was negative, and his physical exam was unremarkable except for severe epigastric tenderness.
An electrocardiogram showed no abnormalities. Laboratory tests were unremarkable except for mildly disturbed liver function tests (LFT); GGT: 84 IU/L, Direct bilirubin: 0.15 mg/dL, Total bilirubin: 0.31 mg/dL, Amylase: 107 IU/L, Lipase: 85 IU/L.
Abdominal ultrasound showed a liver of normal size, no intra- or extrahepatic biliary dilation, and no stones in the gallbladder. A CT Scan Chest-Abdomen-Pelvis displayed evidence of chronic pancreatitis with the presence of a 1cm stone in the main pancreatic duct. An MRCP showed stones in the proximal pancreatic duct at the level of the head, with the largest measuring 1.2 cm. The proximal main duct was dilated to 8 mm, the CBD was 4 mm in diameter, and the gallbladder was distended with mild surrounding fluid and the absence of stone (Figure 4). MRCP showing dilated proximal main pancreatic duct (blue arrow)
The patient was then transferred to our facility after he was deemed not amenable for sphincterotomy or lithotripsy due to stone size and lack of expertise. He underwent endoscopic ultrasound (EUS), which showed the entire pancreatic gland displaying a hypoechogenic, heterogeneous, flaky, globular appearance with microcalcifications, with a 12 mm stone at the level of the head and a cone shadow. The stone is compressing the Wirsung duct, which is dilated by 8 mm upstream. The CBD and the gallbladder were alithiatic (Figure 5). EUS showing the presence of a 12 mm stone at the level of the head and an 8 mm dilated Wirsung duct
The patient was scheduled for distal pancreatectomy with pancreatico-jejunostomy. Intra-operatively, dissection of the greater omentum attachment to the transverse colon and entry into the lesser sac was done, followed by dissection of the peritoneal attachment of the transverse mesocolon to the inferior part of the pancreas. Lateral to medial dissection of the pancreatic tail from the splenic vein and artery was carried out, followed by dissection of the distal pancreas and its removal from its attachment medial to lateral. A transmesocolonic passage of a jejunal limb to create an end-to-side pancreaticojejunostomy was performed manually. A latero-lateral anastomosis was done between the distal jejunum and 60cm from the pancreatico-jejunal anastomosis. Closure of the mesenteric defect was performed. Finally, a lamellated drain was placed, and the abdomen was closed in layers (Figure 6). Intra-op pictures of the surgery. Pancreas (blue arrow), pancreatico-jejunal anastomosis (yellow arrow)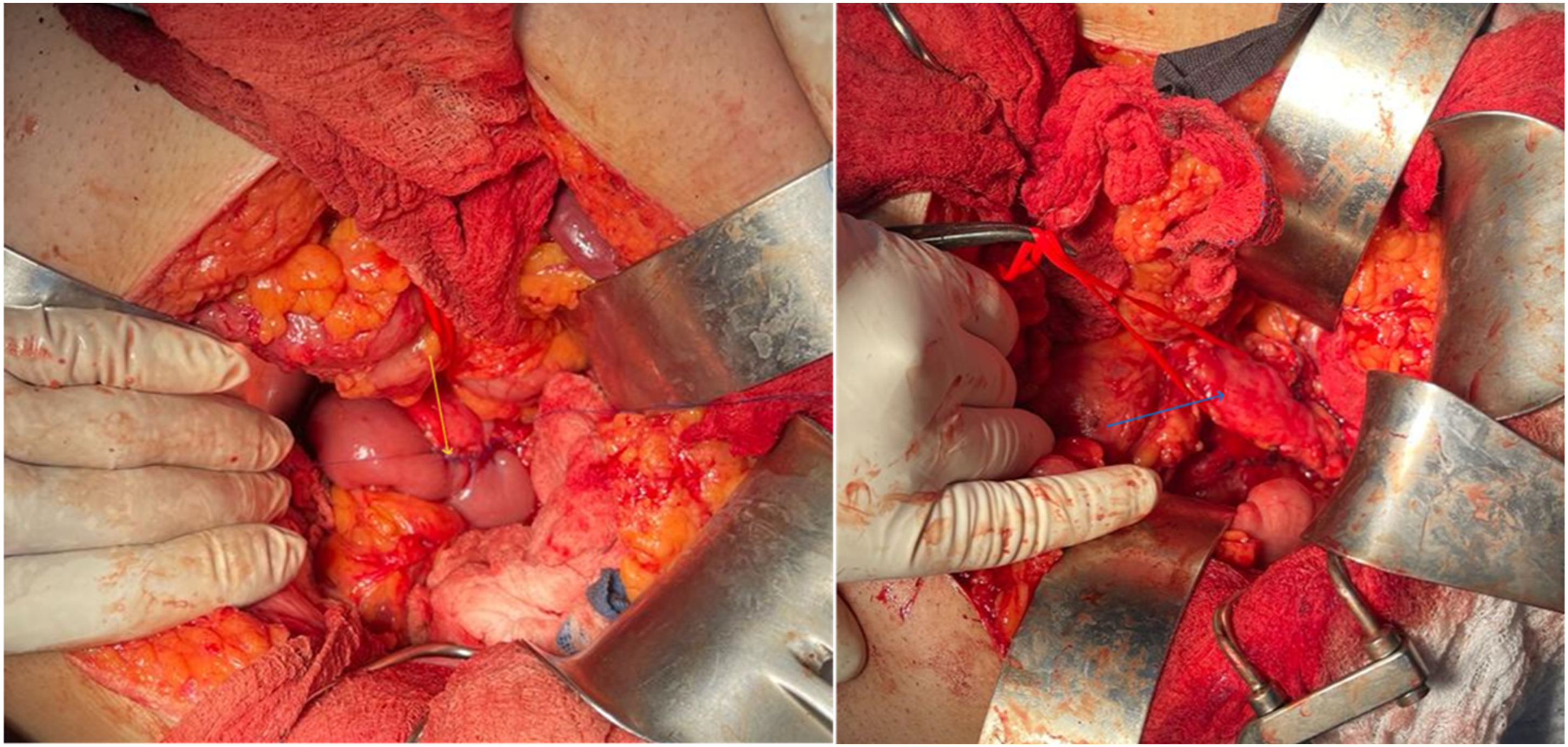
Patient had an uncomplicated hospital stay; patient passed gas on post-operative day 3, the diet was started on day 4 post-operatively, and progressed accordingly. Patient tolerated diet well, had a normal bowel movement, and was discharged on day 7 post-operatively with pancreatic enzyme supplement (Creon) and pain medications. The Pathology showed mild fibrosis, acinar atrophy, and protein plugs suggestive of chronic pancreatitis. Focal low-grade pancreatic intraepithelial neoplasia was negative for carcinoma.
Follow-up of the patient after 6 months was unremarkable. He denied any recurrent epigastric pain; he resumed his normal life activity.
Discussion
Chronic pancreatitis is a chronic inflammatory disorder that impacts the pancreas, marked by fibrosis and permanent structural alterations, leading to the loss of both endocrine and exocrine functions. The progression and symptoms of this disease can vary unpredictably, and pain levels may not consistently correspond to the pancreas’s morphological changes and surrounding tissue alterations. 3
Pancreatic calculi are categorized according to their quantity, composition, and position within the pancreas. They can be: 1. singular or multiple; 2. radio opaque, radiolucent, or mixed; 3. positioned within the main pancreatic duct (MPD), its side branches, or within the parenchyma; 4. situated in the head, body, or tail
Most PC are visible on X-rays, appearing opaque, although some may be transparent to X-rays or have a mixed appearance. 1 Management of chronic calculus pancreatitis requires a multidisciplinary approach ranging from conservative medical management to endoscopic and surgical approaches.
Medical Management
For patients with chronic pancreatitis, management usually includes oral pancreatic enzyme supplements, pain relievers, and adherence to a low-fat diet. 4 This statement is supported by the findings of Isaksson and Ihse, in which 15 of 19 patients treated with pancreatic enzymes for 1 week reported less pain compared with placebo. 5 The main goal is to prevent the activation of the exocrine portion of the pancreas. Some other unproven techniques were suggested, including medication used to dissolve stones, such as the old anticonvulsant trimethadione. 6
Non-surgical methods available include:
Extracorporeal Shock Wave Lithotripsy (ESWL)
ESWL effectively clears stones from the pancreatic duct and alleviates pain, as shown by a meta-analysis by Guda and Freeman. 7 Many other studies have also supported this claim, specifically for the treatment of large pancreatic calculi >5 mm.8,9
In concise terms, ESWL is considered a safe, noninvasive technique that works by using electromagnetic shock wave energy to generate compressive stress on the surface objects, such as pancreatic stones, to cause their fragmentation. Decreasing the size of the calculi can facilitate their sudden or endoscopic removal, ultimately resulting in pain relief.
This procedure is an important option for all chronic pancreatitis cases who have a large pancreatic stone (>5 mm) that cannot be extracted using endoscopic treatment.
As per Tandan and Reddy, a daily session at a rate of 90 shocks per minute can be done, with a maximum of 5,000-6,000 shocks allowed every session. 3
Contraindications to this technique include the presence of large concomitant stones found in the head, body, and tail of the pancreas or a secluded stone in the tail area, due to increased risk of splenic damage. 4 In addition, some calculi may be incompletely fragmented in some patients. In such instances, patients should be recommended for surgical intervention.
Other types of lithotripsy exist, including electrohydraulic lithotripsy, which combines three different shock waves, 10 and laser lithotripsy, where a laser light is emitted at a constant wavelength to induce fragmentation through wave mediation. 11
However, both methods are constrained by their accessibility, high expenses, and limited portability.
The endoscopic treatment has many limitations. For example, endoscopic management plays a limited role in the management of isolated calculi in the tail of the pancreas and stones involving the entire major pancreatic duct (MPD). 12 If endoscopic therapy failed, a multidisciplinary approach should be taken, including surgeons, gastroenterologists, and radiologists regarding surgical treatments, because it carries high morbidity and mortality. 13 This has led to new therapeutic modalities using direct endoscopic visualization to achieve MPD clearance, such as Peroral pancreatoscopy (POP). Stones with a density of more than 820.5 Hounsfield units are less likely to have a response to ESWL. Using intraductal lithotripsy, which may be accomplished by Electrohydraulic lithotripsy (EHL) and laser lithotripsy (LL), is essential to ease extraction throughout ERCP. 14
The electrohydraulic lithotripsy method involves a charge generator and a bipolar probe. This probe releases stimuli at its tip in water, forming a vapor plasma and bubbles that oscillate around the probe’s tip, generating shock waves. 14
High-frequency hydraulic pressure waves generate energy, leading to the fragmentation of adjacent stone. 15 The probe needs to be positioned near the stone but kept away from the ductal wall to prevent any damage or perforation to the duct. EHL can be done either under fluoroscopy by means of centering balloons or under direct vision cholangioscopically by employing SpyGlass technology. A direct cholangioscopic approach is preferred over a fluoroscopic approach to avoid ductal wall damage. 14
On the other hand, laser intraductal lithotripsy creates a laser beam at a precise wavelength that causes fragmentation of the stone. The utilization of laser technology is often restricted due to its expensive nature, alongside the presence of more economically viable alternatives. 16
While highly efficient in managing complex types of stones, it has been reported to achieve comparable success rates to ESWL based on the literature. However, there is limited data available for direct comparison. 14
In our cases, pancreatic lithotripsy was not readily available, with limited expertise. In addition, the patients had concomitant large stones with proximal strictures, rendering ERCP difficult, and lithotripsy might cause fragmentation of the stones, which would require several interventions and possible surgery. Therefore, the sound decision was to directly go for surgical treatment.
Surgical Management
The aim of the surgical treatment of the pancreatic duct stone is to remove the calculi obstructing the duct, decompress the duct, and preserve pancreatic tissue as much as possible. 4 Surgical options include drainage, resection, and combined procedures. The decision for the management should involve multiple disciplines and depend on multiple factors, including the location, size, number of stones, pancreatic duct size, the existence of main duct strictures, the presence of associated pseudocysts, the degree of stone obstruction, concerns about cancer, and the patient’s ability to tolerate surgery. 2 It has also been advocated that in cases with multiple strictures, pancreatic tail calculi, concerns of related head mass, or those who had unsuccessful Endo therapy, surgery is a better alternative. 17
Djuna Cahen et al showed in their study that surgery provides the most favorable long-term outcome compared to Endo therapy. Surgery provided quicker, more efficient, and longer-lasting pain relief than endoscopic drainage. The surgical patients also required fewer procedures. 18
Surgical techniques can be categorized as drainage or resection procedures, but over time, they’ve evolved to include combined drainage and resection methods as a third category. 19
Drainage procedures include Duval’s procedure, in which distal spleen-opancreatectomy is performed, and the pancreatic tail’s duct is achieved through an end-to-side pancreaticojejunostomy. The Puestow-Gillesby procedure, an adaptation of the Duval procedure, incorporates longitudinal pancreaticojejunostomy (LPJ) to guarantee that the pancreatic duct is properly drained, even when dealing with various strictures or stones. 19 and Partington–Rochelle variant of the Puestow procedure by evading distal spleno-pancreatectomy.
Regarding resection procedures, they include the Kausch–Whipple Pancreatico-duodenectomy, pylorus-preserving pancreaticoduodenectomy (ppPD), and Beger operation, which is duodenum-preserving pancreatic head resection [DPPHR]. 19
Hybrid procedures that include resection and drainage include Frey’s procedure, which includes excising the pancreatic head along with performing a longitudinal pancreaticojejunostomy. This procedure is widely applied due to its simplicity and lower morbidity and mortality compared to other procedures.
Izbicki technique involves longitudinal V-shaped removal of the ventral part of the pancreas, accompanied by the attachment of an LPJ to the pancreas capsule. This approach shows promise in managing rare cases of sclerosing ductal pancreatitis, also known as “small duct disease,” characterized by a main pancreatic duct diameter less than 3 mm. 19
In the two discussed cases, since the distal wirsung duct was patent with no stenosis and distal dilation, spleen-preserving distal pancreaticojejunostomy was a safe, less invasive, and simpler approach to alleviate pressure on the main pancreatic duct with no need to remove the stones. In our presented cases, there were no complications during or after surgery, with the pain completely relieved even after a year.
The main limitations of this study include the limited number of cases, the retrospective design, and the absence of a comparative group, which preclude definitive conclusions regarding the superiority of surgical management over other therapeutic modalities.
Conclusion
The decision regarding the management of pancreatic duct stones should be made in a multidisciplinary fashion, including surgeons, gastroenterologists, and radiologists. It depends on multiple factors, including the location, size, number of stones, pancreatic duct diameter, presence of strictures in the main duct, associated pseudocyst, related cancer concerns, the extent of the obstruction by stones, and tolerance of the operation. The results of these cases showed that surgery is still effective with minimal morbidity for patients, especially for spleen-preserving distal pancreatectomy with pancreaticojejunostomy.
Footnotes
Acknowledgements
We would like to aknowledge the departments of General Surgery, and Gastroenterology at Mount Lebanon Hospital for the support and help provided. As well as the encouragement of the faculty of Medicine and Medical Sciences at the University of Balamand.
Ethical Considerations
Case reports approved for publishing by ethical committee at Mount Lebanon Hospital University Medical Center.
Consent to Participate
Written Informed consent for publication was obtained from both patients.
Author Contributions
Ribal Aby Hadeer: first Author, conception of the work, design of the work, revising the work critically for important intellectual content, final approval of the version to be published. Soad Ghattas: review of literature, draft manuscript, revising the work critically for important intellectual content, final approval of the version to be published, and corresponding author. Ayman Tabche: provided revisions to scientific content. Preparation, creation and presentation of the published work, review of literature concerning endoscopic interventions. Johnny Salem: provided revisions to scientific content. Preparation, creation and presentation of the published work, review of literature concerning endoscopic interventions. Hani Maalouf: provided revisions to scientific content. Preparation, creation and presentation of the published work, review of literature concerning surgical intervention. Noha Al Hachem: supervision, validation, project administration,conception of the work,revising the work critically for important intellectual content, final approval of the version to be published project administration. Raja Wakim: supervision, validation, project administration,conception of the work, revising the work critically for important intellectual content, final approval of the version to be published project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.