
Abstract
Background
Hepatic alveolar echinococcosis (HAE), although rare, is a potentially life-threatening parasitic disease when left untreated. Following infection, the disease typically progresses through a prolonged asymptomatic latent phase, resulting in delayed clinical presentation in most patients. The radiological appearance of HAE may closely resemble that of primary hepatic malignancies, thereby creating significant diagnostic challenges.
Case Presentation
We report the case of a 49-year-old previously healthy man who presented with cholestatic liver enzyme abnormalities and imaging findings suggestive of biliary obstruction. Cross-sectional imaging revealed a calcified hilar hepatic mass with biliary dilatation and multiple heterogeneous liver lesions, strongly suggestive of perihilar cholangiocarcinoma. Endoscopic retrograde cholangiopancreatography (ERCP) with brush cytology was initially negative for malignancy. Subsequent magnetic resonance imaging (MRI) demonstrated an infiltrative multiloculated solid-cystic hepatic lesion involving the right hepatic lobe and hilar structures. Definitive diagnosis was ultimately established through liver biopsy and positive serology for alveolar echinococcosis. The patient was treated with albendazole followed by extended right hepatectomy, with favorable postoperative recovery.
Conclusion
HAE may closely mimic perihilar cholangiocarcinoma, exhibiting similar clinical and radiological characteristics. Maintaining a high index of suspicion and obtaining adequate tissue biopsies are essential for establishing an accurate diagnosis and ensuring timely, appropriate management.
Introduction
Alveolar echinococcosis is a zoonotic parasitic disease caused by infection with the larval form of Echinococcus multilocularis. The parasite can invade multiple organs in humans, although the liver is the most frequently affected site. 1 Compared with cystic echinococcosis, caused by Echinococcus granulosus, alveolar echinococcosis is considerably more aggressive and is associated with substantially higher morbidity and mortality rates. In untreated patients, the 10-year mortality rate may reach up to 94%. 2
The progression of HAE is typically slow and insidious. The parasite proliferates through exogenous budding and infiltrative growth, continuously generating new vesicles that progressively invade surrounding tissues. HAE not only infiltrates adjacent hepatic parenchyma, bile ducts, and vascular structures, but may also disseminate extrahepatically to the retroperitoneum, lungs, brain, and other organs through lymphatic and hematogenous spread. Owing to its invasive behavior, HAE has often been referred to as “worm cancer”. 3
Although HAE is classified as a benign parasitic disease, its imaging characteristics may closely resemble those of malignant hepatic tumors, making accurate diagnosis particularly challenging. In this report, we describe a case of hepatic alveolar echinococcosis that radiologically mimicked perihilar cholangiocarcinoma.
Case Presentation
A 49-year-old previously healthy man was admitted to the Department of Gastroenterology and Hepatology at our institution for evaluation of cholestatic liver test abnormalities and suspected biliary obstruction. The patient had no known allergies and denied any family history of gastrointestinal or hepatic malignancy. He was physically active, did not consume alcohol, and was a non-smoker. Further epidemiological questioning revealed that the patient had been living in a rural area of northeastern France, a region known to be endemic for Echinococcus multilocularis. He reported regular outdoor activities in wooded areas and occasional contact with domestic dogs. He denied occupational exposure to livestock, hunting activities, or direct contact with foxes. There was no history of recent international travel. The patient also reported frequent consumption of raw vegetables from local gardens. These epidemiological elements were retrospectively considered compatible with potential exposure to E. multilocularis.
Laboratory investigations demonstrated abnormal liver function tests with a mixed hepatocellular-cholestatic pattern, predominantly cholestatic in nature: aspartate aminotransferase (AST) 73 U/L (normal range 8 to 33 U/L), alanine transaminase (ALT) 108 U/L (normal range 7 to 56 U/L), gamma-glutamyl transferase (GGT) 2044 U/L (normal range 5 to 65 U/L), and alkaline phosphatase (ALP) 2122 U/L (normal range 35 to 147 U/L). Total bilirubin was within normal limits at 11 µmol/L. Additional investigations were performed to evaluate the possibility of hepatobiliary malignancy and alternative causes of biliary obstruction. Serum CA 19-9, carcinoembryonic antigen (CEA), and alpha-fetoprotein (AFP) levels were within normal limits. Serological testing for hepatitis B virus and hepatitis C virus was negative. Serum IgG4 level was normal. No evidence of primary sclerosing cholangitis or other identifiable causes of biliary obstruction was found.
Contrast-enhanced abdominal computed tomography (CT) revealed dilatation of the intrahepatic bile ducts associated with a heterogeneous calcified hilar mass compressing the right portal vein branch. Multiple heterogeneous hypodense hepatic lesions with contrast enhancement were also identified, findings highly suggestive of cholangiocarcinoma (Figure 1A and B). Contrast-enhanced abdominal CT demonstrated a dominant infiltrative heterogeneous lesion involving predominantly segments V, VI, VII, and VIII, with extension toward segment IV and the hepatic hilum. The largest component measured approximately 103 × 63 mm. The lesion contained multiple irregular coarse calcifications and exhibited heterogeneous enhancement with central hypodense areas suggestive of necrosis or microcystic degeneration. A second hilar component measured approximately 63 × 33 mm and was associated with marked dilatation of the intrahepatic bile ducts. The lesion encased the right portal vein branch without clear evidence of complete vascular occlusion. Multiple enlarged lymph nodes were identified within the hepatic hilum and peripancreatic region. Contrast-enhanced abdominal CT: Axial portal venous phase images demonstrate an infiltrative heterogeneous mass involving hepatic segments V–VIII with extension toward segment IV. The lesion contains coarse calcifications and causes intrahepatic biliary duct dilatation (A, B). There is associated encasement of the right portal vein branch. Findings initially suggested perihilar cholangiocarcinoma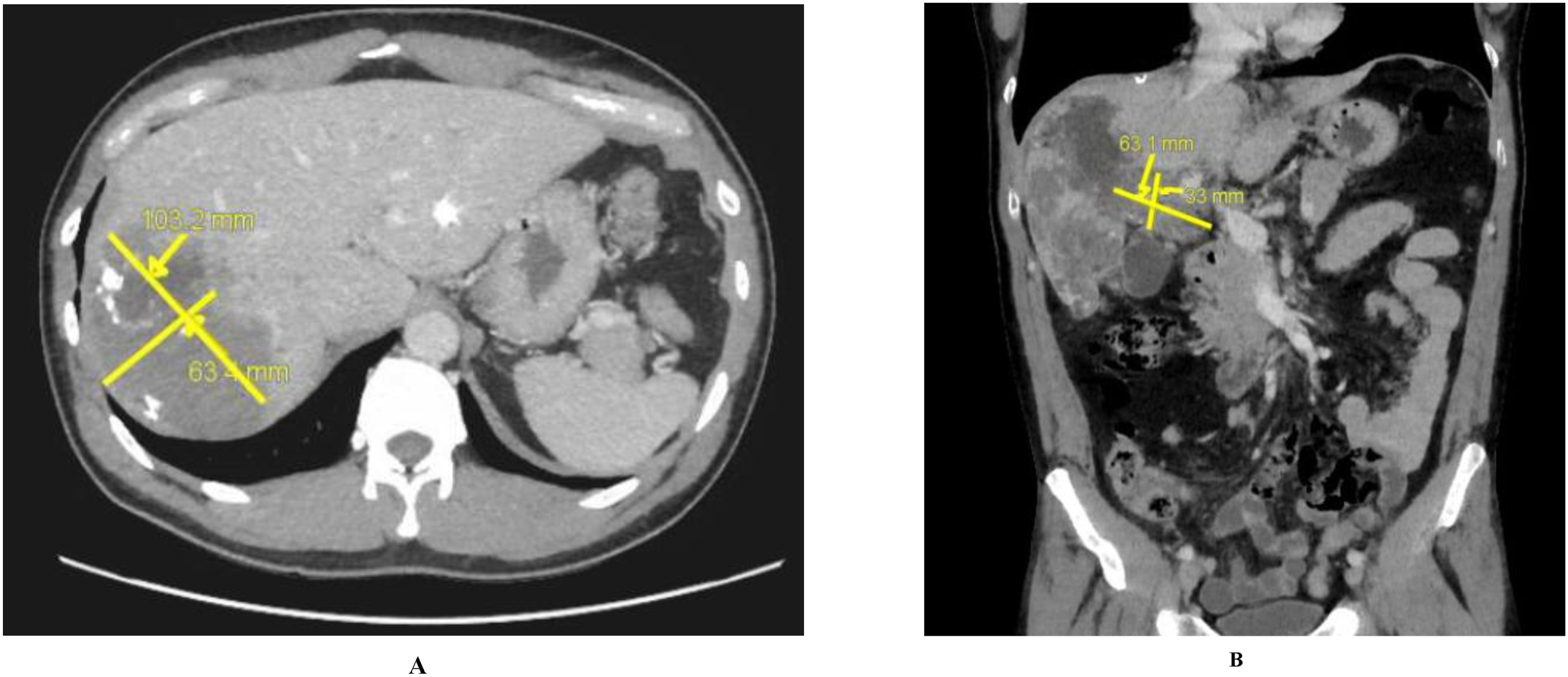
Subsequent liver magnetic resonance imaging (MRI) demonstrated a large infiltrative heterogeneous multiloculated solid-cystic mass involving nearly the entirety of hepatic segments V, VI, VII, and VIII, with extension toward the hepatic dome and segment II. The lesion compressed the right intrahepatic bile ducts and right portal vein branch. No dilatation of the extrahepatic bile ducts was observed. Multiple homogeneous lymphadenopathies were identified in the hepatic hilum, peripancreatic region, right costophrenic angle, and along the right pulmonary ligament. These findings initially raised strong suspicion for perihilar cholangiocarcinoma with intrahepatic metastatic spread.
Endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) were subsequently performed. EUS was unable to adequately visualize the biliary confluence because of marked echogenicity artifacts, although dilated intrahepatic bile ducts were observed. During ERCP, brush cytologies were obtained, and two 15-cm plastic stents were placed respectively in the left intrahepatic duct and the right biliary duct to achieve biliary drainage.
Histopathological examination of the brushing biopsies was negative for malignancy. During hospitalization, the patient developed fever associated with elevated inflammatory markers, including a C-reactive protein (CRP) level of 255 mg/L. Blood cultures remained negative. Empirical antibiotic therapy consisting of ceftriaxone 2 g daily and metronidazole 500 mg three times daily was administered for 7 days.
Given the inconclusive findings, a liver biopsy was ultimately performed (Figure 2A, B and C) and revealed features consistent with hepatic echinococcosis (Figure 3). Further parasitological investigations were subsequently undertaken. Stool parasitology was negative. Serological testing for amebiasis, leishmaniasis, bilharziasis, and toxocariasis was negative; however, serology for alveolar echinococcosis returned positive, thereby confirming the diagnosis of hepatic alveolar echinococcosis. Histopathological examination of the liver core biopsy specimen demonstrated extensive acellular eosinophilic laminated membranes embedded within a fibro-inflammatory and partially necrotic background. On hematoxylin and eosin staining, the membranes appeared as refractile, lamellar structures characteristic of echinococcal infection. Periodic acid-Schiff (PAS) staining strongly highlighted the laminated parasitic membranes. Associated chronic inflammatory infiltrates were present with granulomatous reaction. No atypical epithelial proliferation, dysplasia, or malignant cells were identified. These findings were highly suggestive of hepatic alveolar echinococcosis and were subsequently corroborated by positive serological testing for Echinococcus multilocularis. Ultrasound-guided liver biopsy: Real-time ultrasound images showing localization of a right hepatic lobe lesion (A) and needle trajectory during core biopsy using an 18-gauge system with a coaxial introducer (B, C). The procedure yielded adequate tissue samples for histopathological diagnosis Histopathological examination of the biopsy specimen shows pale, refractile eosinophilic membranous structures that are strongly periodic acid–Schiff (PAS) positive. No tumor cells are identified. (PAS stain, ×200 magnification.)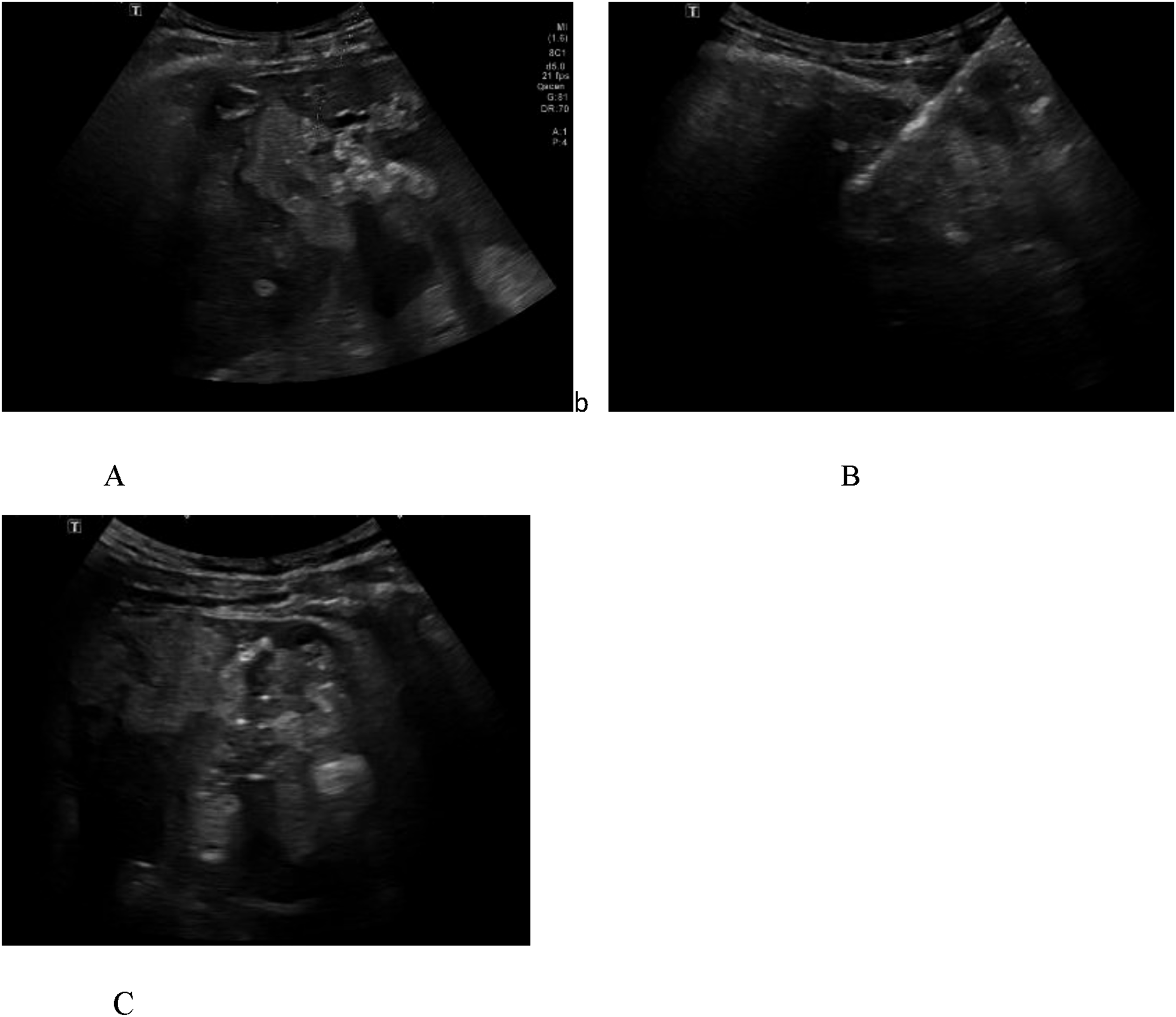

Retrospective application of the WHO-IWGE PNM classification categorized the disease as P3N0M0 (Stage IIIA). The lesion involved the hepatic hilum with biliary and portal vascular involvement extending across both hepatic lobes, without evidence of contiguous extrahepatic organ invasion or distant metastases. This staging was consistent with advanced but potentially resectable disease and supported management with albendazole therapy followed by curative-intent hepatic resection.
Following confirmation of the diagnosis, albendazole was initiated at a dose of 400 mg twice daily in combination with ursodeoxycholic acid 500 mg twice daily. Liver function tests and complete blood counts were monitored regularly during treatment to detect potential hepatotoxicity or hematological adverse effects. The patient tolerated therapy without significant complications.
After multidisciplinary discussion, the patient underwent extended right hepatectomy. Albendazole therapy was continued in the perioperative period and is planned to be maintained postoperatively according to current recommendations. The patient remains under regular clinical, biological, serological, and radiological surveillance, with no evidence of recurrence at the latest follow-up.
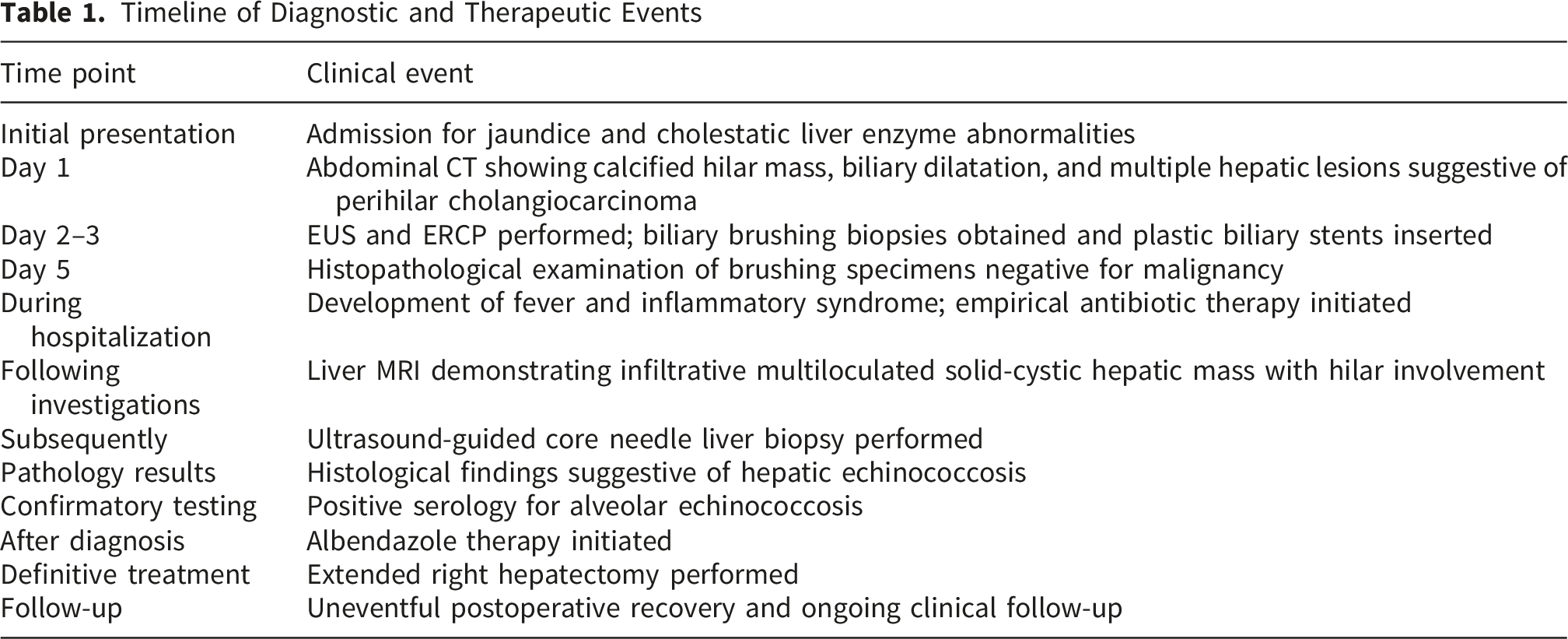
Timeline of Diagnostic and Therapeutic Events
The patient was discussed in a multidisciplinary hepatobiliary tumor board. Although initial imaging strongly suggested perihilar cholangiocarcinoma, subsequent histopathology and positive serology confirmed hepatic alveolar echinococcosis. Surgical resection was indicated due to the presence of a large infiltrative lesion confined to the liver, with no radiological evidence of unresectable extrahepatic spread or distant metastases. The disease was considered resectable based on volumetric and anatomical assessment, allowing for curative-intent extended right hepatectomy following preoperative optimization and antiparasitic therapy.
An extended right hepatectomy was performed. Intraoperatively, the lesion was found to involve segments V, VI, VII, and VIII with extension toward segment IV and the hepatic hilum. Careful dissection of the hepatoduodenal ligament was performed. No vascular reconstruction of the portal vein or hepatic artery was required. Biliary reconstruction was not necessary as adequate margins were achieved at the level of the biliary confluence. No macroscopic peritoneal dissemination was observed.
Gross pathological examination revealed a large infiltrative lesion with heterogeneous solid and necrotic areas containing multiple calcifications. Histological analysis confirmed hepatic alveolar echinococcosis, characterized by laminated acellular PAS-positive membranes surrounded by fibro-inflammatory reaction and necrosis. No malignant cells were identified.
Resection margins were negative for viable parasitic tissue. No evidence of vascular invasion by malignant cells was present. The surrounding liver parenchyma showed inflammation and fibrosis. The postoperative course was uneventful and the patient was discharged home after full recovery.
At the latest follow-up, 1 month after surgery, the patient was clinically well with no abdominal pain, jaundice, or constitutional symptoms. Liver function tests showed normalization of cholestasis.
Serological monitoring for Echinococcus multilocularis demonstrated declining titers. Follow-up contrast-enhanced CT + MRI showed no evidence of residual or recurrent disease.
The patient continues albendazole therapy at a dose of 400 mg twice daily, with good tolerance. Regular monitoring of liver function tests and complete blood counts is performed every 4 weeks. Long-term follow-up has been planned given the risk of late recurrence or residual microscopic disease.
Discussion
Although uncommon, hepatic alveolar echinococcosis is a potentially fatal parasitic disease when left untreated, making prompt and accurate diagnosis critically important. The present case highlights the atypical clinical and radiological presentation of HAE in a 49-year-old patient whose hepatic lesion strongly mimicked perihilar cholangiocarcinoma across multiple imaging modalities.
In the early stages, HAE frequently remains clinically silent. As the disease progresses, the lesion enlarges and progressively infiltrates vascular and biliary structures, resulting in symptoms such as abdominal pain, obstructive jaundice, portal hypertension, liver failure, cachexia, and even metastatic spread to organs such as the lungs and brain.4,5
Currently, the diagnosis of HAE relies primarily on imaging studies, while serological testing serves as an important adjunctive diagnostic tool. Ultrasound, CT, and MRI are the imaging modalities most commonly employed. However, the absence of specific clinical manifestations and the overlapping imaging characteristics with malignant hepatic tumors may lead to frequent misdiagnosis as cholangiocarcinoma, hepatocellular carcinoma, or hepatic hemangioma. 6
Ultrasound is considered the preferred initial screening modality because it is non-invasive, rapid, and cost-effective. CT imaging accurately defines lesion location and morphology, whereas MRI is particularly valuable for assessing the relationship between the lesion and adjacent biliary structures. MRI can also better demonstrate the small cystic vesicles characteristic of the alveolar larval stage, thereby facilitating definitive diagnosis.5,6
Typical imaging findings of HAE include a heterogeneous infiltrative hepatic mass with irregular margins and internal calcifications. On ultrasound, characteristic appearances include the “hailstorm” pattern and the “worm-eaten” appearance. Contrast-enhanced imaging often demonstrates peripheral irregular enhancement with a non-enhancing necrotic center, also referred to as the “black hole sign.” CT commonly reveals irregular low-density lesions with calcifications and central necrosis, whereas MRI generally demonstrates hypointensity on T1-weighted images, hyperintensity on T2-weighted images, and absent or delayed peripheral enhancement. 6
Serological testing plays an important role in diagnosis, epidemiological surveillance, and therapeutic monitoring. Among available assays, recombinant Em18 ELISA (rEm18-ELISA) demonstrates excellent sensitivity and specificity for alveolar echinococcosis. Nevertheless, negative serological results do not exclude the diagnosis, as false-negative findings may occur in histologically confirmed cases. Potential explanations include predominantly necrotic or fibrotic lesions limiting antigen release, early localized disease with insufficient antibody production, or interindividual variability in humoral immune responses. 7
In such cases, tissue diagnosis through targeted biopsy remains essential, ideally sampling the viable peripheral portions of the lesion rather than the necrotic center. Histopathological confirmation relies on identifying characteristic microcystic structures and laminated parasitic membranes within a necrotic background.5,7
Recent advances in molecular diagnostics, particularly metagenomic next-generation sequencing (mNGS), may further improve the identification of parasitic pathogens. Additionally, emerging biomarkers such as serum-derived exosomal circular RNAs have shown promising diagnostic potential in HAE. 7 However, these technologies remain unavailable in many centers, including ours.
Across previously reported cases, hepatic alveolar echinococcosis most commonly mimicked perihilar cholangiocarcinoma or Klatskin tumor due to the presence of hilar infiltrative masses associated with biliary obstruction and cholestatic liver enzyme abnormalities. Tumor markers such as CA19-9 were variably elevated, further contributing to diagnostic confusion. 8
Similar to prior reports, our case demonstrated a hilar infiltrative lesion with biliary dilation and portal vascular involvement, initially favoring a diagnosis of cholangiocarcinoma. However, several features were ultimately more suggestive of alveolar echinococcosis, including extensive intralesional calcifications, multiloculated solid-cystic architecture on MRI, and negative cytological sampling despite significant radiological disease burden. 9
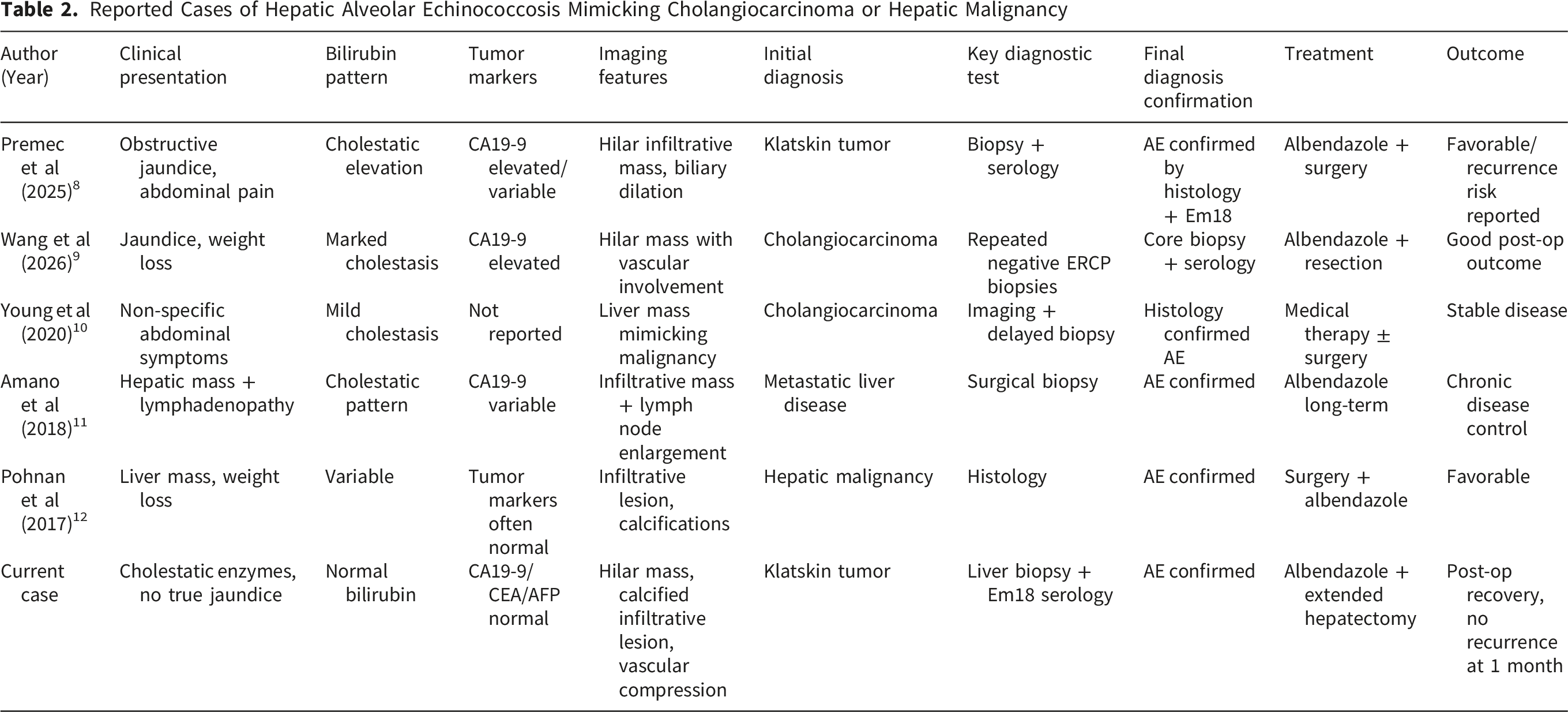
Reported Cases of Hepatic Alveolar Echinococcosis Mimicking Cholangiocarcinoma or Hepatic Malignancy
In the present case, hepatic alveolar echinococcosis closely mimicked perihilar cholangiocarcinoma at initial presentation. Several key features contributed to this diagnostic confusion. First, imaging demonstrated a hilar infiltrative mass associated with marked intrahepatic biliary dilatation, a classic presentation of Klatskin-type cholangiocarcinoma. Second, the lesion was associated with encasement of the right portal vein branch and regional lymphadenopathy, findings frequently interpreted as locally advanced malignant disease. Third, the presence of multiple hepatic lesions raised suspicion for intrahepatic metastases.
Taken together, these findings strongly favored an initial diagnosis of perihilar cholangiocarcinoma.
Despite the initial impression of malignancy, several features were more suggestive of hepatic alveolar echinococcosis. These included the presence of extensive intralesional calcifications, a hallmark of chronic parasitic infection, and the multiloculated solid-cystic architecture observed on MRI, which is atypical for cholangiocarcinoma. In addition, the infiltrative growth pattern across multiple hepatic segments without a clearly defined tumor capsule further supported a parasitic etiology.
Histopathological examination ultimately confirmed the presence of PAS-positive laminated membranes characteristic of Echinococcus multilocularis infection, thereby establishing the diagnosis.
Endoscopic retrograde cholangiopancreatography with biliary brushing cytology was negative for malignancy in this case. This result is consistent with the known limitations of cytological sampling in both cholangiocarcinoma and hepatic alveolar echinococcosis. In alveolar echinococcosis, parasitic tissue is often located in the hepatic parenchyma rather than the biliary epithelium, leading to low diagnostic yield from intraductal sampling. Consequently, negative cytology cannot reliably exclude either malignant or parasitic infiltrative disease.
Definitive diagnosis was achieved through ultrasound-guided core needle biopsy of the hepatic lesion. Histological examination revealed characteristic laminated acellular membranes surrounded by necrotic and fibro-inflammatory tissue, with strong PAS positivity and absence of malignant cells. These findings, combined with positive serology for Echinococcus multilocularis, were diagnostic of hepatic alveolar echinococcosis.
A structured differential diagnosis is essential when evaluating HAE, as its imaging appearance overlaps with several malignant and benign hepatic conditions. Perihilar cholangiocarcinoma typically presents as a predominantly solid infiltrative hilar mass with progressive ductal obstruction and delayed contrast enhancement, whereas HAE more often demonstrates a multiloculated solid–cystic lesion with heterogeneous internal architecture and frequent coarse or punctate calcifications. Unlike cholangiocarcinoma, HAE rarely produces a true desmoplastic mass centered on the bile duct epithelium; instead, it infiltrates along hepatic parenchyma and vascular structures in a tumor-like pattern. 10
Hepatic metastases may also mimic HAE, particularly when cystic degeneration or calcifications are present. However, metastases are usually multiple, well-circumscribed lesions with a known primary tumor history, and they typically lack the characteristic infiltrative “pseudotumoral” growth pattern and parasitic laminated membranes seen in HAE. Hepatocellular carcinoma (HCC), especially the fibrolamellar or scirrhous subtypes, may contain calcifications and appear heterogeneous; however, HCC is usually associated with cirrhosis or chronic hepatitis and demonstrates arterial phase hyperenhancement with portal venous washout, features not typical of HAE. 11
Other calcified hepatic lesions, such as treated hydatid cysts (cystic echinococcosis), abscesses, or hemangiomas with phleboliths, can also enter the differential diagnosis. Cystic echinococcosis more commonly appears as a well-defined cyst with daughter cysts and a pericyst, rather than the infiltrative, tumor-like pattern of HAE. Ultimately, serological testing (particularly Em18-based assays) combined with histopathological identification of PAS-positive laminated membranes remains decisive for definitive diagnosis. 12
This case highlights the importance of obtaining tissue from viable hepatic lesions rather than relying solely on biliary sampling when imaging findings are inconclusive.
Previous reports have documented similar diagnostic challenges in which hepatic alveolar echinococcosis mimicked cholangiocarcinoma or other hepatic malignancies. 11 Across these cases, a consistent pattern emerges: patients frequently present with cholestatic liver enzyme abnormalities and hilar infiltrative lesions on imaging, often leading to an initial diagnosis of cholangiocarcinoma. 12 Tumor markers such as CA19-9 may be normal or variably elevated, further complicating diagnosis.
As in our case, definitive diagnosis is typically achieved only after liver biopsy and/or serological testing, emphasizing the limited sensitivity of initial endoscopic sampling techniques.
This case underscores the importance of considering hepatic alveolar echinococcosis in the differential diagnosis of hilar hepatic masses, particularly in the presence of calcifications and infiltrative solid-cystic lesions. Reliance on imaging alone may lead to misdiagnosis as perihilar cholangiocarcinoma. Negative biliary cytology does not exclude either malignancy or parasitic disease, and early consideration of percutaneous or surgical biopsy is essential when diagnostic uncertainty persists.
Early recognition is crucial, as timely initiation of albendazole therapy combined with appropriate surgical management can significantly improve outcomes.
In conclusion, HAE should remain an important differential diagnosis for perihilar hepatic masses. Negative initial biopsies or serological tests should not definitively exclude the disease when clinical suspicion persists. Repeat targeted biopsy, particularly from viable peripheral tissue, may be necessary to establish the diagnosis. Greater awareness among clinicians, radiologists, pathologists, and surgeons is essential to reduce diagnostic delay and prevent misdiagnosis.
Footnotes
Ethical Considerations
Ethics approval was waived according to institutional policy. The manuscript complies with CARE guidelines.
Consent to Participate
A signed written informed consent was obtained prior to manuscript writing and submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.