
Abstract
Background
Intratracheal tumors are rare neoplasms that may pose significant diagnostic and therapeutic challenges because of their critical location within the central airway. Pleomorphic adenoma arising in the trachea is exceedingly rare, with only a limited number of cases reported in the literature.
Case presentation
We report a case of a 45-year-old patient presenting with stridor, dyspnea, and hemoptysis who was found to have a distal intratracheal mass located one to two tracheal rings above the carina. Bronchoscopic biopsy with planned cryotherapy was performed; however, airway management was particularly challenging due to the tumor’s location, which made tracheostomy unfeasible and distal endotracheal intubation technically difficult. During cryotherapy, manipulation of the lesion triggered bleeding, bronchospasm, and acute airway collapse, resulting in severe ventilatory compromise that required urgent airway stabilization and selective intubation distal to the tumor. Histopathological examination confirmed pleomorphic adenoma.
Conclusion
This case highlights the unique airway management challenges posed by intratracheal tumors located near the carina and underscores the importance of meticulous pre-procedural planning, anticipation of complications, and readiness for emergency airway interventions during bronchoscopic treatment. Even minimally invasive procedures such as cryotherapy may lead to life-threatening airway compromise when tumors are located in critical central airway regions.
Introduction
Pleomorphic adenoma is a benign mixed tumor composed of epithelial, myoepithelial, and mesenchymal components and most commonly associated with the salivary glands. Its occurrence in the tracheobronchial tree is exceedingly rare. 1 Symptoms such as dyspnea, hemoptysis, wheezing, and stridor are due to central airway obstruction. These symptoms often mimic more common respiratory conditions, leading to delayed diagnosis. 2 The location of the tumor within the airway significantly influences both clinical presentation and management. Tumors situated in the lower trachea near the carina pose a particular challenge because this area lies immediately proximal to the bifurcation into the main bronchi. 3 Endoscopic therapies such as cryotherapy are frequently used to treat central airway tumors, especially when surgical resection is not immediately feasible or when the tumor’s location makes resection high-risk. Cryotherapy works by applying extremely cold temperatures to ablate tumor tissue, leading to cellular destruction with relatively minimal thermal injury to surrounding normal tissue. In the context of central airway obstruction, cryotherapy has been associated with a favorable safety profile with a low incidence of serious complications, but moderate bleeding and airway reactions (e.g., spasm) can occur, particularly when tissues are highly vascular or when manipulation of the tumor disturbs adjacent airway structures. 4 Critical to the success of any intervention in this region is airway protection and ventilation, which are complicated when the tumor is located near the carina, a zone where advancing or placing an endotracheal tube beyond the lesion can be technically difficult. 5 In this report, we describe a case of a pleomorphic adenoma located 1–2 tracheal cartilage rings above the carina, presenting with stridor, dyspnea, and hemoptysis, and complicated by difficult airway management and complete airway collapse during cryotherapy, illustrating the challenges posed by tumor location as well as the inherent risks of endoscopic treatment in this high-risk anatomical context.
Case Presentation
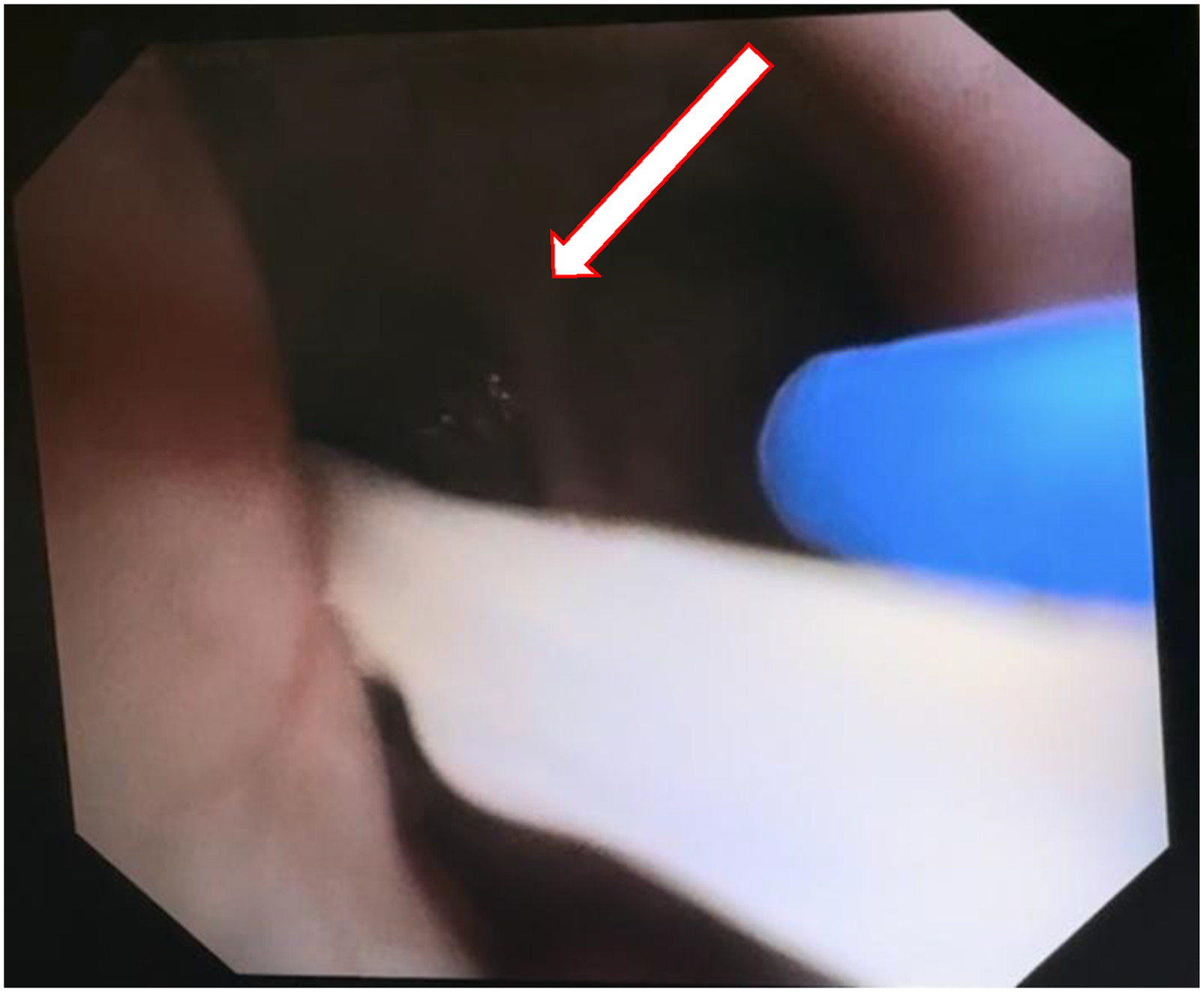
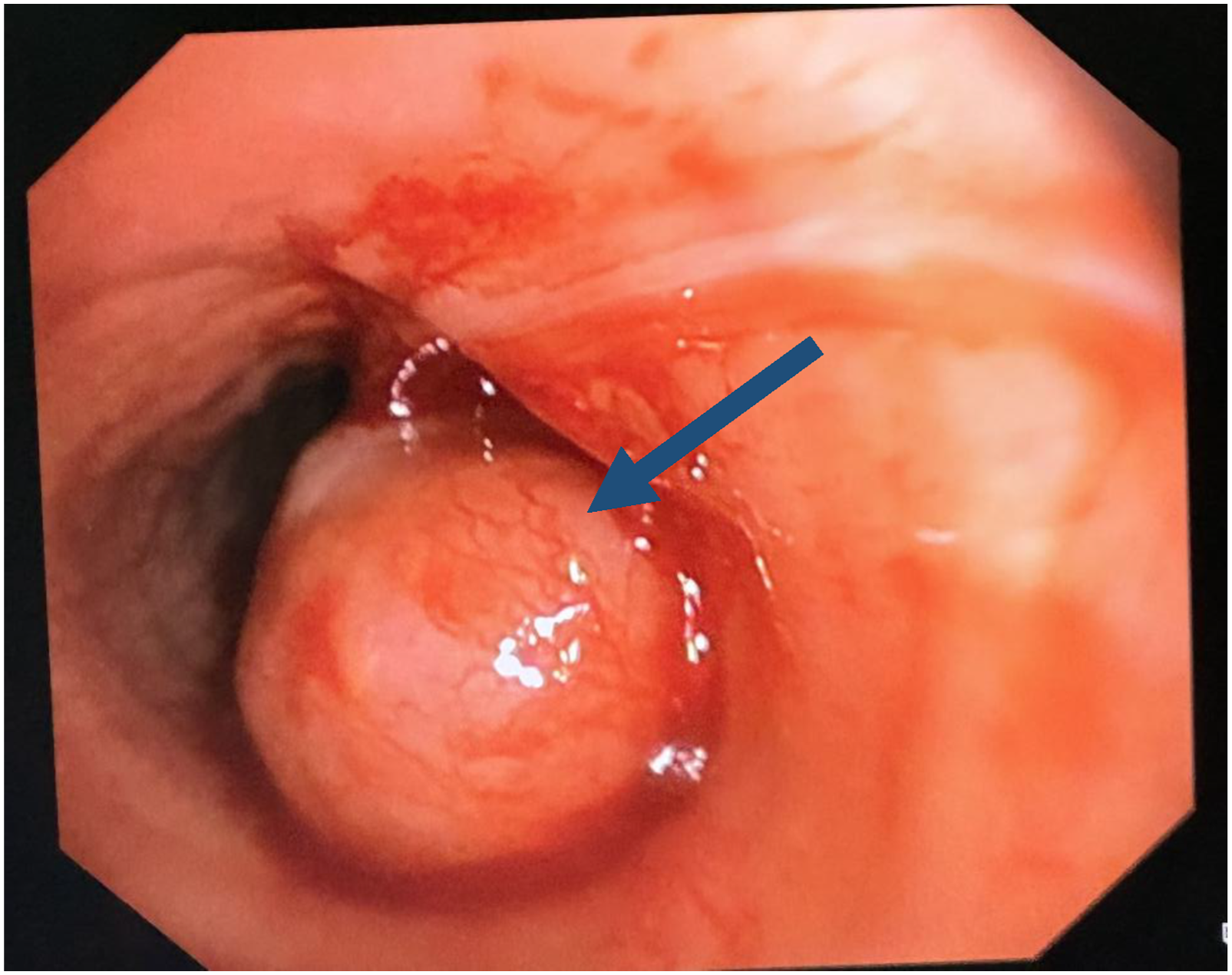
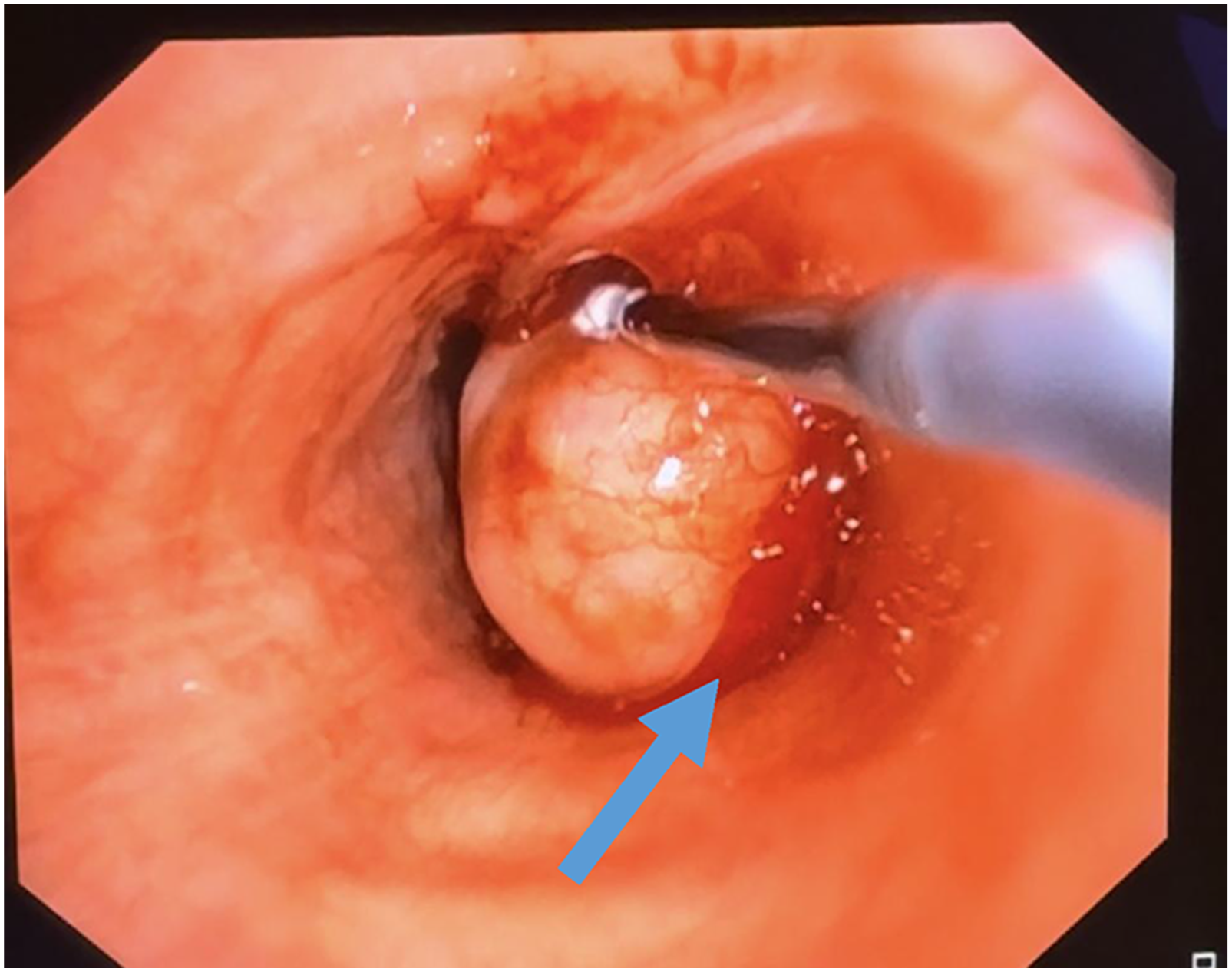
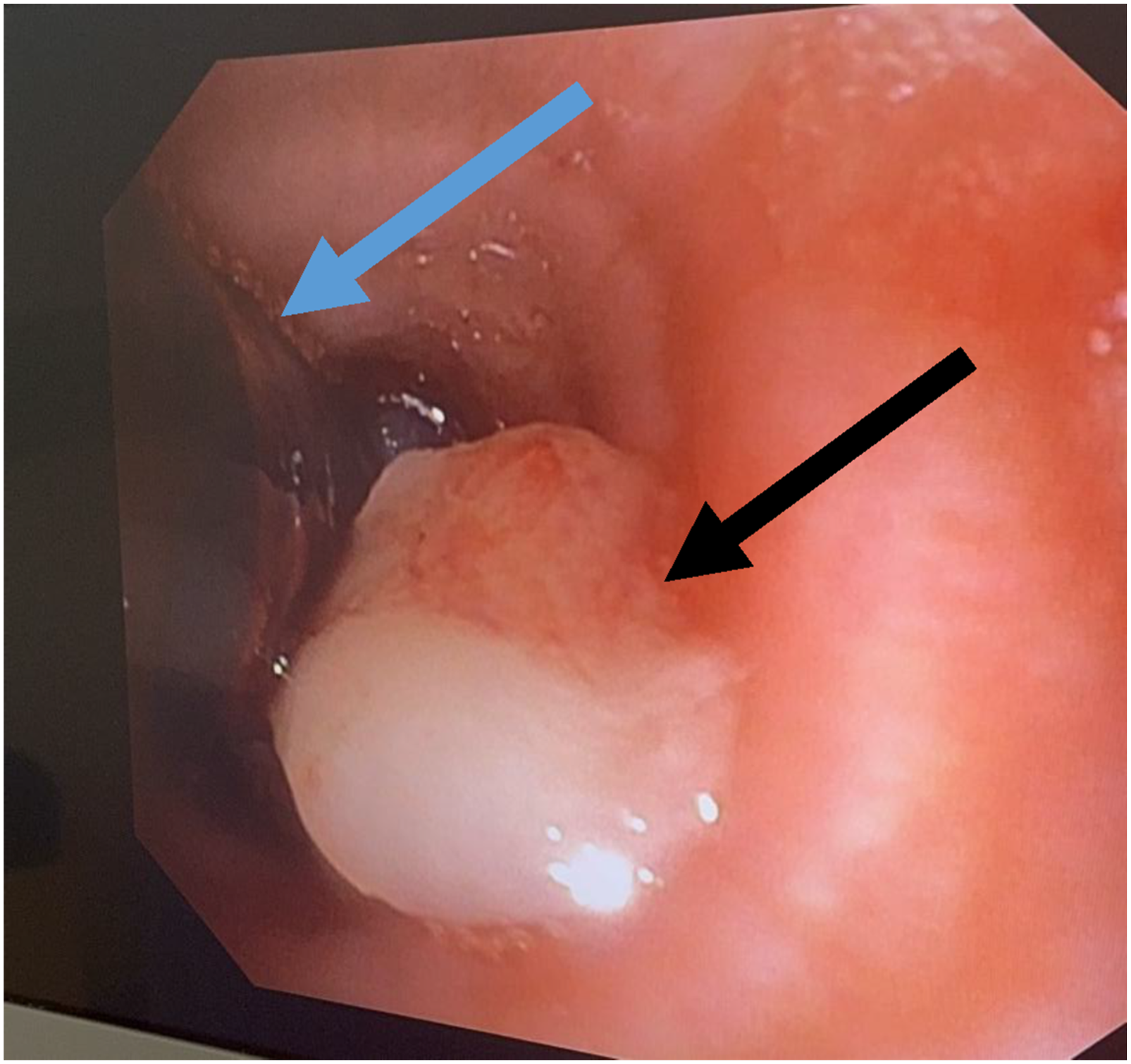
A 45-year-old female patient presented to our pulmonary clinic with progressive stridor, exertional dyspnea, and intermittent hemoptysis Chest computed tomography (CT) demonstrating the intratracheal mass. (A–B) Axial CT images showing a well-defined intraluminal tracheal mass causing near-complete airway obstruction (white arrows) with associated right lung lobar collapse. (C) Lower axial CT section demonstrating the distal extent of the lesion, located approximately one tracheal cartilage ring above the carina (black arrow) Bronchoscopic view of the distal trachea showing the tumor located approximately 1–2 tracheal cartilage rings above the carina (white arrow) Bronchoscopic view showing a large, smooth-surfaced, and highly vascularized intratracheal tumor (blue arrow) with more than 80% obstruction of the tracheal lumen Bronchoscopic view showing active bleeding from the tumor (blue arrow) with associated bronchospasm and airway narrowing during cryotherapy Bronchoscopic view demonstrating placement of a small-diameter endotracheal tube (blue arrow) distal to the tumor (black arrow) to restore airway patency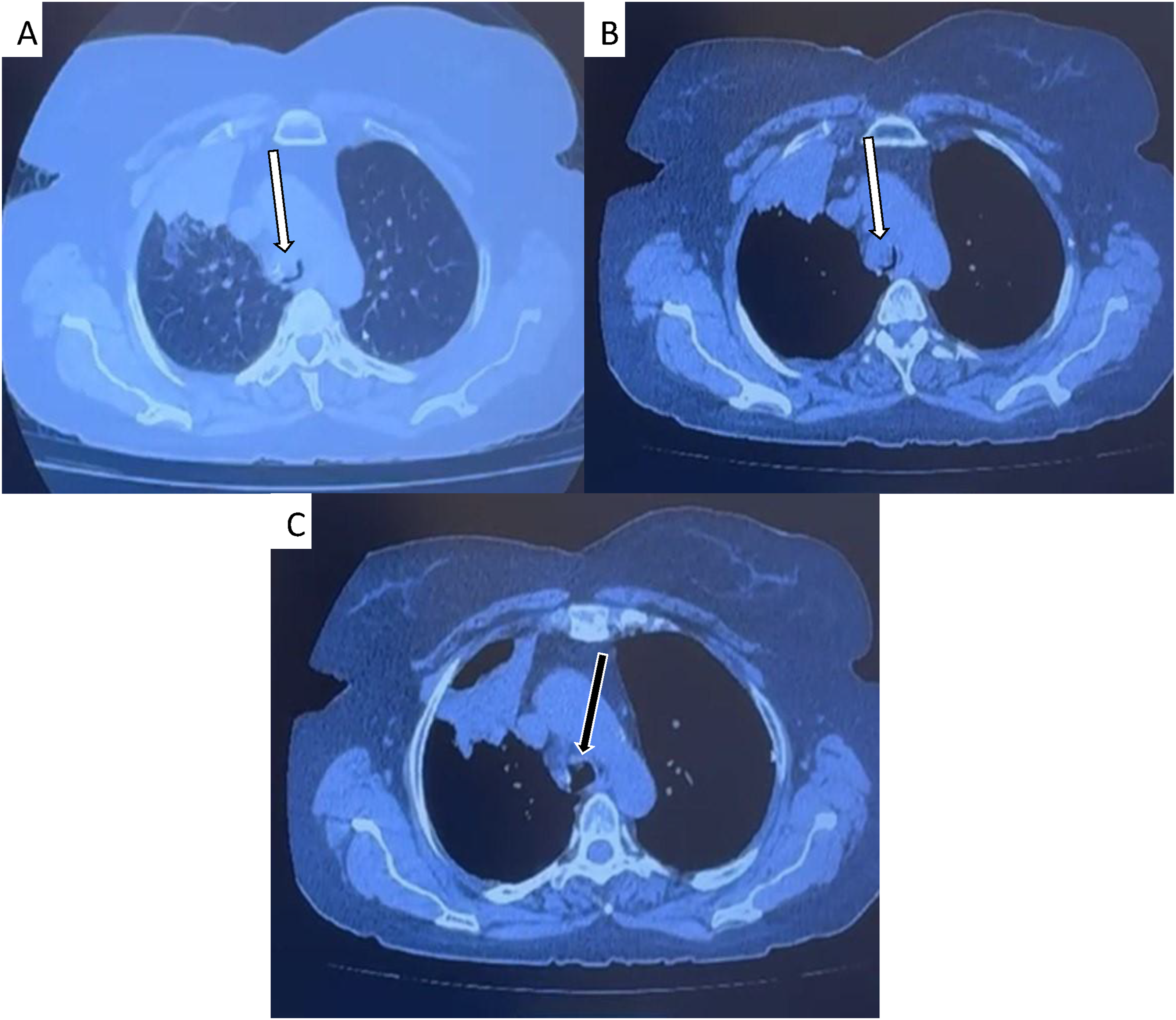
Discussion
Pleomorphic adenoma is a benign mixed tumor composed of epithelial, myoepithelial, and mesenchymal components and is classically associated with the salivary glands, the parotid and submandibular glands. Its occurrence in the tracheobronchial tree is exceedingly rare, accounting for a small minority of salivary gland–type airway tumors. It may also develop in atypical locations, including the nasal cavity, paranasal sinuses, hypopharynx, pharynx, larynx, trachea, and lacrimal glands. In a large single-institution series spanning 34 years, pleomorphic adenoma represented only 1.8% of primary tracheobronchial salivary gland–type tumors, markedly less frequent than adenoid cystic and mucoepidermoid carcinomas.1,6 Clinically, tracheal pleomorphic adenomas often present with nonspecific and slowly progressive respiratory symptoms, including wheezing, cough, and dyspnea, frequently leading to misdiagnosis as bronchial asthma. Symptom duration may be prolonged, with reported cases extending over several years prior to diagnosis. As a result, diagnosis is commonly delayed until imaging or bronchoscopy is performed for persistent or refractory symptoms. 1 Histologically, pleomorphic adenoma is termed a “mixed tumor” due to its heterogeneous architecture rather than a true dual epithelial–mesenchymal origin. The stroma may be mucoid, myxoid, cartilaginous, or hyaline, and malignant transformation to carcinoma ex pleomorphic adenoma occurs in approximately 6% of cases. Immunohistochemically, the tumor typically expresses cytokeratins, p63, S-100 protein, epithelial membrane antigen, and glial fibrillary acidic protein, with S-100 and glial fibrillary acidic protein aiding in differentiation from adenoid cystic carcinoma. 7 This case is unique in that it describes a pleomorphic adenoma located in the distal trachea immediately proximal to the carina, complicated by acute airway collapse during cryotherapy, thereby highlighting the combined challenges of tumor location, airway control, and procedural risk in a setting where conventional rescue strategies such as tracheostomy are not feasible. Intratracheal tumors are exceedingly rare, accounting for approximately 0.2% of all respiratory tract tumors, and may be either primary or secondary in origin.8,9 Although central airway obstruction is typically considered significant at greater than 50% luminal narrowing, clinically relevant dyspnea usually occurs only when narrowing exceeds 70%. Malignant central airway obstruction (MCAO) can be classified as intrinsic, extrinsic, or mixed. Intrinsic tumors originate within the airway lumen and often allow airway patency to be restored using ablative therapies or mechanical debulking techniques. Extrinsic obstruction, caused by external compression, typically requires stent placement, whereas mixed obstruction often necessitates a combination of ablative therapy and stenting. 4
Surgical resection remains the definitive treatment when the diagnosis is confirmed, respiratory status is stable, and complete excision is feasible. However, in the setting of critical airway obstruction, transbronchial biopsy and immediate surgery may pose significant risk. In such cases, endoscopic airway management to restore patency and obtain a definitive histological diagnosis represents a safer initial strategy. While carinal resection with reconstruction is among the most technically challenging thoracic procedures and carries substantial morbidity and mortality, bronchoscopic interventions have become widely adopted for airway stenosis. Endobronchial techniques have been successfully used for resection of tracheal pleomorphic adenoma, offering a less invasive alternative with shorter recovery times and serving as definitive or palliative treatment in patients who are poor surgical candidates or decline surgery.1,9,10 Cases of tracheal pleomorphic adenoma with severe airway obstruction, successfully treated with bronchoscopic intervention have been reported.1,6 In a review of 11 cases of tracheal pleomorphic adenomas, bronchoscopic interventions were mostly used in middle and upper trachea tumor, while surgical intervention was chosen for distal tumors. 1 In another case, intratracheal pleomorphic adenoma was resected using electron bronchoscopy, cryotherapy and APC without significant bleed or perforation. 7 Inomata et al, report a case of tracheal pleomorphic adenoma successfully managed with complete tumor removal, carinal resection with tracheal reconstruction as the tumor was located immediately proximal to the carina. Venovenous extracorporeal membrane oxygenation (VV-ECMO) was initiated to ensure adequate oxygenation during the procedure. 9 Only a limited number of cases of tracheal pleomorphic adenoma have been reported in the literature. Most tumors arise in the upper or middle trachea and are commonly managed either by surgical resection or bronchoscopic intervention. In previously reported cases, bronchoscopic techniques such as electrocautery, laser therapy, or cryotherapy have been successfully used to achieve tumor debulking and restore airway patency. However, tumors located in the distal trachea close to the carina are less frequently described and present additional technical challenges because of the difficulty in securing the airway and maintaining adequate ventilation during intervention.
Among endobronchial ablative therapies, cryotherapy has emerged as a widely used modality because it induces tumor destruction through repeated freezing and thawing cycles while preserving surrounding cartilage and connective tissue.4,11 This extreme cold induces cell death through multiple mechanisms, including intracellular and extracellular ice crystal formation, microvascular thrombosis leading to tissue ischemia.2,4 Cryotherapy selectively targets cryosensitive tissues, such as vascular tumors and granulation tissue, while cryoresistant structures like cartilage and fibrous tissue remain largely intact, minimizing the risk of airway perforation or long-term stenosis.2,4 Unlike electrocautery and laser therapy, cryotherapy carries no risk of airway fire, eliminating the need to reduce inspired oxygen concentrations during the procedure. Large solid tumors (>1 cm) and diffuse metastatic disease are not ideal candidates for cryotherapy. 12
Tumors located near the carina represent a particularly challenging subset of intratracheal lesions. In this region, airway control can be difficult because advancing an endotracheal tube beyond the lesion may not be feasible, and tracheostomy may not provide access distal to the obstruction. Furthermore, manipulation of tumors in this location may rapidly compromise ventilation by causing bleeding, edema, or displacement of the lesion into the airway lumen. For these reasons, procedures involving near-carinal tumors require careful planning and close coordination between interventional pulmonologists, anesthesiologists, and thoracic surgeons.
Several studies have demonstrated the efficacy and safety of cryotherapy in the management of central airway tumors. In a retrospective cohort of 63 patients, cryotherapy achieved complete remission in 33% of tumors smaller than 20 mm and enabled parenchymal-sparing treatment in a substantial proportion of larger lesions, with symptomatic improvement reported in over 90% of patients and only minor self-limited complications such as transient cough with blood-stained sputum. 2 Similarly, endobronchial therapy has shown favorable outcomes in patients with airway tumors, including carcinoid lesions, with high rates of tumor removal and good long-term survival without significant differences compared with surgical management in selected cases. 13 Larger retrospective analyses have also demonstrated high rates of airway recanalization with bronchoscopic cryodebridement, achieving airway patency in up to 95% of cases with relatively low complication rates, most commonly moderate bleeding that can be managed endoscopically. 14 Additional studies of patients undergoing various bronchoscopic interventions for major airway obstruction have reported significant symptomatic improvement and low rates of serious intraoperative complications. 15 In a large retrospective series of 208 patients, risk factors for moderate to severe bleeding during cryotherapy included diabetes mellitus, pre-existing respiratory failure, and distal airway atelectasis, while tumor histology was not associated with increased complication rates. 16
Management of patients with intratracheal tumors requires meticulous planning to secure the airway safely, taking into account tumor location, size, rigidity, and the residual tracheal lumen. For lesions in the upper trachea, options such as tracheostomy under local anesthesia or placement of a small-diameter intratracheal or laryngeal mask airway may be considered to avoid trauma to the mass. 5 However, tumors near the carina pose additional challenges, including the risk of one-lung ventilation, difficult tracheostomy, and the need for sternotomy under general anesthesia. In such cases, a tubeless approach with apneic oxygenation using high-flow nasal oxygen (HFNO) can be safely employed if upper airway patency is maintained. 5 Alternative approaches, such as advancing a microlaryngeal tube beyond the mass under fiberoptic guidance or positioning the tube above the lesion, carry risks of mass dislodgement, bleeding, and impaired ventilation. Another method is to place the tip of the plain tube ID 6.0 above the mass. In this regard, the laryngeal mask airway can also be used. In selected high-risk cases with severe airway obstruction, extracorporeal support strategies such as extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass may be required to maintain adequate oxygenation during airway procedure.3,5
Directing the tracheal intubation in patients with intratracheal tumors may precipitate hemorrhage, tumor fragmentation, or sudden airway obstruction. Various airway strategies have therefore been described, including laryngeal mask airway ventilation, tracheostomy distal to the lesion, and high-frequency jet ventilation. However, each approach carries potential risks such as barotrauma, inadequate ventilation, or tumor displacement, emphasizing the importance of individualized airway planning in patients with critical airway obstruction.8,15
In the present case, airway deterioration was likely the result of a rapid, self-amplifying sequence of events. The tumor’s marked vascularity predisposed to bleeding upon manipulation, which in turn impaired bronchoscopic visualization and limited effective suctioning. At the same time, cryotherapy-induced tissue edema and reflex bronchospasm further reduced the already critically narrowed airway lumen. Importantly, the lesion’s location immediately proximal to the carina created a uniquely high-risk situation, as even minimal reductions in luminal diameter or slight displacement of the endotracheal tube can critically impair ventilation to both main bronchi. In this context, loss of optimal tube positioning likely contributed significantly to the sudden ventilatory compromise. This case illustrates how, in near-carinal lesions, airway instability can evolve rapidly due to the interaction between bleeding, edema, bronchospasm, and mechanical factors, leaving very limited margin for compensation during endobronchial interventions. The patient required prompt stabilization with adrenaline boluses and systemic corticosteroids. After stabilization, the airway was re-entered under direct visualization, and ventilation was restored using a small-diameter endotracheal tube with selective intubation, allowing completion of the procedure. In retrospect, the initial management approach in this case may be reconsidered in light of the tumor’s location and vascular characteristics. A staged strategy, beginning with a limited diagnostic biopsy under high-flow nasal oxygen (HFNO) without immediate tumor ablation, may have reduced the risk of bleeding and acute airway compromise by minimizing early manipulation of the lesion.
Rigid bronchoscopy represents another potentially advantageous approach in this setting, as it provides superior airway control, facilitates rapid mechanical debulking, and allows more effective management of bleeding through tamponade. In the context of a near-carinal lesion with limited airway reserve, this may offer a more controlled environment compared with flexible bronchoscopy. Additionally, advanced oxygenation strategies such as extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass have been described in similar high-risk airway cases, providing a safety margin during complex interventions. Although these modalities were not available in our institution, their use could be considered in comparable scenarios where severe airway compromise is anticipated. Taken together, these considerations suggest that for distal tracheal tumors located near the carina, a more cautious and staged approach, or the use of techniques that provide greater airway control, may reduce procedural risk. Cryotherapy was selected as a bronchoscopic modality due to its tissue-sparing properties, preservation of cartilaginous structures, and lower risk of airway perforation compared with thermal techniques such as laser or electrocautery. In addition, the absence of ignition risk allows its use without reducing inspired oxygen concentration, which is advantageous in patients with compromised respiratory reserve. However, this case underscores that the perceived safety profile of cryotherapy does not eliminate the risk of acute airway compromise, particularly in highly vascular lesions located in anatomically critical regions such as the distal trachea. Procedural risk is therefore determined not only by the modality itself but also by tumor characteristics and location. Despite these advantages, manipulation of the tumor in this case resulted in bleeding and bronchospasm, leading to acute airway compromise. From a practical standpoint, this case emphasizes that near-carinal airway lesions should be approached as high-risk scenarios, even when minimally invasive techniques are planned. Pre-procedural identification of rescue strategies, maintenance of spontaneous ventilation during initial airway assessment, and readiness to rapidly transition to alternative airway control methods are critical to preventing catastrophic outcomes.
This report has several limitations. First, as a single case report, the findings are not generalizable and primarily serve to highlight potential challenges rather than establish optimal management strategies. Second, the absence of advanced airway support modalities such as extracorporeal membrane oxygenation (ECMO) limited the range of procedural options and may have influenced both the choice of intervention and the intraoperative risk profile. Third, although the intraoperative complication was clearly documented, it was not possible to definitively distinguish the relative contributions of bleeding, bronchospasm, and mechanical obstruction to the airway collapse, which may limit mechanistic interpretation. Finally, long-term follow-up data are limited, precluding assessment of recurrence risk, need for repeat intervention, and long-term airway outcomes. Despite these limitations, the case provides important practical insights into airway management challenges in near-carinal tracheal tumors.
Conclusion
This case illustrates the significant challenges posed by distal tracheal pleomorphic adenoma located near the carina, particularly regarding airway management and endoscopic treatment. The patient’s presentation with stridor, dyspnea, and hemoptysis, combined with the tumor’s critical location, made endotracheal intubation difficult and precluded tracheostomy as a rescue option. During cryotherapy, manipulation of the tumor resulted in complete airway obstruction and collapse, bronchospasm, and bleeding, highlighting the potential for life-threatening complications even with minimally invasive interventions. Successful management of similar cases requires meticulous pre-procedural planning, a multidisciplinary approach involving anesthesiology, pulmonology, otolaryngology, and thoracic surgery, and readiness to employ advanced airway strategies such as rigid bronchoscopy, jet ventilation, or extracorporeal support when necessary. This report underscores the importance of anticipating procedural risks based on tumor location and reinforces that airway safety should remain the highest priority in the treatment of central airway tumors.
Footnotes
Ethical Considerations
Case reports are exempted from ethical approval at our institution.
Consent to Participate
A signed written informed consent was obtained from the patient prior to manuscript submission.
Author Contributions
Conceptualization, Antonio Al Hazzouri; writing—original draft preparation, Antonio Al Hazzouri, Maya Hneidi, Philippe Attieh, Katherine Atallah, Kaity Saliba, Pierre Mourad; writing—review and editing, Antonio Al Hazzouri, Maya Hneidi, Philippe Attieh, Katherine Atallah, Kaity Saliba, Pierre Mourad; supervision, Pierre Mourad; project administration, Pierre Mourad. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon request from authors.