
Abstract
Immune checkpoint inhibitors (ICIs) offer important clinical benefits in antitumor therapy. However, they may cause potential and unpredictable immune-related adverse events (irAEs) due to the non-specific immunity activation. Although adrenocortical insufficiency (AI) is a rare irAE, rapid identification and treatment can help patients avoid life-threatening cortisol crises. We describe the case of a 60-year-old Chinese male patient with liver cancer who developed intractable hyponatremia, fatigue, and loss of appetite three months after completing treatment with cadonilimab. Intravenous rehydration and symptomatic treatment were ineffective. The diagnosis of ICI-induced secondary AI was confirmed after refinement of cortisol levels and adrenocorticotropic hormone (ACTH). Additionally, mild subclinical hypothyroidism was identified as a concurrent endocrine finding. Electrolyte disturbances and general malaise improved markedly after oral administration of exogenous cortisol hormone. This case supports existing evidence regarding ICI-related secondary AI and highlights the importance of timely endocrine evaluation in patients with persistent hyponatremia and non-specific systemic symptoms.
Plain Language Summary
Cancer immunotherapy like cadonilimab can cause immune-related adverse events (irAEs), where may involve immune-mediated damage to endocrine axes, particularly the hypothalamic-pituitary-adrenal axis. We report a patient who developed a rare irAE called secondary adrenocortical insufficiency (AI), accompanied by subclinical hypothyroidism, after cadonilimab treatment for liver cancer. In secondary AI, the brain’s pituitary gland fails to signal the adrenal glands to produce cortisol, a vital hormone. This deficiency led to severe fatigue, nausea, and low sodium levels that didn’t respond to standard treatments. The diagnosis was confirmed through hormone tests, and the patient’s condition improved rapidly after starting cortisol replacement medication. This case adds to existing evidence that immune checkpoint inhibitors may cause secondary AI, and it underscores the need for timely endocrine evaluation when patients on immunotherapy present with persistent hyponatremia and non-specific symptoms such as fatigue and nausea.
Keywords
Background
Immune checkpoint inhibitors (ICIs) are crucial in the field of cancer immunotherapy by promoting the immune system’s recognition and destruction of tumor cells. This is achieved by targeting specific immune checkpoints, including cytotoxic T lymphocyte-associated antigen-4 (CTLA-4), programmed cell death protein 1 (PD-1), and programmed cell death-ligand 1 (PD-L1).1,2 However, immune-related adverse events (irAEs) are emerging as a common complication due to nonspecific immune activation, which refers to enhanced T-cell activity that may inadvertently recognize self-antigens in normal tissues, including endocrine organs such as the pituitary gland. 3 IrAEs may affect any organ system unpredictably and occur in 80-90% of treated patients. 4 Endocrine events are among the frequent manifestations of irAEs, affecting up to 40% of patients undergoing ICI therapy. 5
Cadonilimab is the first bispecific antibody targeting both PD-1 and CTLA-4 approved worldwide and is currently used in the treatment of various solid tumors, such as cervical cancer, liver cancer, and gastric cancers. 6 Benefiting from trans-binding and enhanced target binding avidity, cadonilimab demonstrates superior anti-tumor efficacy compared to CTLA-4 or PD-1 monotherapies alone. 7 Adrenocortical insufficiency (AI) is a rare but potentially serious irAE. Although secondary AI has been reported as an adverse event associated with cadonilimab and other ICIs, its clinical manifestations are often non-specific and may be overlooked in routine practice, particularly in patients with malignancy and multiple comorbidities. We present a case of intractable hyponatremia three months after cadonilimab treatment in a patient with hepatocellular carcinoma, who was ultimately diagnosed with secondary AI. This report aims to reinforce clinical awareness of endocrine irAEs and support existing evidence regarding the importance of early endocrine evaluation in patients receiving ICIs.
Case Presentation
A 60-year-old Chinese male patient presented to a local hospital on July 27, 2024 with nausea, vomiting, loss of appetite, and fatigue. Laboratory tests revealed the following: severe hyponatremia (serum sodium 117.9 mmol/L; reference range: 137-145 mmol/L), mild hypokalemia (serum potassium 3.4 mmol/L; reference range: 3.5-5.1 mmol/L), hypochloremia (serum chloride 90.4 mmol/L; reference range: 98-107 mmol/L), and hypoglycemia (serum glucose 3.0 mmol/L; reference range: 3.9-6.1 mmol/L). Hematological evaluation indicated leukopenia (white blood cell count 2.3×10^9/L; reference range: 3.5-9.5×10^9/L) and neutropenia (neutrophil count 1.0×10^9/L; reference range: 1.8-6.3×10^9/L), with hemoglobin at 104.0 g/L (reference range: 130-175 g/L), albumin at 38.8 g/L (reference range: 40-55 g/L), globulin at 17.5 g/L (reference range: 20-40 g/L), and platelet count at 124.0×10^9/L (reference range: 125-350×10^9/L). Despite receiving cautious intravenous fluid replacement with hypertonic saline (3% NaCl) and electrolyte correction in accordance with the European clinical practice guidelines for severe hyponatremia, 8 his symptoms did not improve. The patient was transferred to our hospital for further treatment on Aug 15, 2024.
The patient experienced hypertension for ten years, with the highest recorded blood pressure reaching 160/100 mmHg and received treatment with oral irbesartan 75mg daily. Recently, his antihypertensive medication was suspended due to low blood pressure. The patient was diagnosed with hepatocellular carcinoma in April 2023. After three interventional therapies, he underwent tumor immunotherapy, receiving injections of cadonilimab from April 28, 2023 to May 06, 2024 (once every 3 weeks, 6mg/kg). The patient’s cranial plain magnetic resonance imaging (MRI) on July 8, 2024 showed: empty sella turcica (a benign condition where the sella is filled with cerebrospinal fluid, often an incidental imaging finding but has occasionally been associated with pituitary dysfunction), bilateral involvement of the maxillary and ethmoid sinuses (inflammation of the mucosal lining of the facial sinuses and unrelated to endocrine dysfunction), and mastoiditis (inflammation of the mastoid air cells in the temporal bone and unrelated to immunotherapy-induced endocrinopathy); no other abnormalities were noted (Figure 1). In this case, no definite structural pituitary lesion was identified, although a potential association between empty sella and pituitary dysfunction could not be completely excluded. Cranial plain MRI. No abnormalities of the cranial structures were observed with no enlargement or reduction of the pituitary gland morphology. (A) Axial T1-weighted image; (B) Axial T2-weight image; (C) Sagittal T1-weight image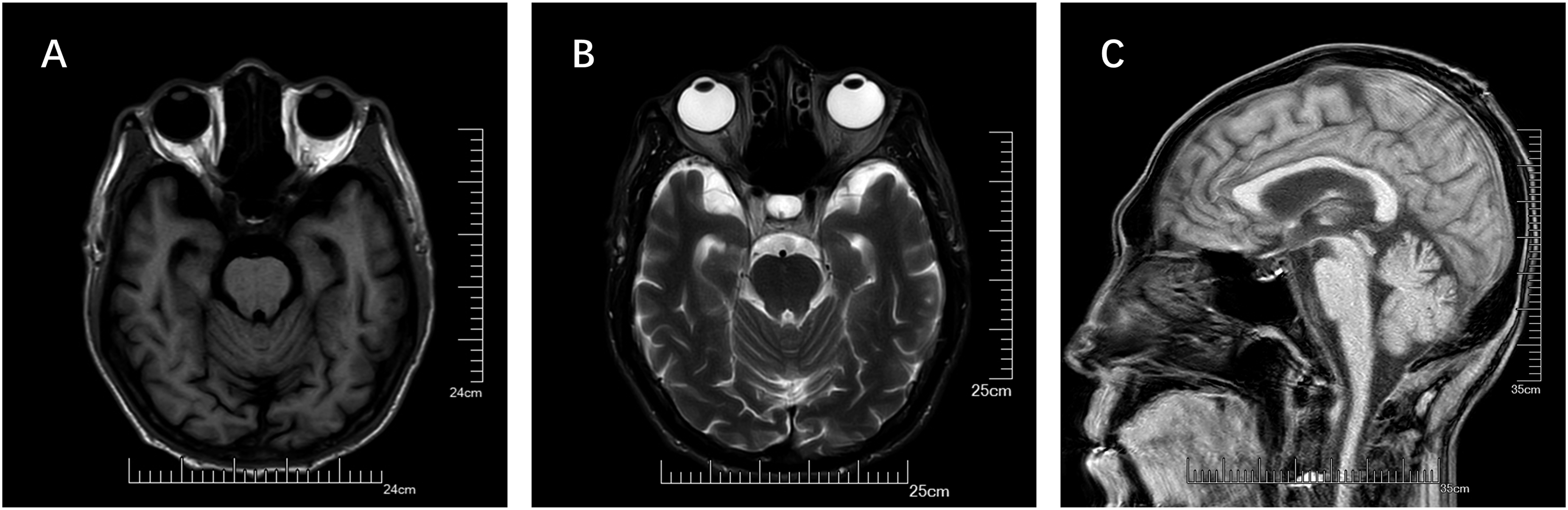
On admission, the patient was conscious, presenting with mild weakness and a mildly anemic appearance. Blood pressure was measured at 124/86mmHg with a heart rate of 65 bpm. Laboratory tests showed: severe hyponatremia (serum sodium 122.4 mmol/L; reference range: 137–145 mmol/L), hypochloremia (serum chloride 91.6 mmol/L; reference range: 98–107 mmol/L), hypoglycemia (serum glucose 3.3 mmol/L; reference range: 3.9–6.1 mmol/L), and hypoalbuminemia (albumin 37.2 g/L; reference range: 40–55 g/L). Serum potassium was 3.8 mmol/L (reference range: 3.5–5.1 mmol/L), and creatinine was 38.0 μmol/L (reference range: 44–104 μmol/L). Glycated hemoglobin was 4.0% (reference range: 4.0–6.0%). Hematological evaluation revealed anemia (hemoglobin 92.0 g/L; reference range: 130–175 g/L), leukopenia (white blood cell count 2.1×109/L; reference range: 3.5–9.5×109/L), neutropenia (neutrophil count 0.7×109/L; reference range: 1.8–6.3×109/L), and lymphopenia (lymphocyte count 0.9×109/L; reference range: 1.1–3.2×109/L). Platelet count was 130.0×109/L (reference range: 125–350×109/L). Urinary studies showed low urinary potassium (19.3 mmol/24h; reference range: 25–100 mmol/24h), while urinary sodium (211.2 mmol/24h; reference range: 130–260 mmol/24h) and urinary chloride (203.0 mmol/24h; reference range: 170–250 mmol/24h) were within normal limits. Further laboratory tests of endocrine function suggested the clinical suspicion of secondary AI: serum cortisol levels were severely depressed and lacked normal circadian rhythm (8 am: 0.37 μg/dL, 4 pm: 0.45 μg/dL, 12 am: 0.37 μg/dL; reference range at 6-10 am: 6.02-18.4 μg/dL, reference range at 4-8 pm: 2.68-10.5 μg/dL). Similarly, urinary free cortisol was markedly low at 0.74 μg/24h (reference range: 50-437 μg/24h). Concurrently, adrenocorticotropin (ACTH) levels were inappropriately low for the degree of hypocortisolemia (8 am: 3.38 pg/mL, reference range: 6-48 pg/mL; 4 pm: 3.27 pg/mL, reference range: 3-30 pg/mL), which is the diagnostic hallmark of secondary adrenal insufficiency.
9
In addition, Prolactin was elevated (38.55 ng/mL; reference range: 2.64–13.13 ng/mL). Thyroid function tests showed elevated thyrotropin (TSH) (5.8 mIU/L; reference range: 0.27–4.2 mIU/L), while free triiodothyronine (FT3) (1.9 pg/mL; reference range: 1.8–3.8 pg/mL) and free thyroxine (FT4) (0.9 ng/dL; reference range: 0.78–1.86 ng/dL) were within normal limits. Thyroid-related antibodies were negative. Computed tomography (CT) scan of abdomen showed: no abnormalities in both kidneys and adrenal glands (Figure 2). Abdominal CT. No definite abnormalities in adrenal morphology or size were identified. (A) Arterial phase; (B) Venous phase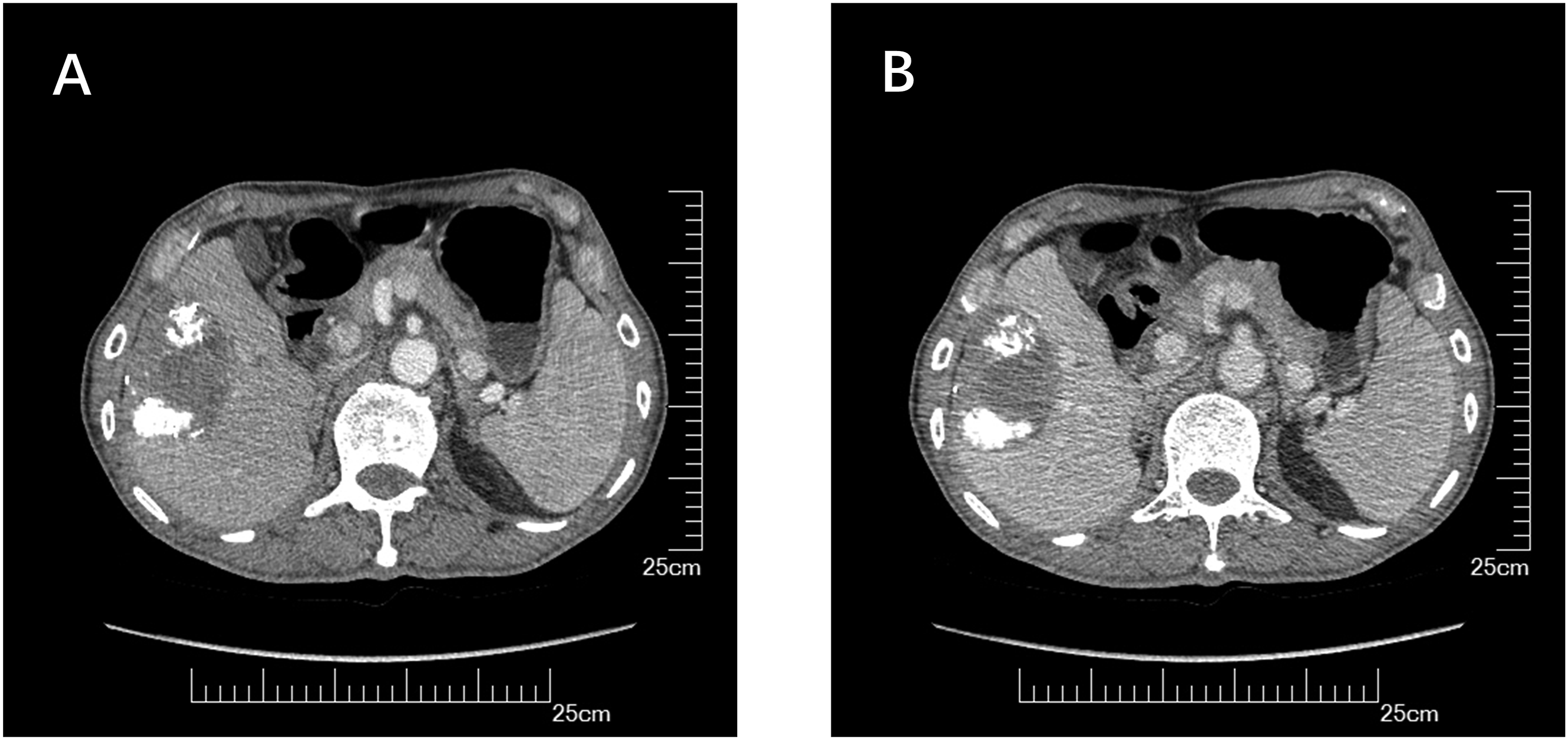
Electrolyte Results Before and After Patient Treatment

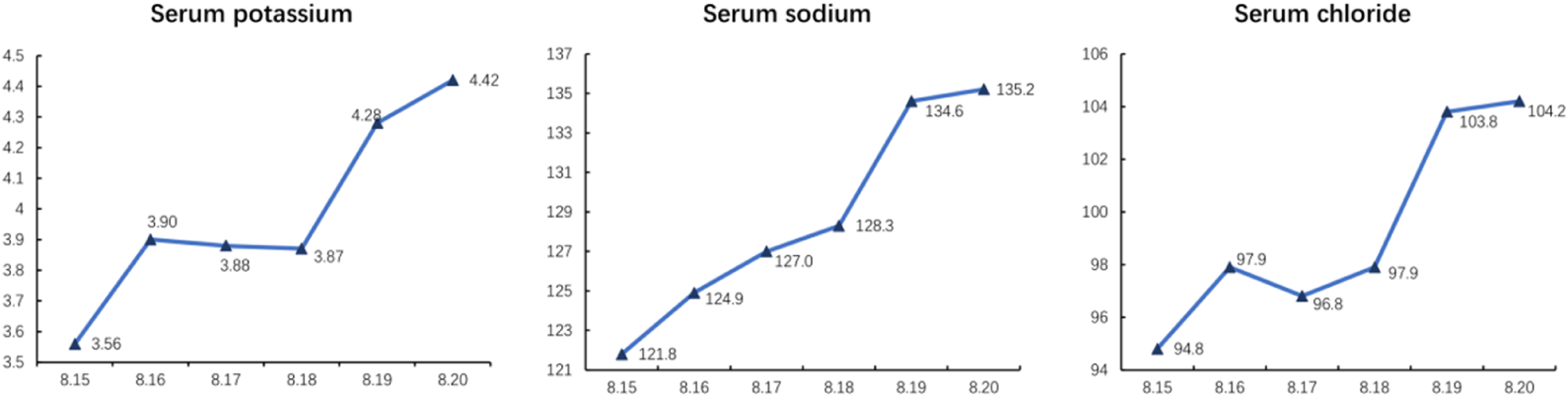
Electrolyte results before and after patient treatment. The patient was rehydrated intravenously to correct electrolytes from 15 August to 17 August. From 18 August onwards the patient suspended rehydration and was started on oral hydrocortisone. Unit: mmol/L
The patient was followed up at the endocrinology clinic every two months after discharge. During follow-up, the patient remained clinically stable, with normal electrolyte levels under continued hydrocortisone replacement therapy. At the last follow-up in August 2025, his serum electrolyte levels were normal (sodium 141 mmol/L, potassium 4.01 mmol/L, chloride 106.5 mmol/L). The hydrocortisone maintenance dose was tapered to 15 mg daily, and he remained free of nausea, vomiting, or fatigue. TSH was 4.66 mIU/L with normal FT3 and FT4, requiring no levothyroxine. Repeat imaging of the liver revealed no evidence of disease progression of the hepatocellular carcinoma. No adrenal crises occurred during the follow-up period.
Discussion
This case presented with intractable weakness, poor appetite, hyponatremia, and hypoglycemia three months following the completion of cadonilimab treatment, and symptoms did not improve despite symptomatic treatment. Further endocrine investigations showed cortisol rhythm test results (8 am-4 pm-12 am): 0.37-0.45-0.37μg/dL, ACTH test (8 am-4 pm): 3.38-3.27pg/mL. Combined with elevated prolactin levels and decreased urinary-free cortisol, a clear diagnosis of secondary AI was established. There was no history of oral exogenous hormone use, radiotherapy, or trauma in this case. Cranial MRI showed no significant abnormalities. Abdominal CT ruled out adrenal metastasis. Thus, cadonilimab treatment was considered the cause of his clinical manifestations.
Cadonilimab, an innovative bispecific antibody, blocks the interaction of PD-1 and CTLA-4 with their ligands PD-L1/programmed cell death-ligand 2 (PD-L2) and B7.1/B7.2, which prevents the immunosuppressive and promotes T-cell activation. 7 However, in addition to tumor cells, T-cells can cause autoimmune-like adverse events across various organ systems, contributing to the irAEs. Endocrine dysfunction is one of the most common irAEs, including thyroid disease, AI, and insulin-deficient diabetes mellitus. 11
Through a retrospective analysis of 1014 patients, Xiang J et al reported the prevalence of ICI-induced AI was 1.97%. 12 AI can manifest as primary, secondary, or mixed-type. 13 In a large-sample case study involving 206 patients with AI, there were 11 patients with primary AI, 191 patients with secondary AI, and 4 patients with mixed-type AI. 14 Damage to the adrenal cortex from ICIs results in primary AI, occurring at an incidence of 0.7% in monotherapy and 4.2% in combination therapy, which is rarer than secondary AI. 15 Secondary AI results from pituitary irAE-mediated ACTH deficiency, with a prevalence of 2.43% in monotherapy and 4.05% in combination therapy.16,17 The precise mechanism of secondary AI is currently unclear. Retrospective studies by Yano S and his colleagues at two centers have found specific human leukocyte antigen (HLA) markers, human leukocyte antigen-DR15 (HLA-DR15) closely associated with pituitary irAEs, potentially serving as predictive markers for secondary AI. 18 Additionally, type II and type IV hypersensitivity reactions may also contribute to pituitary irAE. 15 Several studies have suggested the incidence of ICI-induced AI appears to be higher in male patients, while the underlying mechanisms remain unclear and warrant further investigation. 19 The median time from the start of ICI treatment to the development of primary AI and secondary AI was 200.5 (35-280) days and 178 (16-562) days, respectively. 20
Besides pituitary impairment, ICIs can lead to adverse reactions in various endocrine glands, with thyroid dysfunction being the most prevalent irAE. 21 In this case, the thyroid stimulating hormone level was at the upper limit of normal, while other thyroid function tests were within normal ranges. As a result, subclinical hypothyroidism was considered to be present, which might be associated with the side effects of cadonilimab. Glucocorticoid supplementation followed by thyroxine supplementation is recommended, as administering thyroxine first can accelerate cortisol clearance and precipitate a life-threatening acute adrenal crisis. 22
The clinical symptoms of AI are non-specific, including general malaise, weakness, fatigue, poor appetite, hypoglycemia, postural hypotension, dizziness, nausea, vomiting, weight loss, and so on. 23 The clinical presentation and biochemical changes in AI are often non-specific, particularly in patients with cancer. Electrolyte disturbances caused by vomiting can also disrupt the diagnosis. Similar presentations characterized by hyponatremia and non-specific systemic symptoms have also been reported in patients with immune checkpoint inhibitor-associated adrenal insufficiency, emphasizing the diagnostic challenges of endocrine irAEs in clinical practice. 24 This case adds to the existing literature on immune-related adrenal insufficiency and underscores the importance of considering endocrine irAEs when encountering patients with persistent hyponatremia and non-specific systemic symptoms during or after ICI therapy. Notably, Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) was also considered in the differential diagnosis of hyponatremia in this patient, particularly given the relatively high urinary sodium levels and the presence of malignancy. However, the markedly decreased cortisol levels, inappropriately low ACTH levels, accompanying hypoglycemia, and rapid clinical and biochemical improvement following hydrocortisone replacement strongly supported secondary AI as the primary cause of hyponatremia.
Endocrine irAEs in patients receiving ICIs may present with non-specific manifestations such as persistent hyponatremia, fatigue, nausea, and poor appetite, which are more likely to be misattributed to disease progression or general debility, potentially delaying life-saving hormone replacement, thus highlighting the importance of continued endocrine surveillance. Complete endocrine-related laboratory tests are recommended to screen for the possibility of AI. Therefore, the National Comprehensive Cancer Network guidelines recommend checking morning cortisol levels every four weeks before or during ICI treatment. Follow-up checks are recommended for an additional six to twelve weeks. If cortisol levels are low or below normal, ACTH monitoring is recommended. 25
Conclusion
Our case reinforces the importance of early recognition and timely management of immune-related AI, a potentially life-threatening but treatable complication of ICI therapy. When clinicians encounter patients with persistent electrolyte disturbances and general malaise, not only during but also for several months after completion of ICI treatment, should consider timely and refined screening of ACTH and cortisol levels, which can assist in the early diagnosis and treatment of AI. Continued endocrine monitoring during and after ICI therapy may facilitate earlier recognition of immune-related endocrine dysfunction. Adrenal insufficiency, whether primary or secondary, presents a significant challenge in the context of ICIs due to its potential to drastically affect patient quality of life and treatment outcomes. Enhanced screening protocols, incorporating regular assessments of hormone levels, could mitigate the risk of overlooking this condition. This case supports previous reports of cadonilimab-associated secondary AI and reinforces the importance of recognizing atypical clinical presentations in routine practice.
Footnotes
Acknowledgements
We extend our gratitude to the patient for providing consent for this case report and for their cooperation throughout the process.
Ethical Considerations
This case report was approved by the Ethics Committee of The First Affiliated Hospital of Soochow University (number: 2024-573). All methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Wanqian Pan and Ge Wang were responsible for data collection and original draft writing. Xintao Li, Weixiang Chen, Xia Yin, and Tingbo Jiang performed literature review and clinical data interpretation. Yi Shang analyzed the imaging findings. Ke Chen contributed to manuscript revision and clinical discussion. Yingyi Zhou supervised the study and critically revised the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available within the article.