
Abstract
Introduction
Metronidazole-induced encephalopathy (MIE) is an under-recognised but potentially reversible neurotoxic complication of metronidazole therapy, typically associated with high cumulative doses or underlying comorbidities such as hepatic dysfunction. Classic MRI findings include symmetric T2/FLAIR hyperintensities in the cerebellar dentate nuclei, brainstem, and splenium of the corpus callosum.
Case Presentation
We report a 64-year-old woman with well-controlled hypertension and type 2 diabetes who developed acute dysarthria, gait instability, and a generalized seizure after a 7-day course of metronidazole totaling 10.5 g. Laboratory evaluation was unremarkable.Stool cultures and pathogen-specific PCR were negative. The MRI shows bilateral symmetric T2/FLAIR hyperintensities in the dentate nuclei, brainstem, and splenium, consistent with MIE. No alternative etiology was identified. This case occurred in an adult without hepatic dysfunction. Metronidazole was discontinued immediately, leading to rapid clinical improvement and complete neurological recovery.
Conclusion
This case highlights that MIE can occur even after short treatment durations and low cumulative doses, particularly in patients without traditional risk factors. Early recognition of the clinical and radiologic features is essential, as prompt drug cessation leads to full reversibility in most cases.
Keywords
Introduction
Metronidazole is a widely used nitroimidazole antibiotic for anaerobic and protozoal infections and is also employed in hepatic encephalopathy and Crohn’s disease. 1 While generally well-tolerated, its adverse effects can involve the central nervous system. Neurological toxicity manifests as cerebellar dysfunction (ataxia, dysarthria), seizures, altered mental status, hallucinations, and encephalopathy. These features are collectively termed metronidazole-induced encephalopathy (MIE).1,2 MIE is under-recognised, with an incidence not clearly established, and can occur after both short-term and prolonged therapy.1-3 Most reported cases involve high cumulative doses (often tens of grams) over weeks, especially in patients with risk factors like hepatic dysfunction or alcohol usje.2,4 Neuroimaging (brain MRI) typically shows bilateral T2/FLAIR signal abnormalities, most frequently localized to the dentate nuclei of the cerebellum, the brainstem, and the splenium.3,4
Herein, we report a case of MIE in a 64-year-old woman with no apparent risk factors who developed acute ataxia, dysarthria, and seizure after only a 7-day course (10.5 g total) of metronidazole. This presentation is less commonly recognised at such a low cumulative dose and shorter duration than typical case series (mean ∼58.1 g over ∼39 days), and in the absence of hepatic dysfunction or other comorbidities. To our knowledge, MIE under such low-dose, short-term exposure is under-recognised in the literature. We highlight the diagnostic features and full reversibility of this case, underscoring the need for awareness of MIE even in patients without classic risk factors.1-4
Case Report
A 64-year-old female with a past medical history of hypertension and diet-controlled type 2 diabetes mellitus presented to the emergency department with a 3-day history of vomiting, abdominal cramping, and diarrhea. She was diagnosed with acute gastroenteritis and started on oral metronidazole 500 mg three times daily for a presumed anaerobic infection. Stool cultures and multiplex PCR for common bacterial enteropathogens (including C. difficile, Salmonella, Shigella, and Campylobacter) were negative. Her only chronic medications were metformin 500 mg twice daily and amlodipine 5 mg once daily; she was not taking proton pump inhibitors, diuretics, or other medications known to interact with metronidazole or lower seizure threshold. She improved symptomatically over the next week.
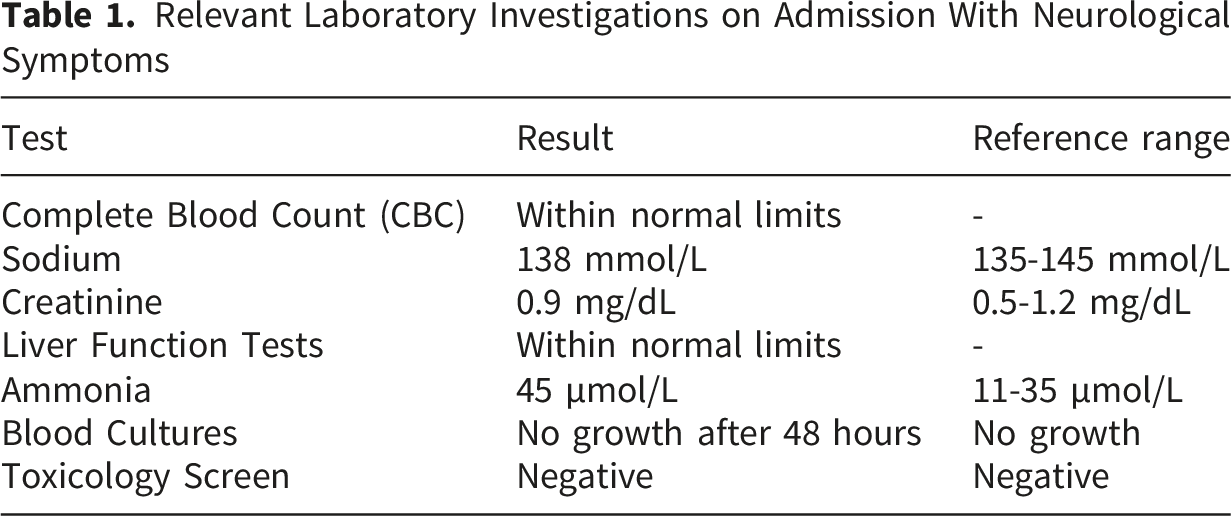
Relevant Laboratory Investigations on Admission With Neurological Symptoms
However, one week after initiation of therapy, she acutely developed slurred speech (dysarthria), gaze-evoked nystagmus, bilateral dysmetria on finger-to-nose and heel-to-shin testing, a positive Romberg sign, and a wide-based, unsteady gait and experienced a single generalized tonic-clonic seizure. The seizure was witnessed by a family member and lasted approximately 90 seconds, with urinary incontinence and a postictal confusional state of approximately 20 minutes. No focal semiology was observed. This was followed by a progressive decline in her level of consciousness. There was no history of fever, head trauma, or meningeal signs. Her family denied any illicit drug use or access to other neurotoxic substances.
Given the acute neurological deterioration, stroke and meningoencephalitis were the primary considerations. An urgent non-contrast Computed Tomography (CT) scan of the brain was unremarkable, ruling out a large acute hemorrhage or infarct.
Brain MRI (obtained within 24 hours of seizure onset) showed bilateral hyperintense lesions on T2/FLAIR sequences involving the cerebellar dentate nuclei, midbrain, and splenium, in keeping with metronidazole - induced encephalopathy. These lesions exhibited restricted diffusion on diffusion-weighted imaging, with corresponding low ADC values consistent with cytotoxic edema. No contrast enhancement or mass effect was observed (Figure 1). Axial T2/FLAIR MRI demonstrating bilateral symmetric hyperintensities in the dentate nuclei (arrowheads). Axial brain MRI demonstrating findings consistent with metronidazole-induced encephalopathy. FLAIR images show bilateral, symmetric hyperintense signal involving the cerebellar dentate nuclei and the dorsal pons (A). Diffusion-weighted imaging reveals corresponding areas of restricted diffusion (B) with low apparent diffusion coefficient (ADC) values (C), indicating cytotoxic edema. No contrast enhancement or mass effect is observed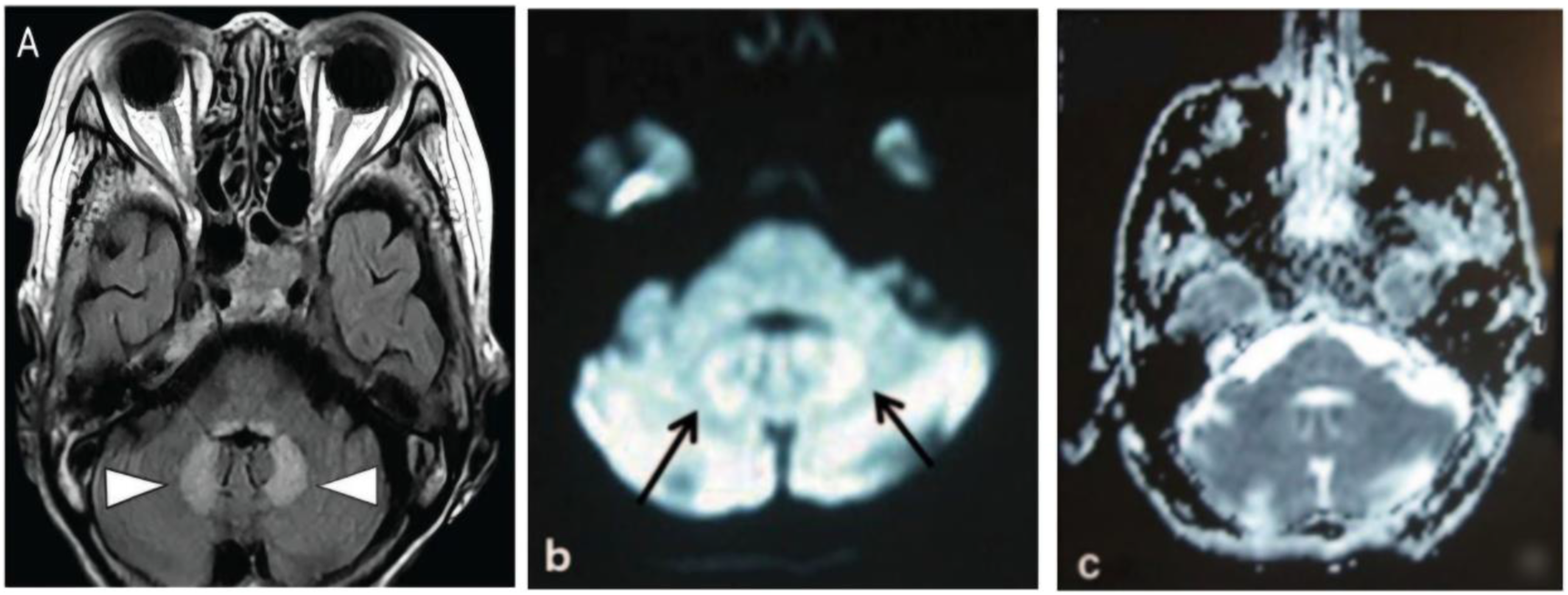
A meticulous review of her medication history confirmed metronidazole as the only potential neurotoxic agent, with a cumulative dose of approximately 10.5 grams over one week. A diagnosis of metronidazole-induced encephalopathy was made. The drug was immediately discontinued. The patient’s neurological symptoms began to resolve within 72 hours. She was managed supportively, and due to the rapid and complete resolution of her motor and cerebellar symptoms, a formal course of physical or speech therapy was not deemed necessary.
Clinical Timeline, Neurological Onset, and Management of Metronidazole-Induced Encephalopathy
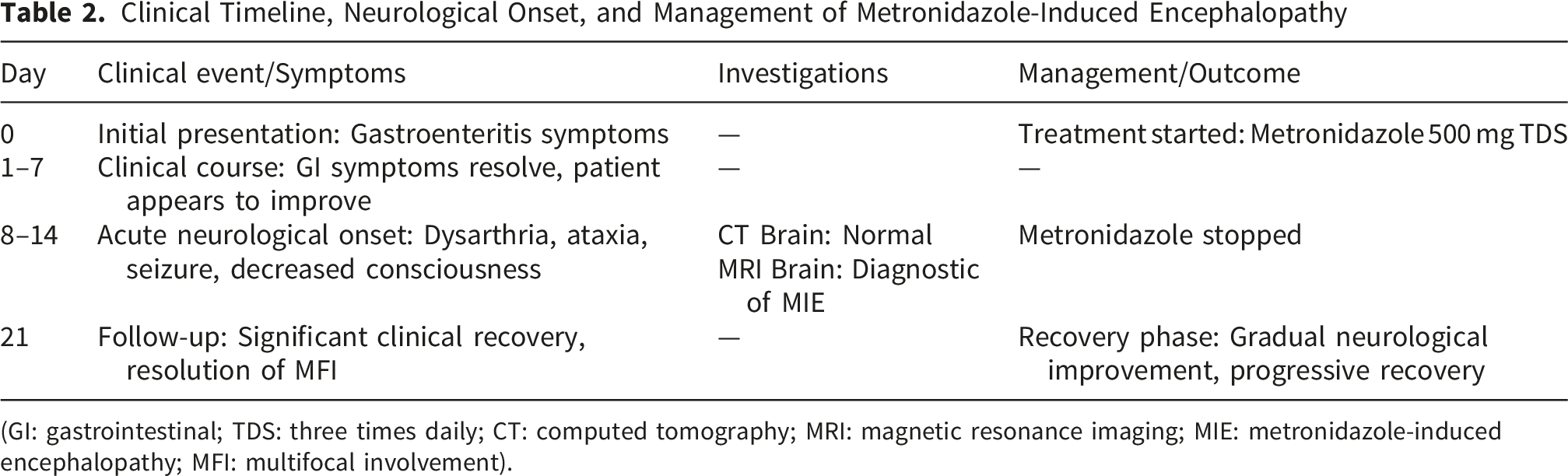
(GI: gastrointestinal; TDS: three times daily; CT: computed tomography; MRI: magnetic resonance imaging; MIE: metronidazole-induced encephalopathy; MFI: multifocal involvement).
The patient reported significant distress during the acute neurological decline but expressed relief at the rapid improvement following discontinuation of metronidazole. She emphasized gratitude for the timely diagnosis and complete recovery, noting restored confidence in her daily functioning.
Discussion
This case illustrates several notable aspects of MIE. First, the cumulative dose (10.5 g) and exposure (7 days) were lower than usually reported. In a large series, affected patients typically received approximately 58 g of metronidazole over a period of 39 days. 4 Likewise, most patients have predisposing conditions (liver disease being most common). 2 Our patient had no significant comorbidity besides well-controlled diabetes and hypertension. Although rare cases of MIE have been reported after relatively short courses (especially in liver disease), its occurrence in a healthy adult at such a low dose is under-recognised; similar cases have been reported only infrequently, suggesting potential diagnostic under-reporting4,5 This emphasizes that clinicians should consider MIE even after brief or standard-dose therapy when neurological symptoms arise.
We conducted a literature review of “metronidazole encephalopathy” and related terms, focusing on case reports with short treatment courses or low cumulative doses. The majority of reported cases of MIE occur after substantially higher cumulative doses than observed in our patient, with systematic reviews reporting mean cumulative exposures ranging from approximately 58 g to 125 g, although rare cases have been described at doses as low as 5 g. A case series reported a median cumulative dose of 64.5 g with a wide range extending from 7.5 g to 1380 g, highlighting that MIE may occur even after short treatment durations and suggesting that its development is not strictly dose dependent. 6
Comparison of Previously Reported Low-Dose or Short - Duration Metronidazole - Induced Encephalopathy Cases in Adults and the Present Case
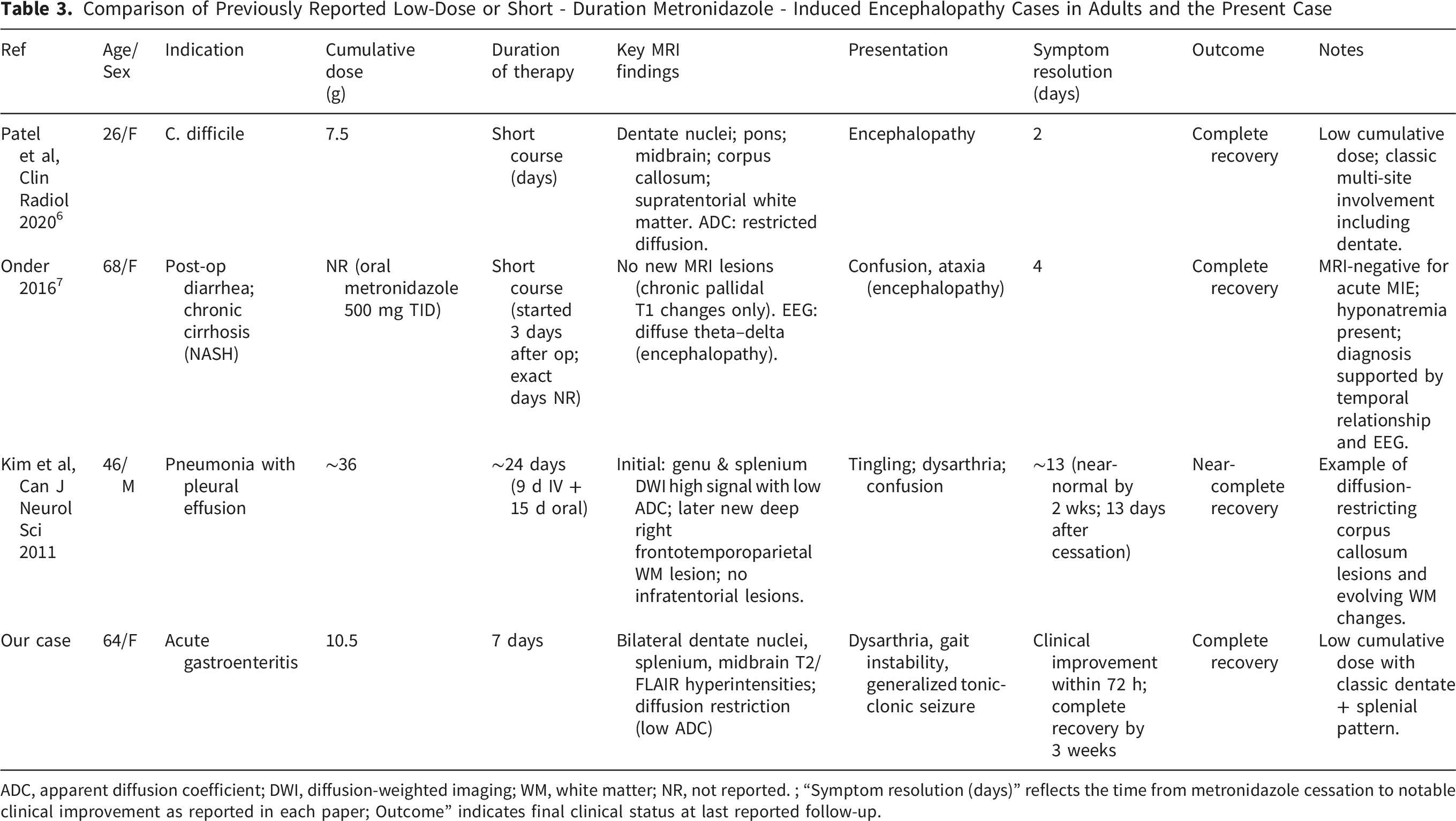
ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; WM, white matter; NR, not reported. ; “Symptom resolution (days)” reflects the time from metronidazole cessation to notable clinical improvement as reported in each paper; Outcome” indicates final clinical status at last reported follow-up.
Aside from the three cases above, we found very few reports of similarly low-dose, short-course MIE. Notably, one pediatric case described encephalopathy after just 3 g over 2 days (though pediatric metabolism differs). The scarcity of such reports underscores that low-dose MIE remains under-recognised in clinical practice. The few analogous adult cases all had underlying pathology, which our patient lacked, making direct comparisons difficult. 9
Consistent with prior reports, our patient presented with acute cerebellar dysfunction (dysarthria, gait instability) and a seizure. These features align with the most common symptoms of MIE. We considered other causes (stroke, infection, Wernicke’s, metabolic encephalopathy) which were excluded by imaging and labs. The close temporal relationship to metronidazole use and lack of alternative explanation pointed to MIE. 10 The MRI in our case showed exactly the classic pattern: symmetric T2/FLAIR hyperintensities in bilateral dentate nuclei, with additional lesions in the splenium and midbrain. This matches the prototypical MIE distribution. The dentate nuclei are almost invariably involved in MIE, and splenial lesions are commonly reported as well. Our observation of diffusion restriction (low ADC) in the splenial lesion is also described in the literature as indicating cytotoxic edema in white-matter areas. The imaging pattern strongly supports the diagnosis of MIE over other etiologies.4,10
Seizures are an established but relatively uncommon manifestation in MIE, reported in approximately 10–15% of cases. 1 In our patient, the occurrence of a generalized tonic–clonic seizure is most plausibly attributable to the cerebellar involvement demonstrated on MRI. The bilateral dentate nuclei were markedly affected, and the cerebellum normally provides a tonic inhibitory influence on cortical excitability. 11 Cytotoxic injury to the dentate nuclei may therefore disrupt this inhibitory control, resulting in cortical disinhibition and a reduced seizure threshold. Supporting this mechanism, both experimental and clinical evidence indicate that epileptiform activity can originate from intrinsic cerebellar pathology.11,12 Boop et al, for example, recorded seizures arising directly from cerebellar tumors in patients. 12 In contrast, the midbrain and splenial lesions in our patient – while characteristic of MIE – are not known to directly generate convulsive seizures. Thus, loss of cerebellar inhibition due to dentate nucleus edema most plausibly underlies the seizure, whereas the other lesions contributed to her encephalopathy and altered consciousness.
The patient’s full recovery after stopping metronidazole is in line with published outcomes. Systematic reviews show that most patients improve within days to weeks of drug withdrawal. Radiologic improvement usually follows clinical recovery. In fact, only a small minority (∼4%) have lasting deficits. Our patient’s rapid resolution reinforces the importance of early recognition: continued metronidazole could have led to irreversible damage, whereas prompt cessation led to complete recovery.1,4,10
Conclusion
Metronidazole-induced encephalopathy can occur even after short courses and low cumulative doses, as demonstrated in this case. Prompt recognition of the characteristic clinical and MRI findings and immediate discontinuation of the drug are essential to ensure full neurological recovery. Clinicians should remain vigilant for MIE in any patient who develops new neurological symptoms while receiving metronidazole, regardless of dose or risk factors.
Footnotes
Ethical Considerations
Ethical approval was not required for this case report, as it involves a single patient and does not meet the criteria for research requiring institutional review board (IRB) oversight. The use of authorized medications was consistent with clinical practice guidelines, and the management of this individual patient did not require IRB approval.
Consent to Participate
Written informed consent was obtained from the patient prior to publication of this case report and any accompanying images. The completed consent form is available to the Editor upon request and will be treated confidentially.
Author Contributions
1. Mohammad Adi: Data Curation, Formal Analysis, Writing, Writing - Original Draft, Review and Editing, Contributions to Discussion.
2. Shaza Mostafa: Methodology, Data Interpretation, Approval of Final Manuscript, Supervision.
3. Javdat Latipov: Writing – Review & Editing.
4. Otabek Kuziev: Writing.
5. Ahmed Ashraf: critically reviewed the manuscript and contributed to the final revision.
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data pertinent to this case report have been included in this article. Further inquiries can be directed to the corresponding author.