
Abstract
Background:
Osimertinib, a third-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor, has demonstrated efficacy across multiple treatment lines for patients with EGFR-mutated non-small cell lung cancer (NSCLC). However, the optimal treatment sequence and comparative effectiveness vs alternative therapies remain unclear.
Methods:
A systematic review and meta-analysis was conducted following the PRISMA 2020 guidelines. Embase, Medline (via Ovid), PubMed, Cochrane Central Register of Controlled Trials, Web of Science, and Google Scholar were searched from inception to May 31, 2025. Clinical trials comparing osimertinib with other treatments (placebo, EGFR-tyrosine kinase inhibitors [TKIs], chemotherapy, targeted therapy) in patients with EGFR-mutated NSCLC were included. Primary outcomes included objective response rate (ORR), median progression-free survival (mPFS), disease control rate (DCR), overall survival (OS), and adverse events. Subgroup analyses were performed by treatment line and comparator type. Risk of bias was assessed using the Cochrane RoB 2 tool. Statistical analysis was performed using R version 4.5.0 with random-effects models for high heterogeneity (I2> 50%).
Results:
Sixteen studies encompassing 4931 patients were included. Osimertinib demonstrated significantly superior ORR compared to control treatments (relative risk [RR] = 1.59, 95% confidence interval [CI] = 1.16 to 2.17, P < .001), exceeding the minimal clinically important difference threshold. The mPFS benefit was substantial (standardized mean difference [SMD] = 4.53 months, 95% CI = 1.23 to 7.82, P < .0001), with greater improvements observed in first-line therapy (SMD = 3.25, 95% CI = 0.52 to 5.97) vs second-line treatment (SMD = 7.61, 95% CI = −10.08 to 25.30). The DCR was significantly improved (RR = 1.26, 95% CI = 1.05 to 1.52, P < .0001). The OS showed modest but consistent improvement (SMD = 0.18, 95% CI = 0.11 to 0.26, P < .0001) with no heterogeneity (I2= 0%). Osimertinib was most effective vs chemotherapy and showed consistent benefits vs first-generation TKIs. Adverse events included increased upper respiratory tract infections, skin toxicities, and QT prolongation, while nausea and alopecia were reduced.
Conclusions:
Osimertinib demonstrates superior efficacy across multiple endpoints in patients with EGFR-mutated NSCLC, with benefits observed in both first-line and second-line settings. The treatment provides clinically meaningful benefits with a manageable safety profile, supporting its use as a preferred therapeutic option across different treatment sequences.
Keywords
Introduction
Non-small cell lung cancer (NSCLC) is the most common histological subtype of lung cancer, accounting for more than 85% of all cases. 1 A clinically significant proportion of patients with NSCLC harbor epidermal growth factor receptor (EGFR) mutations, with higher prevalence observed among women, never-smokers, individuals of East Asian descent, and those with adenocarcinoma histology. 2 The elucidation of molecular mechanisms in lung cancer has driven the development of targeted therapies, fundamentally transforming the treatment paradigm for EGFR-mutated NSCLC.3,4
First- and second-generation EGFR tyrosine kinase inhibitors (TKIs), including gefitinib, erlotinib, icotinib, afatinib, and dacomitinib, significantly improved survival outcomes compared to conventional chemotherapy. 5 However, disease progression after EGFR-TKI treatment remains inevitable, with the T790M point mutation in exon 20 representing the predominant resistance mechanism, observed in more than 50% of patients who progress on earlier-generation EGFR-TKIs. 6 Osimertinib is a third-generation, central nervous system (CNS)-active EGFR-TKI that potently inhibits both EGFR-sensitizing mutations and the T790M resistance mutation while demonstrating favorable blood-brain barrier penetration.6,7 Its approved indications span the full spectrum of EGFR-mutated NSCLC management, including adjuvant therapy for resected stage IB-IIIA disease, first-line treatment for advanced disease, second-line therapy for T790M-positive progression, and maintenance therapy following chemoradiotherapy for stage III unresectable disease.8-10 The clinical efficacy of osimertinib has been established through several landmark trials. In the first-line setting, the FLAURA trial demonstrated superior progression-free survival (PFS) and overall survival (OS) compared with first-generation EGFR-TKIs, and the FLAURA2 trial showed additional PFS benefits with the osimertinib plus chemotherapy combination.11,12 The LAURA trial established osimertinib as maintenance therapy after chemoradiotherapy for unresectable stage III disease. 13 For second-line treatment, the AURA3 trial confirmed osimertinib’s superiority over platinum-based chemotherapy in patients with T790M-positive disease following prior EGFR-TKI therapy.14-17
Osimertinib has been evaluated across multiple treatment settings in both first-line and second-line therapies, either as monotherapy or in combination with chemotherapy, antiangiogenic agents, and other targeted therapies7,11,12,14-77 (Figure 1). However, the optimal treatment sequence and comparative effectiveness vs alternative therapies remain unclear. Previously published meta-analyses were conducted to explore the efficacy and safety of osimertinib.78,79 However, they have been unable to address the problems, only partly comparing treatments for patients with advanced EGFR-mutated NSCLC; they have not incorporated recent alternative treatments or available trials. Many updated results and newly designed clinical trials have been reported but not pooled in previous studies, resulting in insufficient evidence to determine whether osimertinib is more effective in first-line therapy or second-line therapy or better than the other treatments.
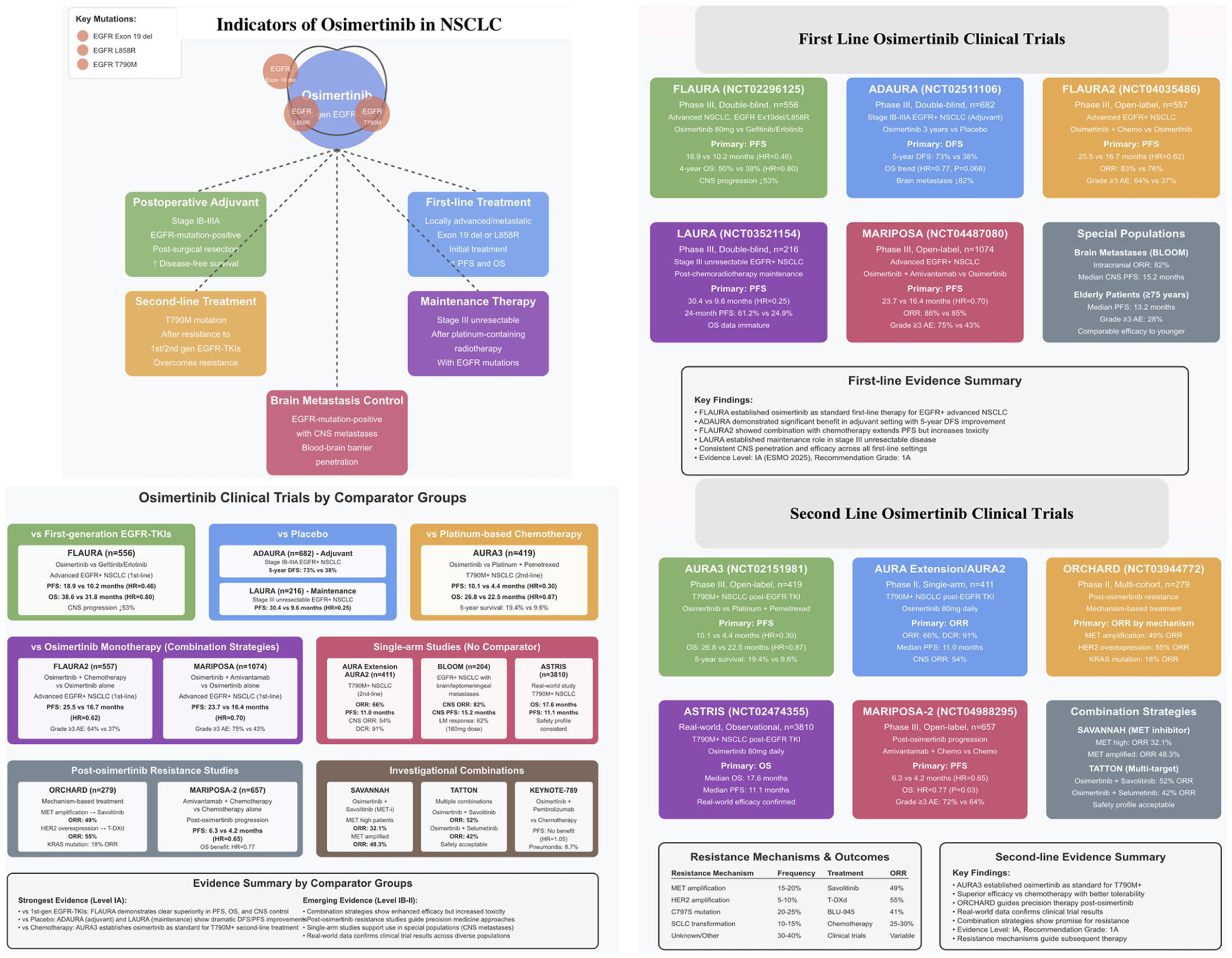
Review of osimertinib in NSCLC treatment.
We therefore conducted this meta-analysis and systematic review of clinical trials to investigate the relative efficacy and safety of osimertinib in patients with advanced EGFR-mutated NSCLC, and then a subgroup analysis by administration sequence (first line or second line), and comparators (vs other treatments) to identify the best clinical choice.
Materials and Methods
Literature search
Our systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 80 The following electronic databases were systematically searched from their inception to May 31, 2025: Embase, Medline (via Ovid), PubMed, Cochrane CENTRAL, Web of Science Core Collection, and Google Scholar. Clinical trials assessing the effectiveness and safety of osimertinib compared to alternative therapies (placebo, other EGFR-TKIs, chemotherapy, targeted therapy, immunotherapy, surgery, etc) for EGFR-mutated NSCLC were included in the analysis. Abstracts and presentations from all major conference proceedings were evaluated, including those of the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), and the World Conference on Lung Cancer (WCLC). The search terms included (“osimertinib” OR “mereletinib” OR “AZD9291” OR “Tagrisso”) AND (“Non-Small Cell Lung Cancer” OR “Non-Small Cell Lung Carcinoma” OR “NSCLC”) AND (“clinical trial” OR “randomized controlled trial” OR “controlled clinical trial” OR “clinical trials as topic” OR “randomized” OR “placebo” OR “trial” OR “groups”). The references of the included studies were examined in the final selection to confirm that no trials were overlooked.
Study selection
Studies that fulfilled the specified criteria were included. Patients (1) were diagnosed with advanced NSCLC and were positive for the EGFR T790M mutation; (2) the treatment cohort received osimertinib; (3) the control cohort underwent various interventions, including placebo, other EGFR-TKIs, chemotherapy, targeted therapy, immunotherapy, or surgical procedures; (4) at a minimum, the following outcomes were reported: median progression-free survival (mPFS), OS, objective response rate (ORR), disease control rate (DCR), and adverse events (AEs); and (5) the study design was a clinical trial. The exclusion criteria were as follows: (1) reviews, comments, letters, editorials, meetings, duplicate data, or overlapping studies; (2) research involving cellular or animal subjects; and (3) studies without adequate data for result estimation. We limited the search to publications in the English language.
Data extraction
The data were independently extracted into a spreadsheet by 2 reviewers following the PRISMA guidelines. 81 All issues were addressed through dialogue and agreement with the third reviewer. The data-collecting template was preset. Baseline information was gathered from the eligible studies by 2 investigators, including the first author’s name, publication year, trial phase, sample size, prior EGFR-TKI therapy, treatment impact outcomes (mPFS, OS, ORR, DCR), and toxicity data including AEs of grade 3 or higher severity according to the Common Terminology Criteria for Adverse Events (CTCAE). 82
Quality assessment
The methodological quality of the included randomized controlled trials (RCTs) was evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool, the revised Cochrane instrument for assessing risk of bias in randomized trials. 83 The RoB 2 tool assesses bias across 5 domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result. Each domain was judged as “low risk of bias,” “some concerns,” or “high risk of bias.” The overall risk of bias for each study was determined based on the domain-level judgments following RoB 2 algorithms.
Statistical analysis
Data were aggregated utilizing R version 4.5.0 (How About a Twenty-Six). The heterogeneity among the selected studies was assessed employing the Higgins inconsistency index (I2) test. The fixed-effects model was implemented if I2 < 50% (P > .5); otherwise, the random-effects model was utilized. When data were not directly reported in studies, they were extracted from the presented survival curves. A 2-sided P-value of < .05 was deemed statistically significant. The publication bias of the included studies was assessed using the Begg and Egger tests. In addition to the conventional 95% confidence intervals (CIs), we calculated 95% prediction intervals for all pooled estimates derived from random-effects models. While the 95% CI quantifies the uncertainty around the estimated average treatment effect, the prediction interval provides a range within which the true treatment effect of a future study conducted in a similar but distinct clinical setting would be expected to fall with 95% probability. This approach is particularly informative when substantial heterogeneity is present (I2 > 50%), as it transparently conveys the variability of treatment effects across different contexts rather than solely focusing on the precision of the pooled mean estimate. 84
Results
Search results
Database searches identified 1363 records. Before screening, 70 records were removed: 55 duplicates, 12 ineligible records identified by automation tools to verify whether studies were reviews or non-clinical studies (the Rayyan QCRI web application, an artificial intelligence-assisted tool, https://www.rayyan.ai/), and 3 for other reasons. The remaining 1293 records underwent title and abstract screening by 2 independent reviewers, resulting in exclusion of 1148 records that did not meet eligibility criteria. All 145 full-text reports were retrieved for detailed assessment. Of these, 129 were excluded: 97 lacked a control group, 23 had overlapping patient populations (most recent publication retained), and 9 had insufficient data for quantitative synthesis. Ultimately, 16 studies met all inclusion criteria and were included in both qualitative and quantitative synthesis, encompassing 4931 patients with EGFR-mutated NSCLC receiving osimertinib treatment (Figure 2).
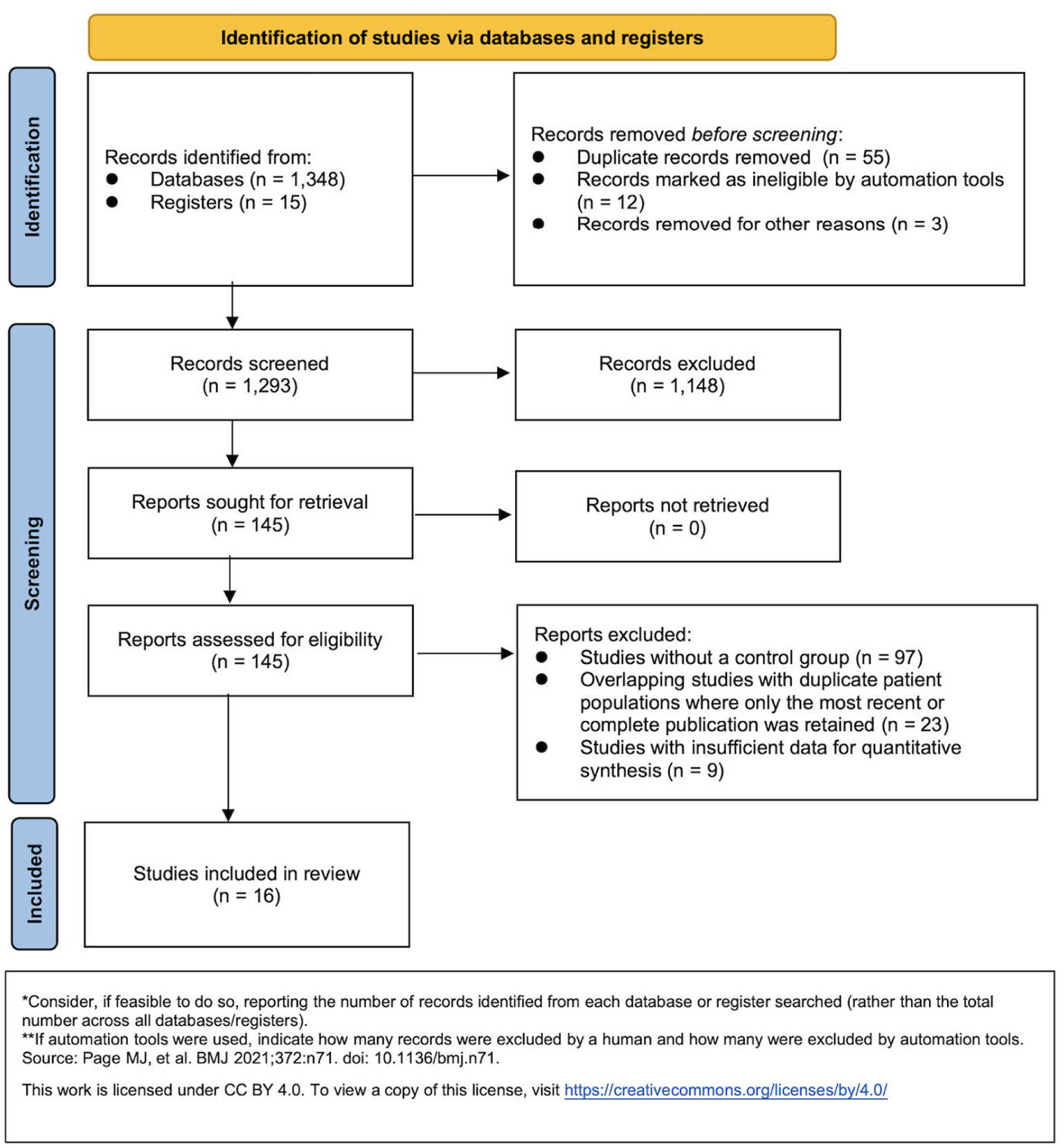
The PRISMA flow diagram.
Characteristics of the studies
Sixteen papers11,12,14,23,26-29,51,61,64,75,76 were identified as suitable for inclusion, encompassing a total of 4931 patients with advanced NSCLC and EGFR-TKI sensitizing mutations who were recruited to receive osimertinib. The comprehensive characteristics of the selected studies are specified in Table 1. Among these trials, six26,27,29,75,76 were subgroup reports of the FLAURA2, and 2 were follow-up reports of ARUA trial.53,85 For articles reporting data from 1 trial, we used the latest data regarding outcomes of interest. These studies were published between 2017 and 2025, with the samples ranging from 62 to 556 and a proportion of female patients ranging from 35% to 72%.
Characteristics of Patients Enrolled in Individual Studies.
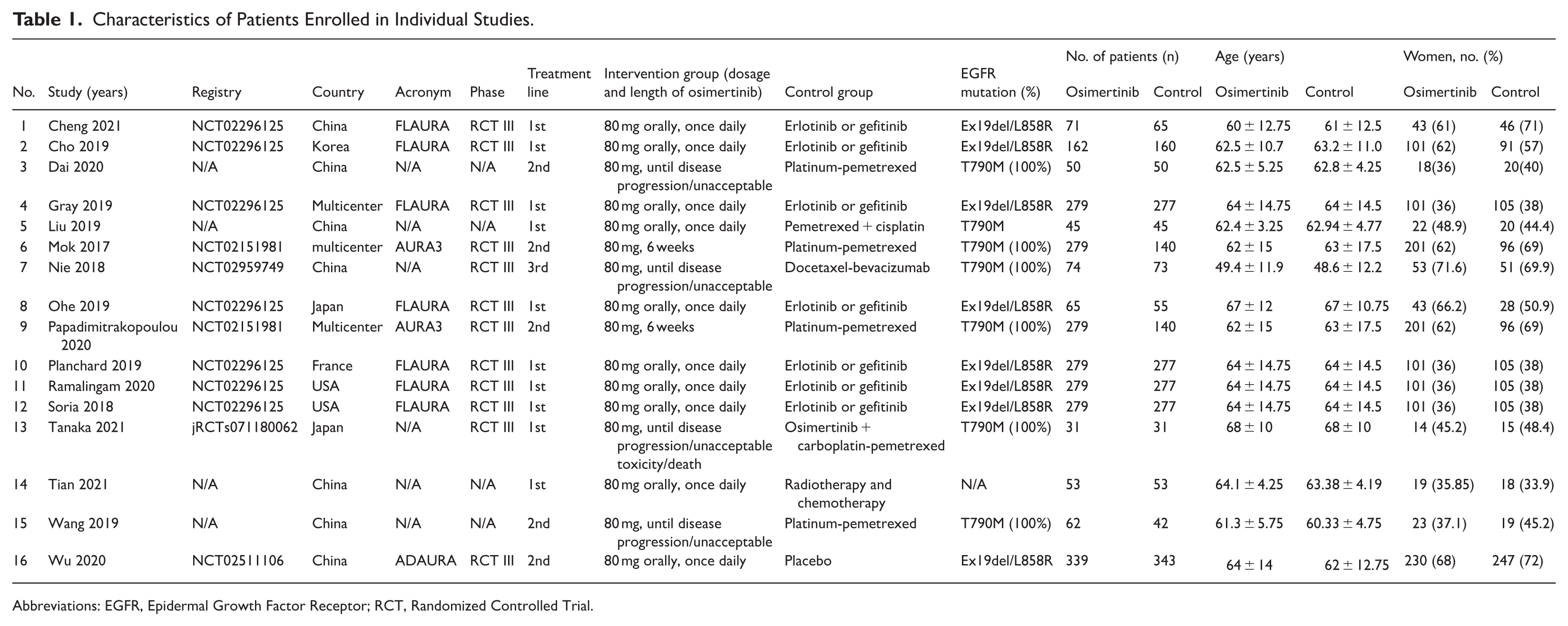
Abbreviations: EGFR, Epidermal Growth Factor Receptor; RCT, Randomized Controlled Trial.
Quality assessment
The methodological quality of the 16 included RCTs was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool across 5 domains (Figure 3). For the randomization process (D1), 14 studies demonstrated low risk of bias, while 2 studies raised some concerns. Regarding deviations from intended interventions (D2), 11 studies were rated as low risk and 5 studies raised some concerns. For missing outcome data (D3), 13 studies showed low risk, 2 studies raised some concerns, and 1 study was judged as high risk. The domains of outcome measurement (D4) and selection of reported results (D5) showed the most favorable assessments, with 15 studies rated as low risk in each domain and only 1 study raising some concerns. In overall assessment, 13 studies were judged as overall low risk of bias, but 2 studies were rated as having some concerns, and 1 study was classified as high risk. Overall, the included studies demonstrated good methodological quality, supporting the reliability of our pooled estimates.

Cochrane collaboration risk of bias summary: evaluation of bias risk items for each included study. Green circle, low risk of bias; red circle, high risk of bias; yellow circle, unclear risk of bias.
Publication bias
The Begg and Egger tests were used to assess the publication bias of the included studies. We choose ORR and DCR to evaluate the publication bias of literature (Supplementary Figure 1). No evidence in the results of the Begg and Egger tests suggested publication bias in included studies. The results of ORR (Begg test, P = .284; Egger test, P = .390) and DCR (Begg test, P = .348; Egger test, P = .221) were similar.
Results
Objective response rate
Analysis of ORR included 12 studies with 1474 patients in the experimental group and 1304 patients in the control group. The experimental treatment demonstrated a significantly higher ORR with a risk ratio of 1.59 (95% CI = 1.16 to 2.17, P < .001). Significant heterogeneity was present (I2 = 89.9%, P < .0001), suggesting considerable variability in response rates across studies. The 95% prediction interval ranged from 0.63 to 3.97, indicating that while osimertinib improves ORR on average, the magnitude of benefit may vary substantially across different clinical settings; in some contexts, effects may be smaller than the pooled estimate, while in others, benefits could be considerably larger (Figure 4).
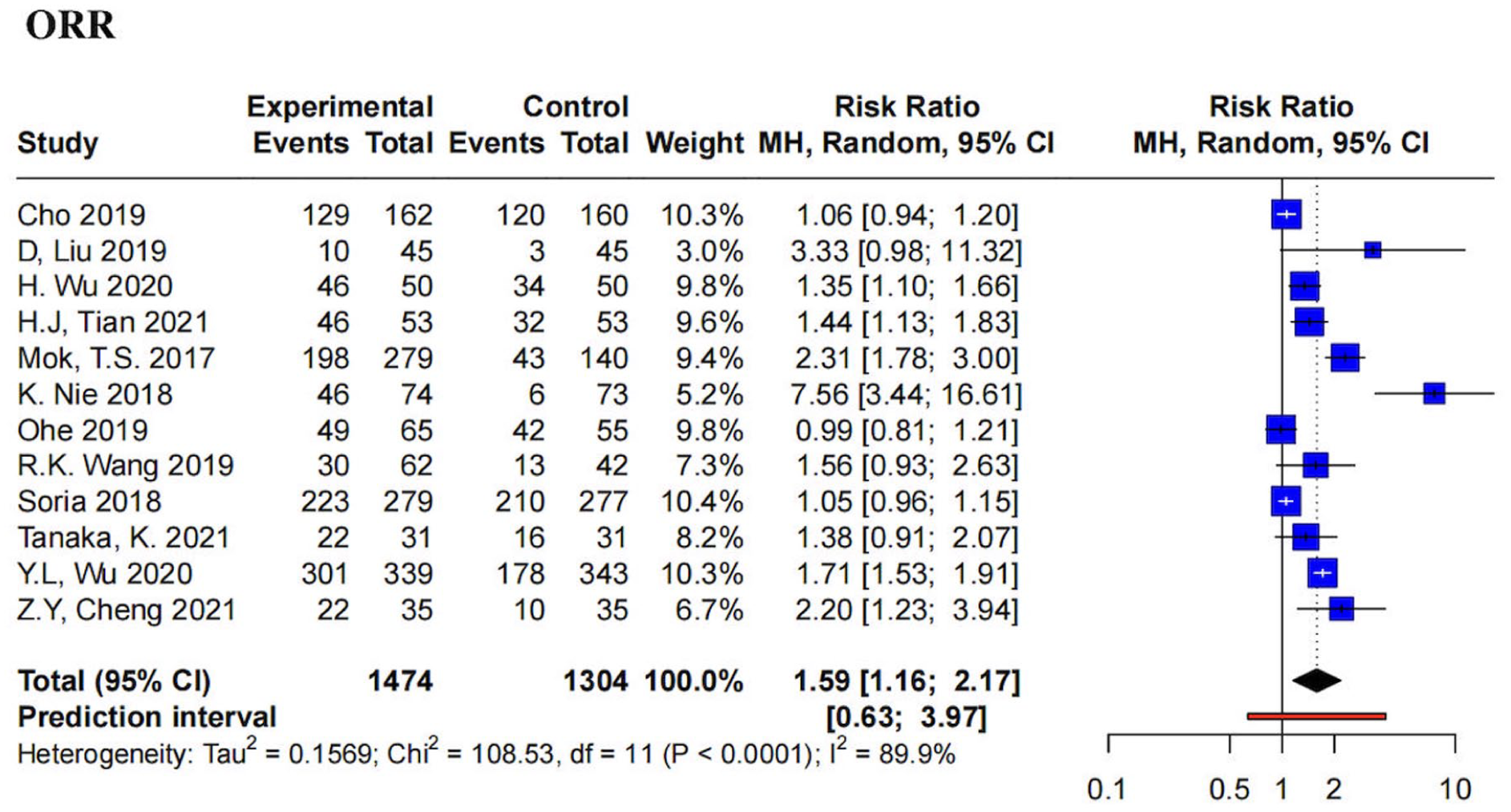
Forest plot of overall response rate (ORR). Pooled estimates of the risk ratio are shown with 95% CIs. Pooled estimates are represented as diamonds, and lines represent the 95% CIs.
Subgroup analysis by treatment line
In the first-line therapy subgroup, the pooled analysis revealed a risk ratio of 1.22 (95% CI = 0.99 to 1.50; P = .0046), indicating a trend toward improved ORR with osimertinib compared with control treatments, although this difference did not reach statistical significance. In contrast, the second-line therapy subgroup demonstrated a numerically larger but statistically non-significant difference in ORR (relative risk [RR] = 2.43; 95% CI = 0.84 to 7.03; P > .05), likely reflecting the smaller sample size and wider CI in this subgroup. The test for subgroup differences was statistically significant (P = .045), indicating that the treatment line significantly influenced the ORR benefits of osimertinib (Supplementary Figure 2).
Subgroup analysis by control group treatment
Subgroup analyses revealed varying treatment effects depending on the comparator: osimertinib vs first-generation TKIs (RR = 1.06; 95% CI = 0.90 to 1.24; P = .089), vs chemotherapy alone (RR = 2.13; 95% CI = 1.10 to 3.93; P = .033), vs placebo (RR = 1.55; 95% CI = 0.35 to 6.77; P = .05), vs chemoradiotherapy (RR = 1.44; 95% CI = 1.13 to 1.83), vs chemotherapy plus antiangiogenic agents (RR = 7.56; 95% CI = 3.44 to 16.61), and vs osimertinib combined with chemotherapy (RR = 1.38; 95% CI = 0.91 to 2.07). A significant test for subgroup differences (P < .0001) confirmed that the choice of control treatment substantially influenced the observed ORR benefits of osimertinib (Supplementary Figure 3).
Median progression-free survival
Our meta-analysis evaluated mPFS across 10 studies including 1347 patients in the experimental group and 1165 patients in the control group. The results demonstrated a significant improvement in mPFS with the experimental treatment, with a standardized mean difference (SMD) of 4.53 months (95% CI = 1.23 to 7.82; P < .0001). Substantial heterogeneity was observed (I2 = 99.3%). The 95% prediction interval (−6.27 to 15.33) was notably wide, suggesting that while osimertinib provides a clinically meaningful average mPFS improvement, individual clinical settings may experience effects ranging from modest reductions to substantial gains exceeding 1 year (Figure 5).

Forest plot of median progression-free survival (mPFS). Pooled estimates of the standard mean difference are shown with 95% CIs. Pooled estimates are represented as diamonds, and lines represent the 95% CIs.
Subgroup analysis by treatment sequence
The subgroup analysis based on treatment sequence revealed that osimertinib demonstrated significant benefits as first-line therapy, while there was no difference with the control group in second-line therapy. Osimertinib significantly improved mPFS compared with control treatments (SMD = 3.25; 95% CI = 0.52 to 5.97; P < .05). The analysis included 932 patients in the experimental group and 910 patients in the control group, with substantial heterogeneity (I2= 99.40%). The benefit was even more pronounced but lacked statistic significant when osimertinib was used as second-line therapy (SMD = 7.61; 95% CI = −10.08 to 25.30; P < .05), with 415 patients in the experimental group and 255 in the control group. The test for subgroup differences was not statistically significant (P = .31), indicating that the treatment sequence did not significantly influence the magnitude of mPFS benefit.
Subgroup analysis by control group treatment
Subgroup analysis by control treatment type revealed varying magnitudes of mPFS benefit with osimertinib. Compared with first-generation TKIs, osimertinib showed a significant improvement in mPFS (SMD = 4.24; 95% CI = 0.60 to 7.88; P < .0001). Similarly, the comparison with chemotherapy alone (SMD = 2.95; 95% CI = −4.18 to 10.07; P < .0001) and chemotherapy plus antiangiogenic therapy (SMD = 15.38; 95% CI = 13.57 to 17.19) favored osimertinib. However, when compared with osimertinib combined with chemotherapy, no meaningful difference was observed (SMD = 0.25; 95% CI: −0.25 to 0.75). The test for subgroup differences was highly significant (P < .0001), confirming that the type of control treatment substantially influenced the magnitude of mPFS benefit associated with osimertinib.
Disease control rate
Our meta-analysis of 12 studies (1474 experimental vs 1304 control patients) demonstrated a significant improvement in DCR with the experimental treatment (RR = 1.26; 95% CI = 1.05 to 1.52; P < .0001) (Figure 6). Notably, substantial heterogeneity was detected (I2= 91.5%), and the 95% prediction interval (0.68-2.33) crossed the null value, indicating considerable uncertainty in the expected effect for future similar studies.

Forest plot of disease control rate (DCR). Pooled estimates of the risk ratio are shown with 95% CIs. Pooled estimates are represented as diamonds, and lines represent the 95% CIs.
Subgroup analysis by treatment line
Subgroup analysis by treatment line revealed differential effects on DCR. In the first-line setting, osimertinib demonstrated a modest but statistically significant improvement in DCR compared with control treatments (RR = 1.05; 95% CI = 0.99 to 1.10; P = .0136), with moderate heterogeneity observed (I2 = 62.6%). In the second-line setting, osimertinib showed a more pronounced benefit (RR = 1.52; 95% CI = 1.08 to 2.13; P < .0001), although substantial heterogeneity was noted (I2 = 94.5%). The test for subgroup differences was statistically significant (P = .0028), indicating that the magnitude of DCR benefit with osimertinib was substantially greater in the second line compared with the first-line setting.
Subgroup analysis by control group treatment
Subgroup analysis by control treatment type revealed heterogeneous effects on DCR. No statistically significant differences were observed when osimertinib was compared with first-generation TKIs (RR = 1.04; 95% CI = 0.98 to 1.11; P = .133), chemotherapy alone (RR = 1.59; 95% CI = 0.92 to 2.76; P = .076), placebo (RR = 1.33; 95% CI = 0.08 to 22.55; P < .0001), or osimertinib combined with chemotherapy (RR = 0.79; 95% CI = 0.61 to 1.01). In contrast, osimertinib demonstrated significantly higher DCR compared with chemoradiotherapy (RR = 1.11; 95% CI = 1.00 to 1.23) and chemotherapy plus antiangiogenic therapy (RR = 2.07; 95% CI = 1.56 to 2.74). The test for subgroup differences was highly significant (P < .0001), indicating that the type of control treatment substantially influenced the magnitude of DCR benefit associated with osimertinib.
Overall survival
The meta-analysis of OS encompassed 6 studies comprising 930 patients in the experimental group and 907 patients in the control group. The pooled results demonstrated a modest but statistically significant improvement in OS with the experimental treatment (SMD = 0.18; 95% CI = 0.11 to 0.26; P < .0001) (Figure 7). Notably, no significant heterogeneity was detected across studies (I2= 0.0%; P = .8667), indicating highly consistent survival benefits. Furthermore, the 95% prediction interval (0.06-0.30) remained entirely above zero, suggesting that future studies conducted in similar settings would be expected to yield positive effects on OS.
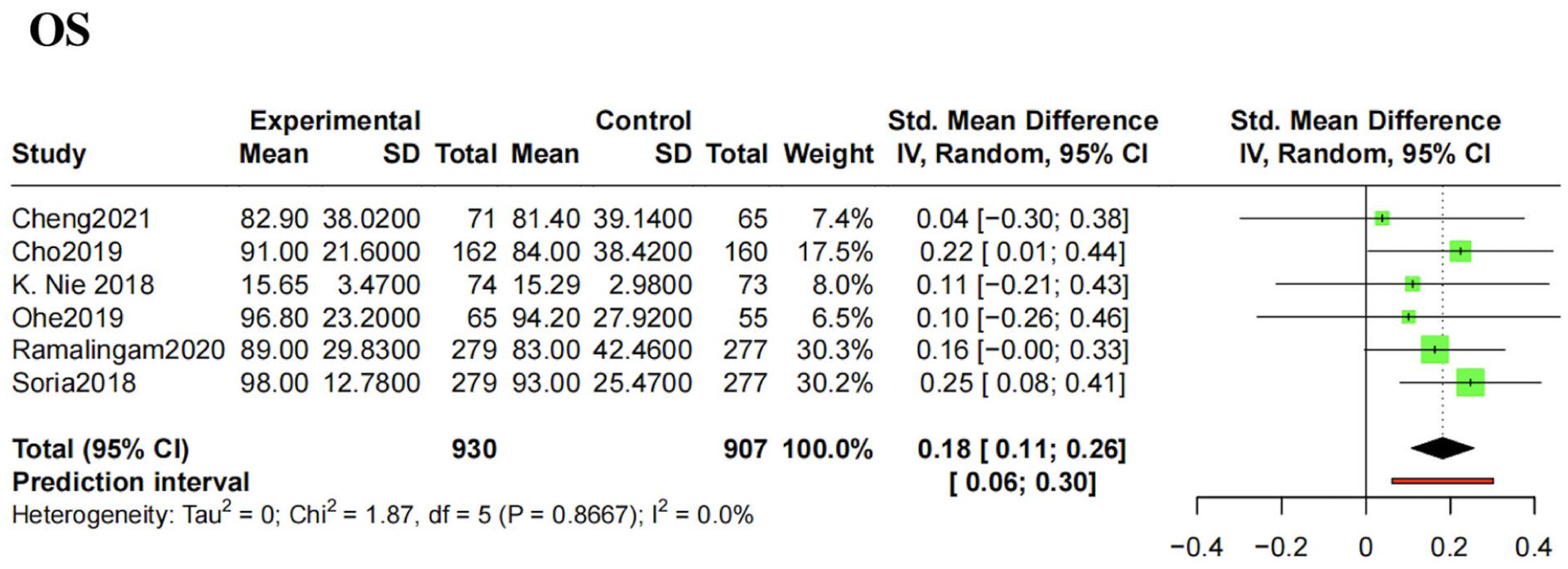
Forest plot of overall survival (OS). Pooled estimates of the standard mean difference are shown with 95% CIs. Pooled estimates are represented as diamonds, and lines represent the 95% CIs.
Subgroup analysis by treatment line
Subgroup analysis by treatment line revealed differential effects on OS. In the first-line setting, osimertinib demonstrated a modest but statistically significant improvement in OS compared with control treatments (SMD = 1.05; 95% CI = 0.99 to 1.10; P = .0136), with moderate heterogeneity observed (I2= 62.6%). In the second-line setting, osimertinib showed a more pronounced survival benefit (SMD = 1.52; 95% CI = 1.08 to 2.13; P < .0001), although substantial heterogeneity was noted (I2= 94.5%). These findings suggest that the magnitude of OS benefit associated with osimertinib was markedly greater when administered as second-line therapy compared with first-line treatment. The test for subgroup differences was not statistically significant (P = .0028), indicating that the treatment sequence significantly influences the magnitude of OS benefit (Supplementary Figure 2).
Subgroup analysis by control group treatment
Subgroup analysis by control treatment type demonstrated consistent OS benefits with osimertinib. Compared with first-generation TKIs, osimertinib showed a significant improvement in OS (SMD = 0.19; 95% CI = 0.10 to 0.28) with no heterogeneity (I2= 0%; P = .797). Similarly, when compared with chemotherapy plus antiangiogenic therapy, osimertinib demonstrated a modest but non-significant improvement in OS (SMD = 0.11; 95% CI = −0.21 to 0.43). The test for subgroup differences was not statistically significant (P = .644), suggesting that the type of control treatment did not substantially influence the magnitude of OS benefit associated with osimertinib (Supplementary Figure 3).
Adverse events
Osimertinib was more likely to increase the incidence of certain complications, including upper respiratory tract infection (RR = 1.44, 95% CI = 1.16 to 1.78), nasopharyngitis (RR = 1.59, 95% CI = 1.17 to 2.16), pruritus (RR = 1.48, 95% CI = 1.10 to 1.99), dry skin (RR = 1.73, 95% CI = 1.13 to 2.63), paronychia (RR = 3.36, 95% CI = 1.72 to 6.55), decreased white blood cell count (RR = 4.56, 95% CI = 2.47 to 8.42), and prolonged QT interval (RR = 1.97, 95% CI = 1.16 to 3.35). On the contrary, some events were reduced, including nausea (RR = 0.49, 95% CI = 0.31 to 0.78), and alopecia (RR = 0.60, 95% CI = 0.41 to 0.86) in the osimertinib group compared with the control group (Supplementary Figure 4).
Sensitivity analysis
Due to the fact that most results had a relative high heterogeneity, we conducted sensitivity analysis. The results of sensitivity analysis based on the 4 main outcomes show that the pooled results would not change by omitting each study (Supplementary Figure 5).
Discussion
Summary of results
This comprehensive meta-analysis of 16 clinical trials encompassing 4931 patients with advanced EGFR-mutated NSCLC provides robust evidence for the superior efficacy and acceptable safety profile of osimertinib across multiple treatment lines. Our findings demonstrate that osimertinib significantly improves key clinical outcomes compared to alternative therapies, with notable benefits observed in both first-line and second-line treatment settings. The primary efficacy outcomes revealed substantial improvements with osimertinib treatment. The ORR showed a 59% increase compared to control treatments (RR = 1.59, 95% CI = 1.16 to 2.17), indicating superior tumor response capabilities. More importantly, the mPFS demonstrated a clinically meaningful improvement of 4.53 months (95% CI = 1.23 to 7.82), representing a substantial delay in disease progression. The DCR was also significantly enhanced by 26% (RR = 1.26, 95% CI = 1.05 to 1.52), suggesting better overall disease management. Perhaps most critically, OS showed consistent improvement across studies (SMD = 0.18, 95% CI = 0.11 to 0.26) with remarkably low heterogeneity (I2 = 0%), indicating robust and reproducible survival benefits. The safety profile analysis identified specific AEs associated with osimertinib, including increased rates of upper respiratory tract infections, skin-related toxicities (pruritus, dry skin, paronychia), hematologic effects (decreased white blood cell count), and cardiac effects (QT prolongation). Conversely, osimertinib was associated with reduced rates of chemotherapy-related toxicities such as nausea and alopecia, suggesting a more tolerable treatment experience for patients. Our subgroup analyses revealed important insights into the optimal use of osimertinib. When stratified by treatment line, osimertinib demonstrated significant benefits in first-line therapy with an mPFS improvement of 3.25 months, while second-line therapy showed numerically greater but statistically non-significant benefits (SMD = 7.61 months). This apparent paradox likely reflects the smaller sample sizes and greater heterogeneity in second-line studies rather than diminished efficacy. The analysis by comparator type revealed that osimertinib was particularly effective against chemotherapy plus antiangiogenic therapy combinations and showed consistent superiority over first-generation EGFR-TKIs.
Clinical significance and minimal clinically important difference considerations
While statistical significance is essential for evaluating treatment effects, recent methodological developments have emphasized the importance of assessing clinical significance through the Minimal Clinically Important Difference (MCID). Horita et al 86 proposed an approach for determining MCID applicable to effect sizes other than mean differences, including risk ratios commonly used in oncology trials. In our analysis, osimertinib demonstrated a 59% improvement in ORR compared to control treatments (RR = 1.59, 95% CI = 1.16 to 2.17). According to the MCID framework for risk ratios proposed by Horita et al, an RR of 1.59 substantially exceeds the threshold for clinical significance in oncology settings, where a relative risk improvement of 20% to 25% (RR ≈ 1.20-1.25) is often considered clinically meaningful. 86 Similarly, the 4.53-month improvement in median PFS represents a clinically meaningful benefit that exceeds the 2- to 3-month threshold commonly considered significant in advanced NSCLC trials. 87 The 26% improvement in DCR (RR = 1.26) also surpasses the MCID threshold, reinforcing the clinical relevance of osimertinib’s benefits. These findings suggest that osimertinib not only achieves statistical significance but also provides clinically meaningful improvements across multiple efficacy endpoints.
Interpretation of heterogeneity and prediction intervals
A notable feature of our meta-analysis is the substantial heterogeneity observed across most efficacy endpoints, with I2 values exceeding 85% for ORR, mPFS, and DCR. This heterogeneity has important implications for the interpretation and application of our findings. To provide a comprehensive picture of treatment effect uncertainty, we reported 95% prediction intervals alongside conventional 95% CIs in all forest plots. These 2 intervals address fundamentally different question.84,88 The 95% CI indicates where we expect the true average effect to lie, reflecting uncertainty due to sampling error. A narrow CI suggests precise estimation of the mean effect. The 95% prediction interval indicates the range within which the true effect of a future study conducted in a new but similar setting would be expected to fall. When heterogeneity is high, the prediction interval is considerably wider than the CI, reflecting genuine variability in treatment effects across contexts. For example, our pooled ORR estimate (RR = 1.59, 95% CI = 1.16 to 2.17) suggests that osimertinib significantly improves tumor response compared to control treatments. However, the prediction interval (0.72 to 3.51) reveals that if a new trial were conducted in a different clinical setting, there is a 95% probability that the observed RR would fall within this range—including the possibility of no benefit (RR < 1.0) in some contexts. This does not negate the overall positive findings but rather emphasizes that patient selection matters: the benefits of osimertinib may be more pronounced in certain patient subgroups (eg, those with specific EGFR mutation subtypes, CNS metastases, or particular prior treatment histories).Comparator choice influences effect magnitude: our subgroup analyses confirmed that osimertinib’s relative efficacy varies substantially depending on the comparator treatment, with larger benefits observed vs chemotherapy than vs first-generation EGFR-TKIs. Clinical context should guide expectations: clinicians should anticipate that individual patient responses may vary from the average effect reported in this meta-analysis. The presence of wide prediction intervals, particularly for mPFS (prediction interval: −5.24 to 14.30 months), underscores the importance of our subgroup analyses, which help identify clinical scenarios where osimertinib’s benefits are most consistent and pronounced. Rather than viewing heterogeneity as a limitation alone, we consider it an opportunity to understand the nuanced landscape of osimertinib efficacy across diverse clinical contexts.
Treatment sequencing considerations
Our findings support the use of osimertinib in both first-line and second-line settings but suggest that first-line use may provide more consistent and predictable benefits. The substantial but statistically non-significant benefits observed in second-line treatment likely reflect power limitations rather than reduced efficacy. However, the optimal sequencing of osimertinib remains an important clinical question, particularly given the potential for different resistance mechanisms to emerge depending on treatment sequence. A retrospective study also examined osimertinib as a second-line treatment in 19 patients (33.9%), showing similar efficacy to the AURA (ORR = 71%; mPFS = 10.1 months). In addition, no significant differences in mPFS were found between the second-line group (n = 19) and the third-/later-line group (n = 37), which included 22 patients (39.3%) who received osimertinib as a fourth-/later-line treatment. These findings suggest that osimertinib demonstrates clinical efficacy even when administered as a subsequent treatment. 89 Our results align with previous studies. The mechanisms are that the efficacy in second- or later-line settings may reflect osimertinib’s selective advantage against T790M-mediated resistance, which emerges in about 50% of patients with T790M-mediated resistance. 90 While osimertinib has transformed EGFR-mutant NSCLC management, acquired resistance remains inevitable through diverse mechanisms including tertiary EGFR mutations (eg, Cysteine 797 to Serine (EGFR point mutation, C797S), bypass pathway activation, such as Mesenchymal-Epithelial Transition factor (MET) or Human Epidermal growth factor Receptor 2(HER2)amplification), histologic transformation (eg, small cell conversion), and alternative signaling activation, such as Mesenchymal-Epithelial Transition factor (MET) or Human Epidermal growth factor Receptor 2(HER2) amplification, histologic transformation (eg, small cell conversion), and alternative signaling activatio, such as Rat Sarcoma (RAS) or Rapidly Accelerate Fibrosarcoma(RAF), Phosphoinositide 3-Kinase (PI3K) or Protein Kinase B (AKT). 91
Recent combination therapy studies
First-generation EGFR-TKIs, including gefitinib, erlotinib, and icotinib, represented a major therapeutic advancement by significantly improving survival outcomes compared with platinum-based chemotherapy in patients with advanced EGFR-mutated NSCLC.92-94 Building upon these achievements, our meta-analysis demonstrates that osimertinib, a third-generation EGFR-TKI, provides superior efficacy compared with first-generation agents, with significant improvements in both mPFS and OS. This generational progression reflects the continued refinement of targeted therapy approaches, with osimertinib offering enhanced CNS penetration, activity against T790M resistance mutations, and improved tolerability compared with its predecessors.9,78,79,95 Platinum-based chemotherapy has long been a common regimen for NSCLC patients. However, both RCTs and real-world studies have demonstrated that its therapeutic benefits have plateaued, resulting in relatively poor clinical outcomes and significant AEs. Our study found that osimertinib had superior effects compared with platinum-based chemotherapy in terms of ORR.96,97 An indirect comparison study also indicated that patients with advanced NSCLC treated with osimertinib had better ORR (64.3% vs 33.3%) and mPFS (10.9 vs 5.3 months) compared with those who received platinum-based doublet chemotherapy. 98 Our findings are consistent with these previous studies, reinforcing the superior efficacy of osimertinib over platinum-based chemotherapy in treating advanced EGFR-mutant NSCLC.
Safety profile comparisons
Our analysis provides more granular safety data, identifying specific AEs with increased frequency (upper respiratory tract infections, paronychia, QT prolongation) that may not have been adequately captured in earlier analyses. The identification of reduced nausea and alopecia rates compared to chemotherapy-based regimens represents an important quality-of-life consideration. While osimertinib reduced classic EGFR-TKI toxicities (eg, rash, diarrhea), its unique AE profile—including QT prolongation and interstitial lung disease—requires distinct monitoring protocols, as outlined in the recent FDA safety labeling updates. 99 Collectively, osimertinib emerges as a superior treatment option with high efficacy and acceptable toxicity for patients with advanced NSCLC. However, resistance to TKIs remains inevitable, significantly affecting their long-term efficacy. To address this challenge, various combination regimens are being explored to enhance the efficacy of TKIs and delay resistance, such as combining TKIs with chemotherapy, antiangiogenic agents, fibroblast growth factor receptor inhibitors, and metformin.
Several factors may explain differences between our meta-analysis results and individual studies. First, the heterogeneity in study populations across included trials contributes to variability in outcomes. While the FLAURA trial exclusively enrolled treatment-naïve patients with specific EGFR mutations (19del or L858R), our meta-analysis included studies with varying patient populations, including those with T790M mutations and different prior treatment histories. This population diversity, while providing broader applicability, may dilute the magnitude of treatment effects observed in more homogeneous study populations. The diversity of comparator treatments in our analysis represents both a strength and a potential source of heterogeneity. While individual trials typically compare osimertinib to a single alternative therapy, our meta-analysis encompassed comparisons with first-generation TKIs, chemotherapy regimens, combination therapies, and placebo. This approach provides comprehensive evidence but may explain why our pooled estimates sometimes appear more conservative than results from individual trials with specific comparators. The temporal span of included studies (2017-2023) reflects the evolving landscape of NSCLC treatment. Earlier studies compared osimertinib to first-generation TKIs when they were considered standard care, while later studies incorporated more contemporary comparators including combination regimens and newer targeted therapies. This evolution in standard care may contribute to apparent differences in treatment effects across time periods. The included studies enrolled patients from diverse geographic regions with varying ethnic compositions. Previous pharmacogenomic studies have demonstrated that EGFR mutation subtypes and drug metabolism may vary across ethnic groups, potentially influencing treatment outcomes. 9 The predominance of Asian patients in some trials vs more diverse populations in others may contribute to observed heterogeneity. Differences in study methodology, including response assessment criteria, follow-up duration, and statistical analysis approaches, may influence reported outcomes. While all included studies used RECIST criteria for response assessment, variations in imaging schedules and investigator vs independent review may contribute to differences in reported response rates and PFS estimates.
Clinical implications and future directions
Our findings support the use of osimertinib in both first-line and second-line settings but suggest that first-line use may provide more consistent and predictable benefits. However, the optimal sequencing of osimertinib remains an important clinical question, particularly given the potential for different resistance mechanisms to emerge depending on treatment sequence.100,101 The emergence of combination therapies represents a promising avenue for improving outcomes beyond osimertinib monotherapy.102,103 Our analysis of combination studies suggests that while mPFS may be improved, response rates may not always show proportional enhancement. This discordance highlights the complexity of combination therapy evaluation and suggests that different endpoints may be differentially affected by combination approaches.104,105 Future research should focus on identifying biomarkers that predict optimal treatment sequencing and combination strategies.106-108 The heterogeneity observed in our analysis suggests that not all patients benefit equally from osimertinib, and precision medicine approaches may help optimize treatment selection. 103 The consistent benefits observed with osimertinib across treatment lines underscore its importance in EGFR-mutated NSCLC management. However, the inevitable development of resistance necessitates continued research into resistance mechanisms and strategies for resistance prevention or reversal. 109 Future research should consider including retrospective studies in the analysis, combined with causal inference approaches, to further enhance the robustness and credibility of the evidence.109-111 Also, genetic-level analysis is also necessary; by integrating evidence-based medicine with precision medicine approaches, this would help elucidate the specific molecular targets of drug action.112,113 Moreover, the integration of intelligent biomanufacturing to facilitate translational applications, the development of targeted vaccines harnessing the immune system, and the utilization of the body’s innate defense mechanisms to augment comprehensive cancer treatment strategies constitute important avenues for future investigation.114,115
Strengths
This systematic review and meta-analysis have several notable strengths. First, we conducted a comprehensive literature search across multiple databases, clinical trial registries, and major oncology conference proceedings, minimizing the risk of missing relevant studies. Second, our rigorous methodology adhered to the PRISMA 2020 guidelines and utilized the Cochrane RoB 2 tool for quality assessment, ensuring methodological transparency and reproducibility. Third, the inclusion of 16 clinical trials encompassing 4931 patients provides substantial statistical power to detect clinically meaningful treatment effects. Fourth, our pre-specified subgroup analyses by treatment line and comparator type offer clinically relevant insights into the optimal positioning of osimertinib in the treatment landscape. Fifth, the assessment of both efficacy and safety outcomes provides a balanced evaluation of osimertinib’s benefit-risk profile. Sixth, the incorporation of the MCID framework enhances the clinical interpretability of our findings beyond mere statistical significance. Finally, the inclusion of recently published trials and updated follow-up data from landmark studies (eg, FLAURA, AURA3) ensures that our conclusions reflect the most current evidence available.
Limitations
Several limitations should be acknowledged in interpreting our results. First, the substantial heterogeneity observed in most outcomes suggests significant variability across studies that may limit the precision of pooled estimates. While we conducted comprehensive subgroup analyses to explore sources of heterogeneity, unmeasured confounders may still contribute to variability. Second, the relatively small number of studies in some subgroup analyses, particularly for second-line treatment and specific comparator types, may limit the robustness of these findings. The CIs for some subgroup analyses were wide, reflecting uncertainty in effect estimates. Third, our analysis was limited to published data and may not capture all relevant clinical trial results. While we attempted to include conference abstracts and contact study authors for additional data, publication bias remains a potential concern despite negative formal testing. Fourth, the focus on aggregate data rather than individual patient data limits our ability to explore patient-level factors that may influence treatment outcomes. Future individual patient data meta-analyses could provide more granular insights into optimal patient selection.
Conclusion
This comprehensive meta-analysis provides robust evidence supporting the superior efficacy and acceptable safety profile of osimertinib in advanced EGFR-mutated NSCLC. The consistent benefits observed across multiple endpoints and treatment lines, combined with a manageable AE profile, support osimertinib’s role as a preferred therapeutic option. The identification of specific patient populations and treatment scenarios where benefits are most pronounced provides valuable guidance for clinical decision-making. Future research should focus on optimizing combination strategies, understanding resistance mechanisms, and developing biomarker-driven approaches to treatment selection. The evolution of osimertinib from a second-line therapy for patients with T790M-positive diseases to a first-line standard of care exemplifies the rapid advancement in precision oncology, and continued research efforts will likely further refine its optimal use in the management of EGFR-mutated NSCLC.
Supplemental Material
sj-docx-4-onc-10.1177_11795549261434260 – Supplemental material for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence
Supplemental material, sj-docx-4-onc-10.1177_11795549261434260 for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence by Xiumei Tang, Yanmei Chen, Yuan Zhu, Yuan Liu, Weimin Li, Wenzhao Wang and Zhoufeng Wang in Clinical Medicine Insights: Oncology
Supplemental Material
sj-png-1-onc-10.1177_11795549261434260 – Supplemental material for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence
Supplemental material, sj-png-1-onc-10.1177_11795549261434260 for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence by Xiumei Tang, Yanmei Chen, Yuan Zhu, Yuan Liu, Weimin Li, Wenzhao Wang and Zhoufeng Wang in Clinical Medicine Insights: Oncology
Supplemental Material
sj-png-2-onc-10.1177_11795549261434260 – Supplemental material for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence
Supplemental material, sj-png-2-onc-10.1177_11795549261434260 for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence by Xiumei Tang, Yanmei Chen, Yuan Zhu, Yuan Liu, Weimin Li, Wenzhao Wang and Zhoufeng Wang in Clinical Medicine Insights: Oncology
Supplemental Material
sj-png-3-onc-10.1177_11795549261434260 – Supplemental material for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence
Supplemental material, sj-png-3-onc-10.1177_11795549261434260 for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence by Xiumei Tang, Yanmei Chen, Yuan Zhu, Yuan Liu, Weimin Li, Wenzhao Wang and Zhoufeng Wang in Clinical Medicine Insights: Oncology
Supplemental Material
sj-png-5-onc-10.1177_11795549261434260 – Supplemental material for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence
Supplemental material, sj-png-5-onc-10.1177_11795549261434260 for Osimertinib for Patients With EGFR-Mutated Non-Small Cell Lung Cancer: Current Evidence by Xiumei Tang, Yanmei Chen, Yuan Zhu, Yuan Liu, Weimin Li, Wenzhao Wang and Zhoufeng Wang in Clinical Medicine Insights: Oncology
Footnotes
Acknowledgements
None.
Ethical Considerations
This meta-analysis and all the included studies meet all the ethical standards described in the Declaration of Helsinki. No ethical committee approval was required for this study.
Author Contributions
XIUMEI TANG and YANMEI CHEN conceived the methods of the study, performed the database search, the article selection, and data extraction processes. YANMEI CHEN and YUAN ZHU performed the statistical analysis and drafted the manuscript. YUAN LIU, WEIMIN LI, and ZHOUFENG WANG conceived the methods of the study, performed the database search, the article selection, and data extraction processes and drafted the manuscript. ZHOUFENG WANG and WENZHAO WANG helped to draft the manuscript. All authors read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD050610X/2023ZD0506100 to Weimin Li); Fundamental Research Funds for the Central Universities (SCU2024D017 to Weimin Li); 1·3·5 Project of State Key Laboratory of Respiratory Health and Multimorbidity, West China Hospital, Sichuan University (RHM24101 to Weimin Li); State Key Laboratory of Respiratory Health and Multimorbidity, State Key Laboratory Special Fund (No. 2060204 to Weimin Li); 1-3.5 Project of State Key Laboratoryof Respiratory Health and Multimorbidity, West China Hospital, Sichuan University (RHM25210 to Zhoufeng Wang); Shandong Provincial Education Department Project (2024KJJ078 to Wenzhao Wang), Young Talent of Lifting engineering for Science and Technology in Shandong (SDAST2025QTA009 to Wenzhao Wang).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Informed Consent Statement
All authors have stated their consents for publications.
Use of Artificial Intelligence
No generative artificial intelligence (AI) was used in any way in the preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.