
Abstract
Introduction
Clozapine is the most effective antipsychotic for treatment-resistant schizophrenia but is associated with a dose-dependent reduction in seizure threshold. While seizures are typically linked to high doses or rapid titration, events at therapeutic doses remain clinically significant and poorly characterized, particularly in resource-limited settings.
Case presentation
We report a 35-year-old Ethiopian man with treatment-resistant schizophrenia stabilized on clozapine 300 mg/day for 8 months who presented with a first generalized tonic–clonic seizure. There was no prior seizure history. Laboratory evaluation and neuroimaging were unremarkable. Electroencephalography (EEG) demonstrated generalized spike–wave discharges with photoparoxysmal response, suggesting underlying epileptiform susceptibility. Clozapine serum levels were unavailable. After exclusion of alternative causes, the event was considered likely clozapine-associated. Clozapine dose was reduced to 200 mg/day and sodium valproate initiated. The patient remained seizure-free at 6-month follow-up with preserved psychiatric stability.
Conclusion
Clozapine may precipitate seizures at therapeutic doses in patients with latent epileptiform susceptibility. When therapeutic drug monitoring is unavailable, careful clinical assessment, EEG evaluation, and exclusion of alternative causes are essential. Dose reduction with anticonvulsant therapy may permit safe continuation of clozapine.
Introduction
Clozapine remains the gold standard for treatment-resistant schizophrenia because of its superior efficacy in symptom reduction and suicide prevention compared with other antipsychotics.1,2 However, its use is limited by adverse effects, including agranulocytosis, myocarditis, metabolic disturbances, and reduced seizure threshold. 3 Clozapine-associated seizures occur in approximately 1% to 5% of patients at standard doses, with higher risk at doses exceeding 600 mg/day.4,5 Recognized risk factors include rapid titration, high plasma concentrations, concomitant medications that lower seizure threshold, and pre-existing neurological vulnerability. 6
Seizures occurring at therapeutic doses are less commonly reported but remain clinically important because dose alone may not reliably reflect individual exposure or risk. In resource-limited settings where clozapine serum level monitoring is often unavailable, clinicians must rely on clinical assessment, electroencephalography, and exclusion of alternative causes. We present a case of a first generalized tonic–clonic seizure in a patient receiving a stable therapeutic dose of clozapine, highlighting diagnostic considerations, the role of EEG, and management strategies.
Case Presentation
A 35-year-old Ethiopian man with a 12-year history of treatment-resistant paranoid schizophrenia presented to the emergency department after a witnessed generalized tonic–clonic seizure. His psychiatric illness had been refractory to haloperidol, risperidone, and olanzapine. Clozapine had been initiated 8 months prior and titrated gradually over 8 weeks to 300 mg/day (150 mg twice daily), resulting in significant clinical improvement (Clinical Global Impression-Severity score reduced from 6 to 3).
He had no prior history of seizures, head trauma, central nervous system infection, or family history of epilepsy. His only concomitant medication was clonazepam 1 mg nightly, taken consistently for 6 months. The seizure occurred at home and was characterized by sudden loss of consciousness, tonic stiffening followed by rhythmic clonic movements lasting approximately 2 minutes, urinary incontinence, and post-ictal confusion for 30 minutes. There were no preceding symptoms such as fever, headache, or trauma.
On arrival, he was alert, oriented, and neurologically intact. Vital signs were stable. Laboratory investigations, including complete blood count, serum electrolytes (sodium 138 mmol/L, potassium 4.1 mmol/L, calcium 2.2 mmol/L), glucose (92 mg/dL), and renal and liver function tests, were within normal limits. Electrocardiogram and non-contrast CT brain were unremarkable.
Electroencephalography performed 48 hours later showed a normal background rhythm with intermittent generalized spike–wave discharges lasting 1–2 seconds, enhanced by photic stimulation (photoparoxysmal response) (Figure 1). These findings are characteristic of generalized epileptiform activity and suggest underlying neuronal hyperexcitability rather than purely provoked seizure activity.
7
Electroencephalogram (EEG) demonstrating generalized spike–wave discharges with photoparoxysmal response. The recording shows a background rhythm interrupted by intermittent, bilaterally synchronous spike–wave complexes across multiple channels. During photic stimulation (highlighted by vertical markers), there is a marked increase in generalized epileptiform activity, consistent with a photoparoxysmal response and suggestive of underlying generalized epileptiform susceptibility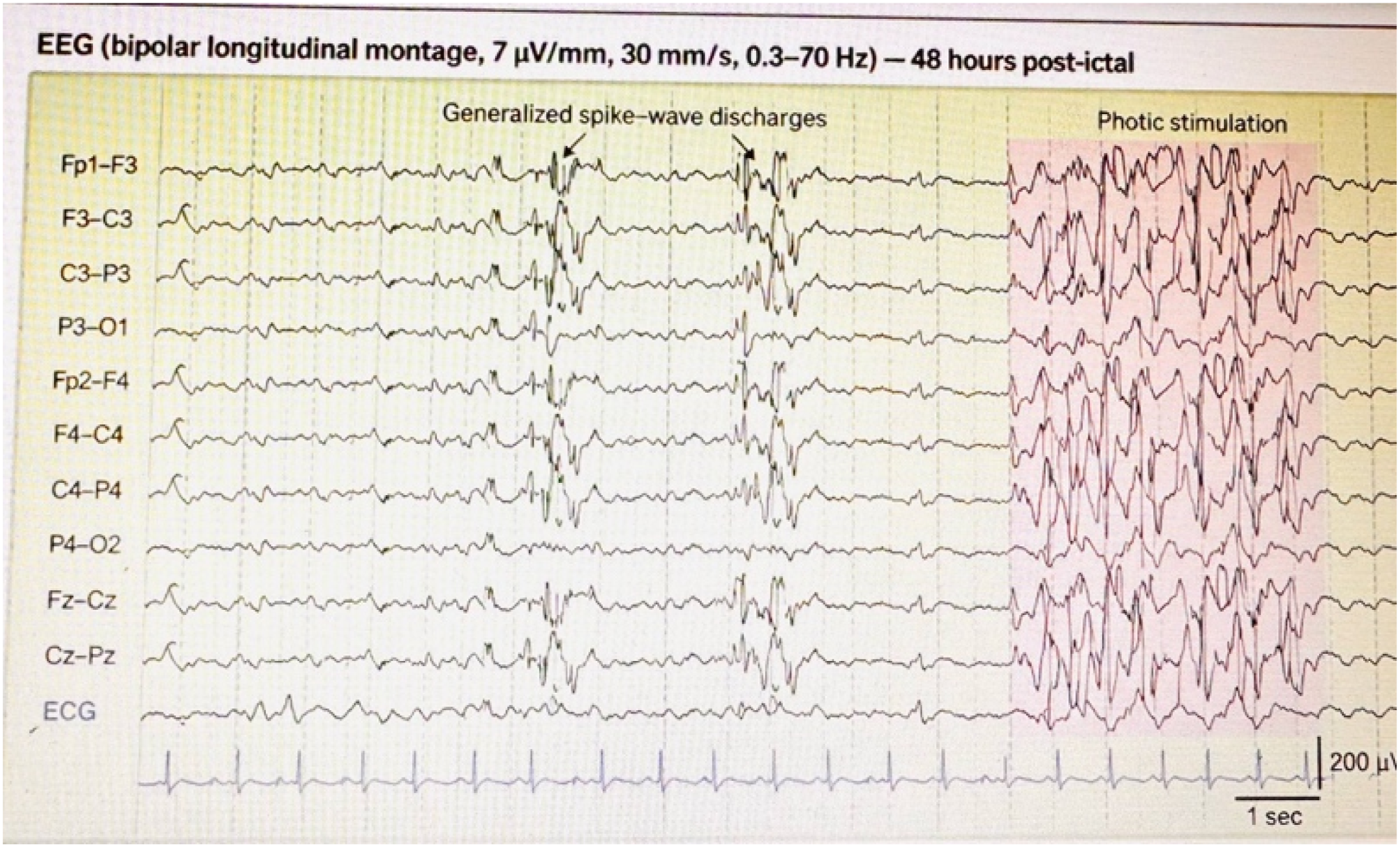
Clozapine serum levels were not available. No alternative precipitants were identified, including metabolic disturbance, infection, or substance withdrawal. The event was therefore considered most likely clozapine-associated, with possible contribution from underlying epileptiform susceptibility. Clozapine dose was reduced to 200 mg/day (100 mg twice daily), and sodium valproate 500 mg twice daily was initiated. Clonazepam was continued unchanged. The patient remained hospitalized for 5 days without recurrence.
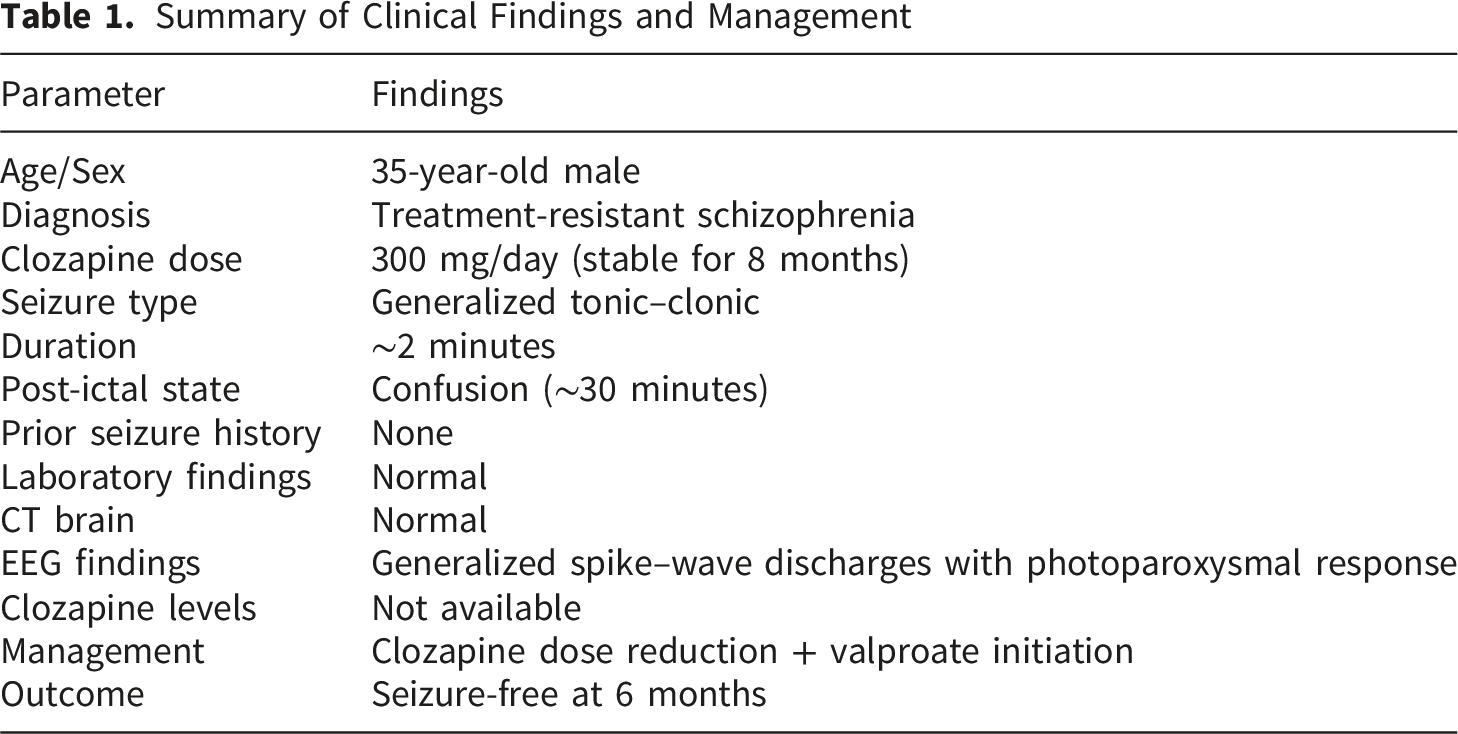
Summary of Clinical Findings and Management
Discussion
This case illustrates a generalized seizure occurring at a therapeutic, stable dose of clozapine, emphasizing that seizure risk is not restricted to high doses or early titration phases. While the temporal association and absence of alternative causes support a drug-related event, the EEG findings introduce an important nuance. The presence of generalized spike–wave discharges with photoparoxysmal response is more consistent with an underlying predisposition to generalized epilepsy rather than a purely drug-induced seizure. 7
Thus, the most accurate interpretation is that clozapine likely lowered the seizure threshold sufficiently to unmask latent epileptiform activity, rather than being the sole cause. This distinction is important, as it reframes the mechanism from direct toxicity to interaction with patient-specific neurophysiological vulnerability.8,9
Although the dose of 300 mg/day falls within the therapeutic range, clozapine pharmacokinetics exhibit significant interindividual variability. Plasma concentrations may vary due to genetic factors, smoking status, and metabolic differences. In the absence of therapeutic drug monitoring, dose alone cannot reliably indicate exposure risk. 8
EEG played a critical role in this case by supporting epileptiform activity, suggesting underlying susceptibility, and providing an objective baseline for follow-up. In resource-limited settings where drug levels are unavailable, EEG may serve as a key diagnostic adjunct.
Management required balancing seizure risk against psychiatric relapse. Clozapine discontinuation carries a high risk of symptom exacerbation and withdrawal phenomena. 10 Dose reduction combined with sodium valproate represents a pragmatic strategy. Valproate is preferred due to minimal pharmacokinetic interaction with clozapine. In contrast, carbamazepine is avoided due to risk of agranulocytosis and enzyme induction.11,12
The favorable outcome in this case supports a conservative approach that prioritizes continuation of clozapine when clinically feasible. This case highlights that seizures can occur at therapeutic clozapine doses, that underlying epileptiform predisposition may modify risk, that EEG is valuable when drug monitoring is unavailable, and that dose reduction with adjunctive anticonvulsant therapy can preserve treatment efficacy.
Limitations
Clozapine and valproate serum levels were not measured, limiting pharmacokinetic interpretation. Additionally, the presence of epileptiform EEG abnormalities raises the possibility that this event represents the first manifestation of underlying epilepsy rather than a purely drug-induced seizure.
Conclusion
Clozapine-associated seizures may occur at therapeutic doses, particularly in patients with latent epileptiform susceptibility. In resource-limited settings, careful clinical evaluation, EEG assessment, and exclusion of alternative causes are essential. Dose reduction combined with anticonvulsant therapy may allow safe continuation of clozapine while maintaining psychiatric stability.
Footnotes
Ethical Considerations
Ethical approval was obtained, and written informed consent was provided by the patient.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.