
Abstract
Background
Gastric adenocarcinoma remains a major cause of cancer-related morbidity and mortality worldwide. Early detection is crucial for improving prognosis; however, early lesions may be overlooked during esophagogastroduodenoscopy (EGD), particularly in anatomically challenging areas such as the incisura angularis. This region is considered a high-risk site for gastric neoplasia and may act as a blind spot during routine endoscopic evaluation.
Case summary
A 38-year-old female with a history of chronic gastroesophageal reflux disease presented with worsening reflux symptoms, postprandial epigastric pain, and recurrent vomiting. Nine months prior, the patient had undergone an EGD for similar symptoms, which showed no significant abnormalities. Despite treatment with proton pump inhibitors, her symptoms progressively worsened and were accompanied by early satiety and an 8-kg unintentional weight loss. A repeat EGD was performed and revealed suspicious ulcerative lesions at the level of the incisura angularis. Multiple biopsies were obtained, and histopathological examination confirmed gastric adenocarcinoma. The patient was subsequently referred for multidisciplinary management and oncological evaluation.
Conclusion
This case highlights the potential for gastric adenocarcinoma to be missed during initial endoscopic examination, particularly at the incisura angularis. Careful mucosal inspection and appropriate retroflexion during EGD are essential for improving lesion detection in this high-risk anatomical region.
Introduction
Gastric adenocarcinoma remains a major life-threatening malignancy worldwide and is a significant contributor to cancer-related mortality. Early detection plays a critical role in improving survival outcomes. 1 However, many patients are diagnosed at advanced stages due to the insidious onset of symptoms and delays in detection.
Patients commonly present with nonspecific gastrointestinal complaints such as heartburn, postprandial epigastric pain, nausea, or dyspepsia.2,3 These vague symptoms may lead healthcare providers to initially attribute them to benign gastrointestinal disorders, thereby delaying diagnosis.
Esophagogastroduodenoscopy (EGD) is considered the gold standard for the diagnosis of gastric cancer.4,5 Nevertheless, early gastric lesions may be missed during endoscopic examination, particularly in anatomically challenging areas such as the incisura angularis. Studies have reported that a considerable proportion of gastric cancers are overlooked during prior endoscopic examinations.
In this report, we describe a case of gastric adenocarcinoma located at the incisura angularis that was not detected during an initial EGD but was diagnosed nine months later on repeat endoscopy. This case emphasizes the importance of careful endoscopic evaluation of this high-risk anatomical site.
Case Presentation
A 38-year-old female with a history of chronic gastroesophageal reflux disease presented to the clinic with worsening reflux symptoms and postprandial epigastric pain. She also reported daily episodes of vomiting. The patient does not have a family history of gastric or colorectal cancer. She denies any family history of hereditay cancer syndromes. She is a non-smoker and denies any history of autoimmune gastritis or previous Helicobacter pylori exposure.
Nine months prior to presentation, the patient had consulted her primary care physician for similar symptoms. At that time, an esophagogastroduodenoscopy (EGD) was performed, which did not reveal any significant abnormalities. The patient was managed conservatively with proton pump inhibitors and was advised to follow up in the clinic.
Despite medical therapy, her symptoms persisted and progressively worsened. She also developed early satiety and experienced an unintentional weight loss of approximately 8 kg. Due to the persistence and progression of symptoms, she was referred to our institution for further evaluation.
Physical examination revealed mild epigastric tenderness on deep palpation without any palpable abdominal masses. A repeat EGD was performed. During the procedure, suspicious ulcerative lesions were identified at the level of the incisura angularis, raising strong suspicion for malignancy (Figure 1). Endoscopic view of the gastric incisura angularis showing suspicious ulcerative lesions. Esophagogastroduodenoscopy demonstrating irregular ulcerated mucosal lesions located at the level of the incisura angularis, raising suspicion for malignant pathology (black arrow)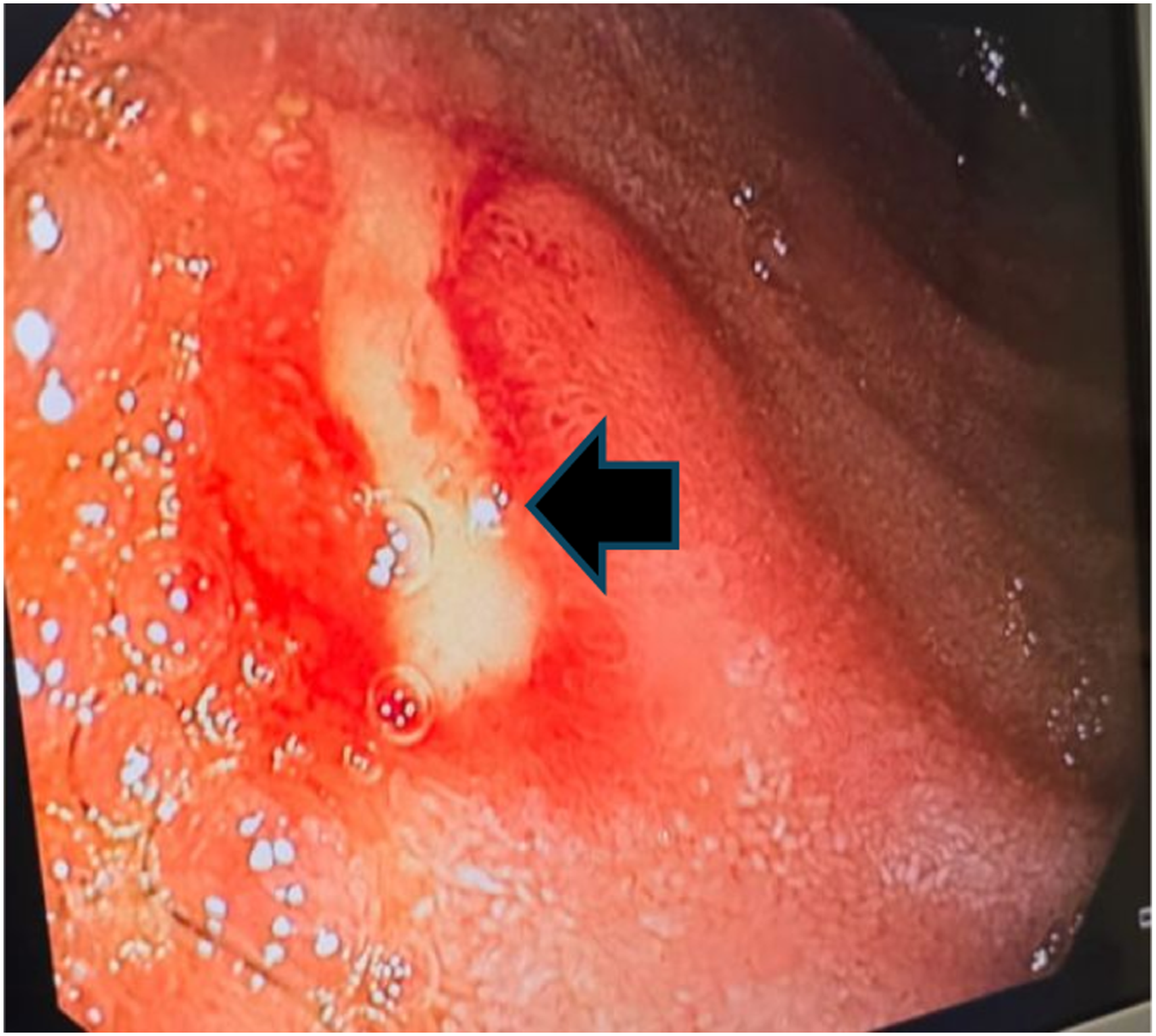
Multiple biopsies were obtained from the lesion (Figure 2). Histopathological examination confirmed the diagnosis of gastric adenocarcinoma of intestinal subtype with moderate differentiation. Immunohistochemical analysis for HER2, mismatch repair (MMR)/microsatellite instability (MSI), and PD-L1 status was performed. Results demonstrated negativity for HER2, MMR and PD-L1 with a low MSI status. Endoscopic biopsy of the lesion at the incisura angularis. Endoscopic image demonstrating biopsy sampling of the suspicious ulcerative lesion at the incisura angularis using standard biopsy forceps during esophagogastroduodenoscopy (black arrow)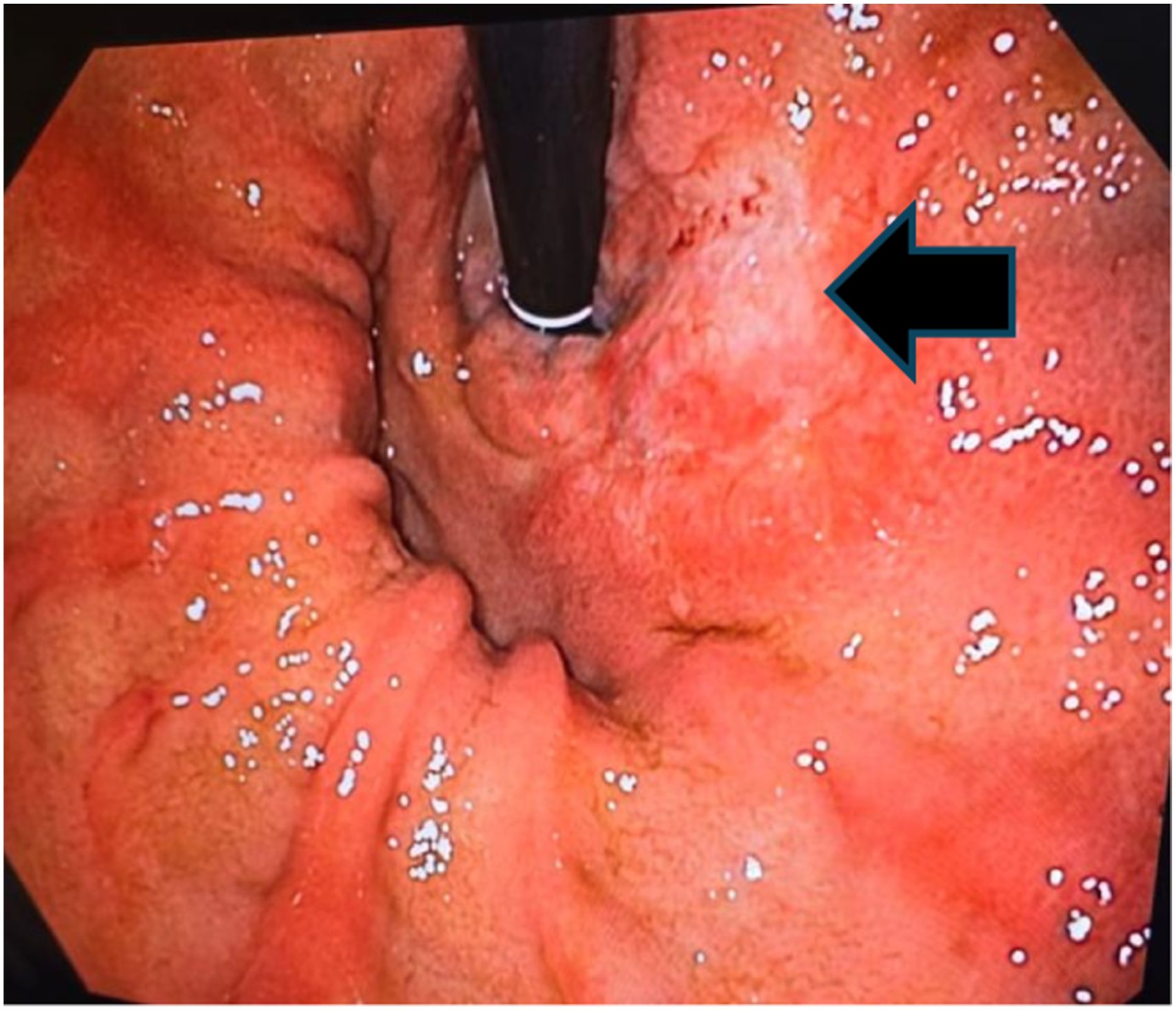
The biopsy specimens obtained during esophagogastroduodenoscopy were also evaluated for Helicobacter pylori infection using histopathological examination, which was negative. Initial laboratory investigations, including complete blood count and liver function tests, were within normal limits except for mild anemia with a hemoglobin level of 11.2 g/dL. Tumor markers, including CEA and CA 19-9, were obtained as part of the initial oncologic workup and were within normal limits.
Contrast-enhanced computed tomography (CT) of the chest, abdomen, and pelvis demonstrated focal gastric wall thickening at the level of the incisura angularis without evidence of distant metastatic disease. Positron emission tomography-computed tomography (PET-CT) demonstrated hypermetabolic thickening at the level of the gastric incisura angularis consistent with the known primary gastric malignancy, without evidence of distant metastatic disease.
The patient was subsequently referred for multidisciplinary oncologic evaluation for further staging and management. An oncology consultation was obtained for staging workup and consideration of neoadjuvant chemotherapy as part of the management plan.
The patient was referred to the oncology service for multidisciplinary management. She underwent full staging workup confirming absence of distant metastases and was subsequently evaluated for neoadjuvant chemotherapy followed by surgical management. At the time of manuscript preparation, she remains under active oncologic follow-up.
Discussion
Gastric adenocarcinoma remains one of the leading causes of cancer-related mortality worldwide. Its pathogenesis involves a complex interplay of environmental, infectious, and genetic factors. Chronic inflammation of the gastric mucosa plays a pivotal role in carcinogenesis and may lead to a sequence of histopathological changes known as the Correa cascade. 5
This cascade typically begins with chronic gastritis, most commonly associated with Helicobacter pylori infection. Over time, persistent inflammation may progress to atrophic gastritis, intestinal metaplasia, dysplasia, and eventually gastric adenocarcinoma. 2
Premalignant changes frequently occur at the level of the incisura angularis, which represents the transitional zone between the gastric antrum and the body. This anatomical region is therefore considered a high-risk site for the development of gastric neoplasia.3,4
Although endoscopy is highly effective for detecting gastric cancer, early lesions can be missed during routine examination. Previous studies suggest that approximately 10% of gastric cancers are missed during initial endoscopy. 5 Missed lesions may result from several factors, including perceptual errors, inadequate mucosal exposure, and sampling errors. 5
The incisura angularis is particularly prone to diagnostic oversight. Due to its sharp angulation and dynamic peristaltic movements, it may act as a blind spot during forward-viewing endoscopy. 6 Additionally, early neoplastic lesions may appear isochromatic with surrounding mucosa, making them difficult to recognize visually. 7
In the present case, the patient underwent an EGD nine months prior to diagnosis, which did not reveal any abnormalities. However, repeat endoscopy performed for worsening symptoms revealed suspicious ulcerative lesions at the incisura angularis.
During the second examination, careful retroflexion of the endoscope was performed to allow optimal visualization of this region. Retroflexion provides a better view of the gastric mucosa and can significantly improve the detection of subtle mucosal abnormalities. In our patient, this maneuver allowed precise visualization of the incisura angularis and facilitated the identification of the malignant lesion.
Missed gastric cancer, also referred to as interval gastric cancer, remains an important limitation of diagnostic esophagogastroduodenoscopy (EGD). Meta-analyses have demonstrated that approximately 6–10% of upper gastrointestinal cancers are missed within 1 year prior to diagnosis, while up to 11% may be missed within 3 years of a prior endoscopic examination. Several predictors of missed gastric cancer have been identified, including younger age, female sex, diffuse histologic subtype, inadequate biopsy sampling, gastric ulceration, and technically suboptimal endoscopic examinations. 5 The growing recognition of interval gastric cancers has led to increased emphasis on quality indicators for diagnostic EGD. Current quality measures include adequate mucosal visualization, sufficient insufflation and mucosal cleansing, systematic photo-documentation, careful inspection time, and appropriate biopsy protocols. European and British guidelines recommend standardized photo-documentation of key anatomical landmarks, including retroflexed views of the cardia, fundus, and incisura angularis, to reduce blind spots during examination. Careful inspection time during EGD has also emerged as an important determinant of neoplasia detection. 6 Studies suggest that prolonged and systematic mucosal examination improves the detection of early gastric neoplasia and premalignant lesions. Similarly, adequate photo-documentation may serve both as a quality-control measure and as confirmation that high-risk anatomical areas were sufficiently examined. Advanced imaging techniques may further improve lesion detection. Image-enhanced endoscopy modalities such as narrow-band imaging (NBI), chromoendoscopy, and magnification endoscopy can increase visualization of subtle mucosal and vascular abnormalities that may not be apparent under conventional white-light endoscopy. These techniques are particularly valuable for identifying early gastric cancer and areas of intestinal metaplasia or dysplasia. 7
The incisura angularis represents a particularly important anatomical blind spot during forward-viewing endoscopy because of its sharp angulation and dynamic peristalsis. Retroflexion allows improved visualization of the lesser curvature and angularis region and may therefore increase detection of subtle lesions that could otherwise remain undetected. In our patient, careful retroflexion during repeat EGD enabled direct visualization of the malignant ulcerative lesion at the incisura angularis. 5
Our case is also notable because the patient was relatively young. Although gastric adenocarcinoma is more common in older individuals, interval gastric cancers have also been reported in younger patients, particularly females and patients with diffuse-type histology. Younger age has paradoxically been associated with diagnostic delay and missed lesions, partly because symptoms may initially be attributed to benign gastrointestinal disorders.
This case highlights the importance of systematic inspection of the gastric mucosa during endoscopy, with particular attention to high-risk anatomical sites such as the incisura angularis. Adequate mucosal exposure, careful retroflexion, and a high index of suspicion are essential to minimize the risk of missed lesions.
Conclusion
Gastric adenocarcinoma remains a common and potentially fatal gastrointestinal malignancy. Early detection is essential for improving patient outcomes but remains challenging due to subtle early-stage lesions and anatomical blind spots during endoscopy.
This case describes a gastric adenocarcinoma located at the incisura angularis that was missed during an initial EGD and subsequently diagnosed nine months later on repeat examination. The report emphasizes the importance of meticulous endoscopic technique, including adequate retroflexion and thorough inspection of high-risk areas such as the incisura angularis.
Improving awareness of these potential blind spots may help reduce the incidence of missed gastric cancers and facilitate earlier diagnosis.
Footnotes
Ethical Considerations
Case reports are exempted from ethical approval at our institution.
Consent to Participate
A signed written informed consent was obtained prior to manuscript writing and submission.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.