
Abstract
Introduction
Infectious diseases exert systemic effects beyond localized inflammation, yet selective disruption of host metabolic pathways remains incompletely characterized. Carnitine-dependent fatty-acid transport is essential for mitochondrial energy production, and acquired deficiencies are rarely attributed to infection. Chronic bacteremia has not been clearly linked to functional impairment of this pathway.
Case Presentation
A 34-year-old man with no prior metabolic or neuromuscular disease presented with subacute proximal muscle weakness, fasting intolerance, and episodic confusion following several weeks of constitutional symptoms. Evaluation demonstrated hypoketotic hypoglycemia (plasma glucose 46–54 mg/dL with β-hydroxybutyrate <0.3 mmol/L), elevated creatine kinase (peak 2,140 U/L), and reduced plasma free carnitine (12 μmol/L; reference 25–50 μmol/L), indicating impaired mitochondrial fatty-acid transport. Serial blood cultures isolated Achromobacter xylosoxidans, confirming persistent bacteremia. Alternative endocrine, metabolic, and immunologic causes were excluded.
Discussion
Resolution of metabolic abnormalities following targeted antimicrobial therapy supports an acquired and reversible disruption of fatty-acid transport. Potential mechanisms include inflammation-mediated renal carnitine loss and host–pathogen metabolic competition during prolonged bacteremia.
Conclusion
Chronic Achromobacter xylosoxidans bacteremia may be associated with reversible secondary carnitine deficiency and selective impairment of fatty-acid transport. Plasma free carnitine normalized after antimicrobial therapy and short-term L-carnitine supplementation, with no recurrence during six months of follow-up. Metabolic evaluation should be considered in patients with unexplained hypoketotic hypoglycemia and persistent bloodstream infection.
Introduction
Metabolic homeostasis during infection is maintained through coordinated interactions between immune activation, substrate availability, and mitochondrial function. 1 While acute infections frequently induce transient insulin resistance or hypercatabolism, 2 sustained disturbances in specific metabolic pathways are uncommon and typically attributed to critical illness or genetic vulnerability. 3 In particular, infection-related perturbation of fatty-acid oxidation has been largely confined to sepsis-associated mitochondrial dysfunction, where impaired oxidative phosphorylation arises secondary to hypoxia, nitric oxide signaling, and inflammatory mediator excess. 4 Outside this context, selective disruption of fatty-acid transport mechanisms has rarely been linked to infectious etiologies.
Carnitine is indispensable for mitochondrial beta-oxidation, acting as a carrier molecule for long-chain fatty acids across the inner mitochondrial membrane via the carnitine shuttle system, which includes carnitine palmitoyltransferase I, carnitine–acylcarnitine translocase, and carnitine palmitoyltransferase II. 5 Acquired carnitine deficiency in adults is most often encountered in the setting of chronic kidney disease, prolonged parenteral nutrition, hepatic insufficiency, or exposure to medications that interfere with renal tubular reabsorption, such as valproate or pivampicillin 6,7. Infectious causes of carnitine depletion are not routinely considered in diagnostic algorithms for hypoketotic hypoglycemia or metabolic myopathy and is not routinely included in current diagnostic frameworks.
Achromobacter xylosoxidans is an aerobic, motile, nonfermenting Gram-negative organism of clinical relevance due to intrinsic resistance mechanisms and persistence in host environments. 8 Although traditionally regarded as a low-virulence pathogen, it can cause chronic bloodstream infection, biofilm formation, and immune evasion, particularly in immunologically intact hosts with indolent exposure sources. 9 Its pathogenic profile has been well characterized in pulmonary and device-associated infections, 10 yet its systemic metabolic impact has not been well characterized. Following the CARE guidelines (for CAse REports), 11 the present case describes a potential association between chronic opportunistic bacteremia and selective impairment of host lipid metabolism and suggests that persistent infection may affect host metabolic pathways beyond organ-specific pathology.
Case Presentation
A 34-year-old man with no prior metabolic, neuromuscular, renal, or endocrine disease presented with subacute symptoms characterized by proximal muscle weakness, early fatigability, and intermittent episodes of confusion occurring predominantly during overnight fasting or delayed meals. He reported six weeks of constitutional symptoms including low-grade fever (maximum recorded 38.1 °C), drenching night sweats, and progressive anorexia, with a documented weight loss of approximately 4 kilograms. There was no recent hospitalization, indwelling vascular access, or illicit drug use, but he had undergone dental extraction eight weeks earlier without antimicrobial prophylaxis. Given the persistence of low-grade fever, constitutional symptoms, and the absence of a clear focal source, serial blood cultures were obtained to evaluate for occult or intermittent bacteremia. Initial cultures drawn at presentation yielded no growth at 48 hours, suggesting low-grade or slow-growing infection. Subsequent cultures obtained during febrile episodes demonstrated consistent growth of Achromobacter xylosoxidans, consistent with the diagnosis of persistent bloodstream infection rather than transient bacteremia. The decision for repeated sampling was based on the clinical suspicion of indolent infection and the known potential for delayed positivity in nonfermenting Gram-negative organisms.
Physical examination revealed low-grade pyrexia, sinus tachycardia (resting heart rate 108 beats/min), and mild orthostatic intolerance. Neuromuscular assessment demonstrated symmetric weakness predominantly affecting hip flexors (Medical Research Council grade 4−/5) and shoulder abductors (4/5), without myalgia, fasciculations, or sensory deficits. Deep tendon reflexes were preserved, and there were no signs of myoglobinuria or rhabdomyolysis-related renal impairment. Cardiopulmonary and abdominal examinations were unremarkable, and no cardiac murmurs or peripheral stigmata of endocarditis were identified.
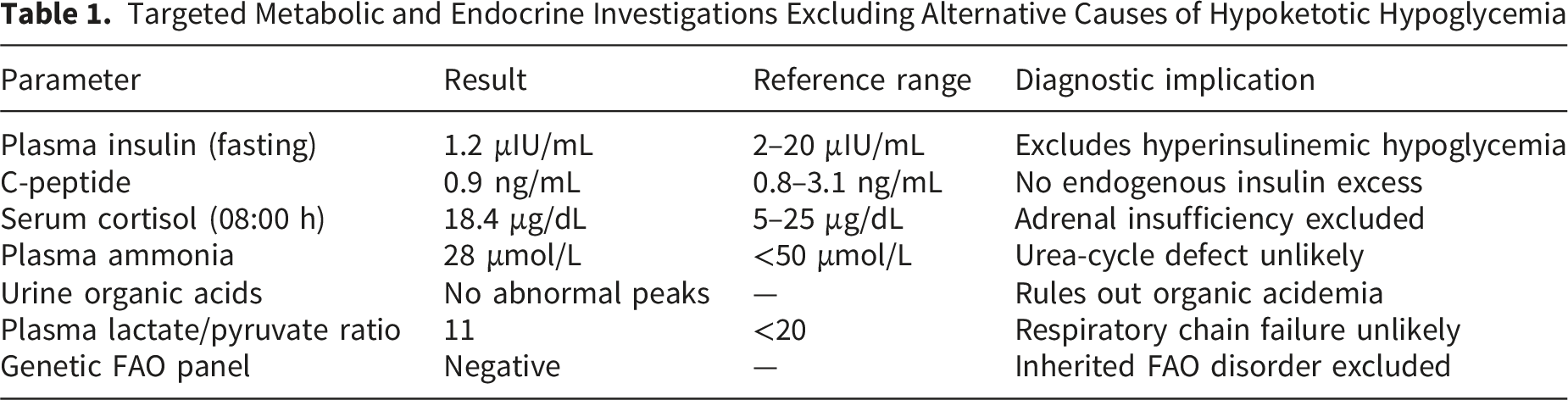
Initial biochemical evaluation identified hypoketotic hypoglycemia during spontaneous fasting (plasma glucose 48 mg/dL with concomitant β-hydroxybutyrate 0.21 mmol/L), accompanied by elevated creatine kinase (2,140 U/L) and mild hepatocellular enzyme elevation (alanine aminotransferase 94 U/L, aspartate aminotransferase 88 U/L) without cholestasis. Serum lactate remained within normal limits (1.2 mmol/L), excluding overt mitochondrial respiratory chain failure. Renal function was preserved, with stable serum creatinine and no tubular proteinuria. Plasma acylcarnitine profiling demonstrated an elevated long-chain acylcarnitine to free carnitine ratio, supporting impaired mitochondrial fatty-acid transport.
Targeted Metabolic and Endocrine Investigations Excluding Alternative Causes of Hypoketotic Hypoglycemia
Antimicrobial Susceptibility Profile and Pharmacodynamic Considerations for Achromobacter xylosoxidans Isolate
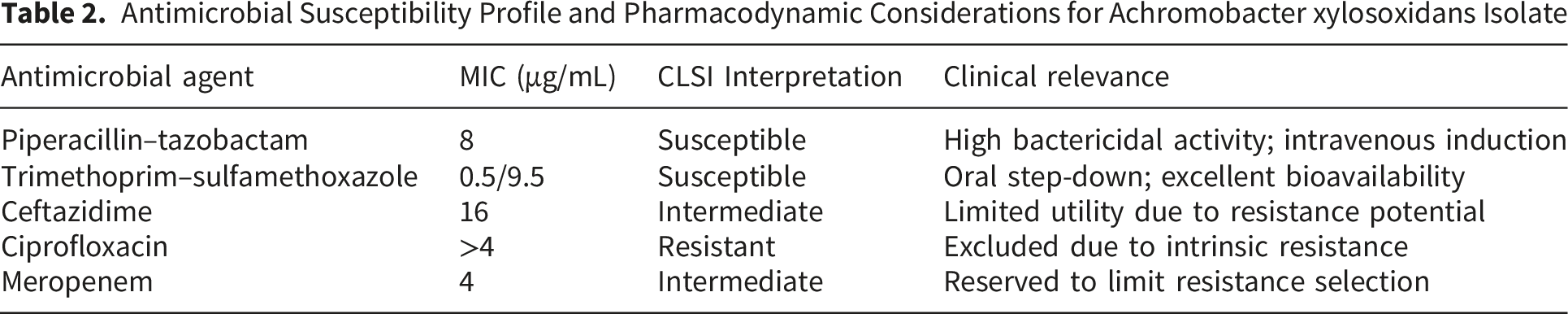
The patient received 14 days of intravenous piperacillin–tazobactam followed by a four-week course of oral trimethoprim–sulfamethoxazole. Adjunctive oral L-carnitine (2 g/day in divided doses) was administered during the acute phase to mitigate ongoing metabolic compromise. Clinical improvement was rapid, with resolution of fasting intolerance within five days and restoration of muscle strength over three weeks. Plasma free carnitine normalized by week four (32 μmol/L), allowing discontinuation of supplementation without recurrence during six months of follow-up.
Discussion
The metabolic phenotype observed in this patient highlights the relationship between chronic infection and mitochondrial substrate utilization. Hypoketotic hypoglycemia accompanied by proximal myopathy is classically associated with defects in fatty-acid transport or oxidation, conditions that are predominantly genetic in origin and typically manifest earlier in life. 12 The adult onset, reversibility, and absence of recurrent symptoms after infection clearance are not consistent with an inherited disorder and instead suggest an acquired, environmentally mediated disruption of fatty-acid handling.
Achromobacter xylosoxidans infection is most frequently described in immunocompromised individuals, particularly those with cystic fibrosis, malignancy, or indwelling medical devices. 9 Chronic pulmonary disease and repeated healthcare exposure are recognized risk factors for colonization and subsequent bacteremia. 13 However, cases in immunocompetent individuals without identifiable predisposing conditions have been reported, often characterized by indolent clinical courses and delayed diagnosis.14-18 In the present case, the absence of immunosuppression or structural lung disease indicates the organism’s capacity for persistence even in otherwise healthy hosts, potentially facilitated by biofilm formation or environmental exposure.
One plausible pathway involves infection-driven modulation of renal carnitine homeostasis. Carnitine balance depends heavily on proximal tubular reabsorption via organic cation transporter novel type 2 (OCTN2). 19 Experimental and clinical studies have shown that inflammatory cytokines, including tumor necrosis factor-alpha and interleukin-6, can downregulate OCTN2 expression, resulting in increased urinary carnitine loss without overt renal dysfunction.20-23 Chronic low-grade bacteremia may therefore induce a sustained negative carnitine balance sufficient to impair fatty-acid oxidation, even in the absence of systemic inflammatory response syndrome.
An additional, non-mutually exclusive mechanism relates to microbial metabolic adaptability. Achromobacter xylosoxidans exhibits broad substrate utilization capabilities and has been shown in vitro to metabolize quaternary amines under nutrient-limited conditions.24-26 Although direct bacterial consumption of host carnitine has not been demonstrated in vivo, the organism’s metabolic plasticity suggests competitive depletion of host-derived metabolites during prolonged bloodstream residence. Such an interaction may represent an underrecognized form of host–pathogen metabolic competition with clinically relevant consequences.
Importantly, the biochemical pattern in this case differed from sepsis-associated mitochondrial dysfunction, which is typically characterized by elevated lactate, multiorgan involvement, and poor correlation with fasting states.27,28 The selective impairment of ketogenesis, preserved oxidative phosphorylation markers, and rapid reversibility with targeted therapy are consistent with a mechanism localized to fatty-acid transport rather than generalized mitochondrial failure. This distinction is clinically relevant, as it shifts diagnostic focus away from structural or ischemic pathology and toward dynamic metabolic assessment.
From a clinical perspective, this case challenges the prevailing reliance on imaging to evaluate unexplained myopathy or hypoglycemia. In scenarios where biochemical signatures indicate functional metabolic impairment and microbiological evidence is compelling, imaging may offer limited incremental value. Instead, serial metabolic profiling, urinary carnitine assessment, and microbiological clearance can serve as both diagnostic confirmation and therapeutic endpoints. Incorporating chronic infection into the differential diagnosis of acquired fatty-acid oxidation defects may reduce the need for unnecessary invasive investigations and expedite appropriate treatment.
This report has several limitations inherent to a single-case observational design. Molecular confirmation using polymerase chain reaction or genomic sequencing was not performed, which could have provided additional precision in organism identification and strain characterization. While repeated cultures demonstrated consistent phenotypic identification and susceptibility profiles, molecular methods may have strengthened microbiological certainty. In addition, mechanistic pathways linking chronic bacteremia to altered carnitine homeostasis were inferred from biochemical patterns and existing experimental literature rather than directly measured. Biomarkers of inflammatory signaling and renal tubular transporter expression were not assessed, limiting direct validation of the proposed pathophysiological mechanisms. Finally, although the temporal association between infection clearance and metabolic recovery supports causality, contributory effects of L-carnitine supplementation cannot be entirely excluded.
Conclusion
Chronic bacteremia may act as a modifier of host metabolic function rather than solely a source of persistent infection. The observed disruption of fatty-acid transport demonstrates how prolonged host–pathogen interaction may be associated with reversible metabolic vulnerability without structural tissue injury or critical illness. Integrating metabolic assessment into the evaluation of chronic bloodstream infections may inform diagnostic evaluation and management that are not apparent through conventional organ-focused approaches.
Footnotes
Acknowledgements
The authors extend their gratitude to Medicos In Research, Nautanwa, UP, 273164, India, an initiative by Dr. Amogh Verma, for their unwavering guidance and support throughout the development of this manuscript. Their invaluable contributions provided a platform for us to learn research methodologies, collaborate effectively, expand our professional network, and gain additional insights that significantly enriched this work. We deeply appreciate their efforts in fostering an environment of academic growth and scientific inquiry. Dr. Amogh Verma also serves as an Associate Editor for Clinical Medicine Insights: Case Reports. He was not involved in the editorial handling, peer review, decision-making process, or publication outcome of this manuscript. All editorial decisions were made independently in accordance with the journal’s standard editorial policies. The authors declare that this role did not influence the conduct, interpretation, or reporting of the study.
Ethical Considerations
Ethical approval was not required for this study as per the policies of our institution. The Institutional Review Board waived the need for approval in accordance with the institutional guidelines for case-based studies.
Consent to Participate
Written informed consent was obtained from the patient to participate in this study.
Consent for Publication
Written informed consent was obtained from the patient for publication of this study (including images or case details).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting of Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Generative AI Use Statement
Paperpal and ChatGPT-5.5 were used only for language and stylistic refinement. These tools were not involved in study design, data analysis, interpretation, or content development. All intellectual contributions and scientific interpretations are the sole work of the authors, who take full responsibility for the accuracy, originality, and integrity of the manuscript.