
Abstract
Recurrent inguinoscrotal hernias with visceral involvement present significant technical challenges, particularly when dense adhesions and large hernia sacs limit safe laparoscopic dissection. We report the case of a 55-year-old man with a large recurrent right inguinoscrotal hernia containing predominantly small bowel loops following previous open bilateral inguinal hernia repair. Preoperative computed tomography demonstrated bowel herniation with features suggestive of early incarceration. Surgery was initiated laparoscopically, allowing safe reduction of the herniated bowel and assessment of bowel viability. Due to dense adhesions and difficulty dissecting the large hernia sac laparoscopically, a limited open inguinal approach was performed for controlled sac dissection, followed by laparoscopic posterior mesh placement. This laparoscopic–open–laparoscopic hybrid approach provided a safe and effective solution, combining the benefits of minimally invasive assessment with secure open sac management, and should be considered in complex recurrent inguinoscrotal hernias when laparoscopic sac dissection is unsafe.
Keywords
Introduction
Inguinal hernia repair is among the most commonly performed general surgical procedures; however, recurrent inguinal hernias remain a significant technical challenge, particularly when associated with large scrotal extension and prior surgical intervention. Reported recurrence rates range from 1% to 15%, depending on operative technique, patient factors, and follow-up duration.1,2 Recurrent inguinoscrotal hernias constitute a distinct subgroup characterized by distorted anatomy, dense adhesions, and an increased risk of visceral injury during reoperation.
International guidelines from the HerniaSurge Group and the European Hernia Society recommend a posterior laparo-endoscopic approach for recurrence after anterior repair and an anterior approach following failed posterior repair.1-3 Although laparoscopic techniques such as transabdominal preperitoneal (TAPP) and totally extraperitoneal (TEP) repair provide superior visualization and reduced postoperative pain, their role in large scrotal or incarcerated hernias remains controversial.4,5 More recently, the enhanced-view totally extraperitoneal approach has been introduced, offering improved working space and visualization in complex groin hernias; however, its applicability in large inguinoscrotal or incarcerated hernias remains limited and technically demanding. Long-standing scrotal hernias are frequently associated with bulky sacs, visceral involvement, and chronic adhesions, rendering laparoscopic sac dissection technically challenging and potentially unsafe. 6
In such complex cases, hybrid surgical strategies combining laparoscopic exploration with a limited open anterior approach have been advocated. This approach allows laparoscopic assessment, bowel reduction, and posterior mesh placement while enabling safe open dissection of large or adherent hernia sacs.6-9 Hybrid techniques have been reported in recurrent, re-recurrent, incarcerated, and large scrotal hernias, demonstrating acceptable outcomes with low recurrence rates and reduced risk of visceral injury compared with forced continuation of a single approach.6-10 While hybrid approaches have been previously described, their role as a structured, intraoperative decision-making strategy in complex recurrent inguinoscrotal hernias remains underemphasized. In particular, clear indications for transitioning from a purely laparoscopic to a hybrid approach are not well defined in current literature. This report highlights a safety-driven, stepwise approach to managing a large recurrent inguinoscrotal hernia with visceral involvement, emphasizing intraoperative judgment.
Case Presentation
A 55 year old male patient presented with a progressively enlarging right inguinoscrotal swelling associated with intermittent discomfort. He had a history of previous bilateral inguinal hernia repair, performed via an open anterior approach with no mesh placement, resulting in altered local anatomy. There was no history of prior bowel resection. On physical examination, a large, irreducible right inguinoscrotal hernia was noted, extending well into the scrotum. The overlying skin was intact, and there were no signs of peritonitis.
A contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis demonstrated a large right inguinoscrotal hernia extending through the inguinal canal into the scrotum, containing herniated bowel loops, predominantly small bowel, along with mesenteric fat. Imaging showed luminal narrowing at the hernia neck with crowding of mesenteric vessels, mild bowel wall thickening, and reduced mural enhancement, raising concern for early incarceration. No free intraperitoneal air, bowel perforation, or intra-abdominal abscess was identified (Figure 1). Given the recurrent nature of the hernia, the large scrotal extension, colonic involvement, and radiologic concern for incarceration, surgical repair was indicated. Contrast-enhanced computed tomography of the abdomen and pelvis CT images showing a large right inguinoscrotal hernia extending into the scrotum and containing herniated colon and mesenteric fat. Luminal narrowing at the hernia neck with crowding of mesenteric vessels and mild bowel wall thickening suggest early incarceration. No free intraperitoneal air is seen
The procedure was initiated with diagnostic laparoscopy using a TAPP approach. Intraoperative findings confirmed a large recurrent right inguinoscrotal hernia with herniation of the small bowel through the internal ring. Careful dissection of the peritoneum around the hernia neck was performed, and gentle traction allowed successful reduction of the herniated bowel and mesentery into the abdominal cavity (Figure 2). Bowel viability was confirmed based on color, peristalsis, and pulsation of mesenteric vessels. However, further laparoscopic dissection of the hernia sac proved technically challenging due to dense adhesions and the large size of the sac, with concerns for prolonged operative time and potential visceral or cord injury. Intraoperative laparoscopic view laparoscopic image demonstrating colonic herniation into the right inguinoscrotal hernia sac through the internal inguinal ring prior to reduction, with surrounding adhesions contributing to difficult laparoscopic sac dissection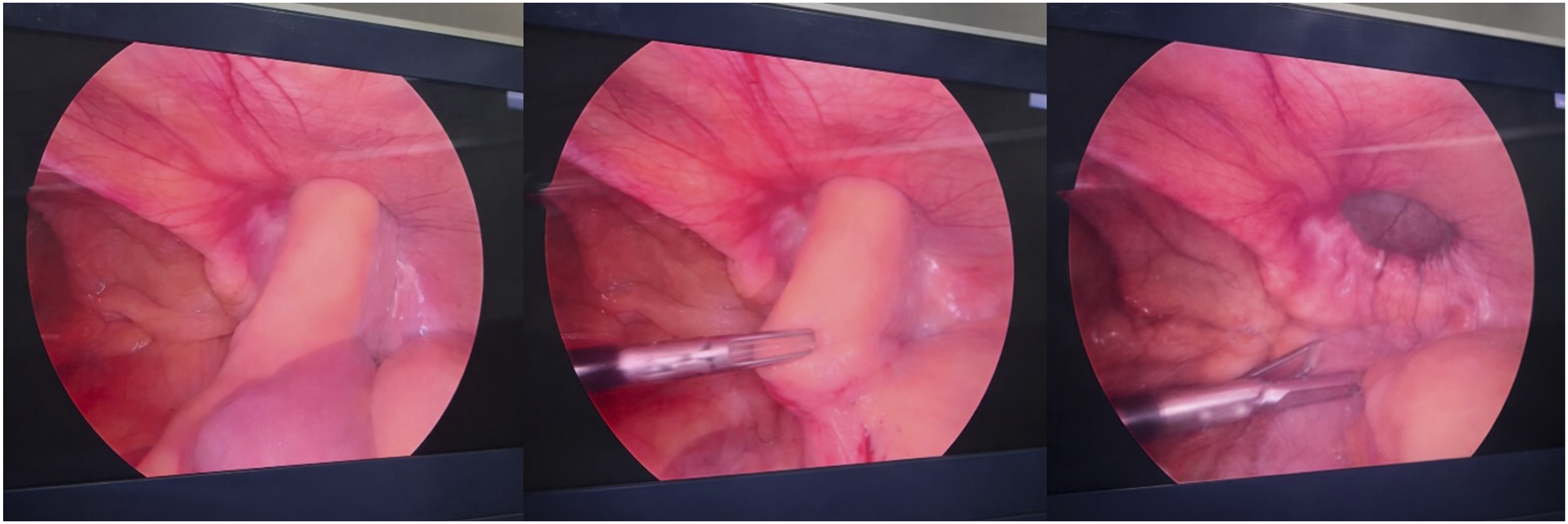
A right inguinal incision was therefore performed. Dissection was carried down through the previous scar to the external oblique aponeurosis. The spermatic cord structures were carefully identified and protected. Due to pressure from abdominal insufflation, the hernia sac easily protruded like a balloon. The sac was safely isolated from surrounding scrotal tissues, opened to confirm complete reduction, ligated, and transected at the level of the internal ring. This step was completed efficiently, achieving secure control of the sac with excellent hemostasis. The inguinal canal was then closed in layers. Although laparoscopic reduction of the hernia contents had been achieved, the sac was intentionally opened via the inguinal approach to ensure complete reduction, exclude any missed sliding component or residual adhesions, and allow safe ligation of the large scrotal sac. This step also minimized the risk of postoperative seroma formation and facilitated definitive management of the redundant sac.
Primary laparoscopic closure or reduction of the sac without opening was not pursued due to the large size of the scrotal component and dense adhesions, which increased the risk of incomplete management and postoperative complications such as seroma or recurrence.
Attention was subsequently returned to the abdominal cavity. Laparoscopic re-inspection confirmed complete reduction of contents and clear delineation of the myopectineal orifice. A large lightweight polypropylene mesh (e.g., 15 × 10 cm) was placed in the preperitoneal space, chosen for its durability, wide coverage of the myopectineal orifice, and compatibility with laparoscopic placement.
The patient tolerated the procedure well with no intraoperative complications. Postoperatively, he experienced minimal pain managed with multimodal analgesia and was mobilized on the day of surgery. Oral intake was resumed on postoperative day one. He was discharged in good condition on postoperative day two. At follow-up, surgical wounds were healing appropriately, scrotal swelling was minimal, bowel function was normal, and no recurrence or chronic groin pain was noted.
Discussion
Recurrent inguinal hernia repair remains technically demanding due to altered anatomy, fibrosis, and prior mesh placement, challenges that are further amplified in large inguinoscrotal hernias with bulky sacs, visceral involvement, and dense adhesions. Recurrence rates following inguinal hernia repair range from 1% to 15%, depending on operative technique, patient factors, and follow-up duration.1,2
International guidelines from the HerniaSurge Group and the European Hernia Society recommend a posterior laparo-endoscopic approach (TAPP or TEP) for recurrence after anterior repair and an anterior approach following failed posterior repair.1-3 These recommendations are supported by comparative and registry-based studies favoring repair through the anatomical plane opposite the previous operation.3,11 However, the guidelines acknowledge that complex hernias, including large scrotal hernias, incarceration, or extensive adhesions, require individualized intraoperative decision-making.1,3
Laparoscopic approaches provide important advantages in recurrent hernia surgery, including panoramic visualization of the myopectineal orifice, identification of prior mesh position, and assessment of bowel viability in incarcerated cases. 4 In the present case, laparoscopy enabled safe reduction of herniated colon and confirmation of bowel viability. Nevertheless, laparoscopic sac dissection in large or long-standing inguinoscrotal hernias has been associated with increased risks of bowel injury, testicular vessel compromise, and prolonged operative time.5,12
To mitigate these risks, hybrid surgical strategies combining laparoscopy with a limited open anterior approach have been increasingly advocated. Ferzli et al demonstrated favorable outcomes using a combined laparoscopic and open extraperitoneal approach in large scrotal hernias when laparoscopic reduction proved unsafe. 6 Similarly, Bansal et al emphasized early adoption of laparoscopic-assisted hybrid techniques when hernia contents cannot be safely reduced or visualization is compromised, particularly in massive scrotal hernias. 7 In our case, early transition to an open inguinal incision allowed rapid and controlled sac dissection, avoiding prolonged laparoscopic manipulation. Opening and ligation of the hernia sac via an anterior approach remains a valuable adjunct in large inguinoscrotal hernias, particularly when redundant scrotal sacs are present. This step helps reduce seroma formation and ensures complete management of the hernia sac, which may not be reliably achieved laparoscopically in such cases.
Hybrid approaches have also been described in recurrent and re-recurrent inguinal hernias, where laparoscopy serves as a diagnostic and guidance tool rather than the sole repair modality. 8 In emergency settings, Ooe et al reported successful hybrid repair of obstructed recurrent hernias, highlighting the limitations of laparoscopy in the presence of bowel dilatation and adhesions. 9
Additional evidence supports the view that large scrotal hernias represent a relative contraindication to purely laparoscopic repair, with higher technical difficulty and complication rates reported.5,12 Diagnostic laparoscopy has therefore been advocated as a decision-making tool in complex and re-recurrent hernias, enabling tailored selection of open, laparoscopic, or hybrid strategies. 10
Overall, the available literature supports a tailored, safety-driven approach for complex recurrent inguinoscrotal hernias. In the present case, a laparoscopic–open–laparoscopic hybrid strategy facilitated safe bowel reduction, efficient sac dissection, and definitive posterior mesh reinforcement, consistent with published evidence and contemporary guideline principles. The added value of this report lies not in the novelty of the hybrid technique itself, but in illustrating its role as a pragmatic, safety-oriented strategy in complex recurrent inguinoscrotal hernias. Specifically, this case demonstrates the importance of early intraoperative decision-making to avoid prolonged and potentially hazardous laparoscopic dissection in the presence of dense adhesions and large scrotal sacs. 13
Conclusion
Large recurrent inguinoscrotal hernias with visceral involvement represent a challenging subset of inguinal hernia disease, in which rigid adherence to a single operative approach may compromise safety. This case demonstrates that a laparoscopic–open–laparoscopic hybrid strategy allows safe reduction of herniated bowel, efficient dissection of a large and adherent hernia sac under direct vision, and definitive posterior mesh reinforcement. By integrating the complementary advantages of laparoscopy and open surgery, hybrid repair offers a pragmatic, tailored solution for complex recurrent inguinal hernias and should be considered when laparoscopic sac dissection is technically difficult or potentially hazardous.
Footnotes
Acknowledgements
The authors would like to acknowledge the surgical team and operating room staff involved in the management of this case for their contribution to patient care. We also thank the patient for providing consent for publication of this case report.
Ethical Considerations
This case report was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was not required for this study as it describes a single clinical case without experimental intervention, in line with institutional policies.
Consent to Participate
Informed consent to participate was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Identifying information has been anonymized to ensure patient confidentiality. A copy of the written consent is held by the authors and is available for review by the journal upon request.
Author Contributions
HF contributed to the conception and design of the study, acquisition and interpretation of clinical data, and drafting of the manuscript. GK was involved in the surgical management of the patient, critically revised the manuscript for important intellectual content, and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to this case report are included within the article. No additional datasets were generated or analyzed during the current study.