
Abstract
Background
Glioblastoma (GB), or grade IV astrocytoma, is the most prevalent primary tumor of the central nervous system (CNS). This systematic review aimed to investigate the efficacy and tolerability of virotherapy treatment for recurrent and progressive glioblastoma patients. We also examined recent progress in preclinical and clinical trials, and future perspectives.
Methods
We developed a search strategy using Medical Subject Headings (MeSH) terms and keywords. Inclusion criteria were English language published and ongoing clinical trials that involved patients undergoing virotherapy for glioblastoma. We searched through PubMed, Embase, Ovid, Scopus, Cochrane databases and https://Clinicaltrials.gov from inception until May 9th, 2025. Two independent reviewers screened records, extracted data, and assessed risk of bias (ROB2). No meta-analysis was performed due to heterogeneity. PROSPERO CRD420250636791.
Results
Of 975 records screened, 43 studies (24 published, 19 ongoing) enrolled 462 virotherapy patients. Most common adverse events: headache (n=145), fatigue (n=83) and fever (n=78). Risk of bias was moderate to serious in most studies.
Conclusion
We encountered several limitations, including high heterogeneity, reporting inconsistencies, and small sample sizes. Most patients experienced disease stabilization. However, objective response and complete remission occurred infrequently. A small proportion of patients achieved long-term survival, suggesting that virotherapy could be effective in specific subgroups. While oncolytic virus therapy is generally tolerated, neurotoxicity remains the most significant risk. Adverse effects were mostly Grade 1–2. Some trials (notably with HSV-1 or NDV) had severe events. Symptoms were often transient and manageable but need closely monitoring. However, the observed heterogeneity, limited data standardisation, and lack of randomized controlled trials, besides tumor heterogeneity, antiviral immunity and immunosuppressive microenvironment, necessitate further research to identify predictive biomarkers and optimize therapeutic protocols. We also suggest further trials on novel delivery methods, such as the nanoparticles, to enhance blood-brain barrier (BBB) penetration.
Keywords
1. Introduction
Glioblastoma (GB), also known as grade IV astrocytoma, is the most prevalent primary tumor of the central nervous system (CNS),1,2 representing 14.5% of all CNS tumors and 48.6% of malignant CNS tumors. 1 GB incidence ranges from 3.19 to 4.17 cases per 100,000 person-years, with a median overall survival (OS) of 15 to 20 months and a five-year survival rate of only 5.8% following standard therapy, despite the standard therapy—maximal surgical resection followed by radiotherapy and temozolomide (TMZ). For recurrent disease, lomustine and bevacizumab are used, but outcomes have improved only modestly. 2 Hence, considerable efforts have been made in the past several years to increase survival rates and improve therapy outcomes.
Virotherapy (or oncolytic virus therapy) is a promising treatment for GB patients, as it is compatible with the unique characteristics of the brain environment, effectively targets rapidly proliferating tumor cells, and has a low risk of distant metastases. 3 While early studies suggested cancer regression following viral infection, initial efforts focused on the principle of ‘direct oncolysis'—using viruses as simple, targeted killing agents. However, the modern era has seen a fundamental transition toward ‘immuno-virotherapy’, where oncolytic viruses are engineered not only to destroy tumor cells directly but also to prime the host’s immune system for a sustained, systemic anti-cancer response. 4 Oncolytic virotherapy preferentially kills cancer cells in a 2-pronged approach: it directly infects and lyses cells, while acting as an immunogenic agent to stimulate an antiviral immunotherapeutic response. 5 The fundamental mechanism underlying virotherapy involves the enhancement of antigen-presenting cell (APC) function, which plays an essential role in immunogenic cell death (ICD), by facilitating the release of tumor-associated antigens (TAAs), damage-associated molecular patterns (DAMPs), viral pathogen-associated molecular patterns (PAMPs), and a variety of cytokines, ultimately leading to activation of cytotoxic CD8+ T lymphocytes (CTLs) and promoting an effective immune response against the tumor.3,6
However, GB tumor is an immunologically cold tumor, characterized by weak immune cell infiltration and inadequate control of tumor growth. In addition to the hypoxic niches which are part of the complex intrinsic microenvironment of the GB tumors that support the glioma stem cells, and further contribute to the tumor progression and immunosuppression. 7 Multiple mechanisms are responsible for the T-cell dysfunction in the GB microenvironment which include tolerance, exhaustion, and anergy. Moreover, tumor-associated macrophages produces indoleamine which exacerbates T-cell exhaustion. These exhausted T-cells reduce cytokines production and low functional capabilities. 8 Recent studies demonstrated that oncolytic virotherapy could expand pre-existing tumor-infiltrating T-cells that were formerly exhausted, causing persistent T-cell activation against tumor cells. 9
In addition to intratumoral heterogeneity, the glioblastoma microenvironment itself represents a major obstacle to effective virotherapy. Glioblastoma is characterized by a highly immunosuppressive milieu involving regulatory T-cells, tumor-associated macrophages, and inhibitory cytokines such as TGF-beta and IL-10, all of which may restrict viral replication and limit antitumor immune activation. Moreover, structural factors including abnormal vasculature and dense extracellular matrix components may further impair viral dissemination within the tumor tissue. These challenges have prompted the development of genetically engineered viral vectors designed to improve tumor selectivity, evade premature immune clearance, and enhance intratumoral spread.10,11
Furthermore, Both cancer cells and viral replication share similar metabolic hallmarks (the Warburg effect), including increased glycolysis, lactic acid production, activation of the pentose phosphate pathway (PPP), glutaminolysis, and altered lipid metabolism. 12 Both DNA and RNA viruses can modify the host’s central carbon metabolism by enhancing glycolysis and increasing pentose phosphate pathway activity to produce nucleotides, amino acids, and lipids. While many viruses boost the uptake of nutrients like glucose and glutamine and activate similar anabolic pathways, the specific metabolic changes can vary depending on the virus, its family, and the host cell type.13,14 On the other hand, these metabolic changes in cancer cells’ environment disrupt the antiviral defence system (interferon, cell arrest, apoptosis and immune activation), which along with disorganized tissue architecture, loss of intracellular contacts, leaky tumor vessels and abundance of surface penetration receptors, all make cancer cells susceptible to viral replication. 15
Additionally, virulence (a virus’s ability to harm the infected host) can differ from one virus group to another. Viral virulence is encoded in the viral genome and expressed through attenuation in any structural proteins, nonstructural proteins, or noncoding sequences, and can be altered by very small changes in the genome, if they occur at critical sites, for instance a specific amino acid or base site. These attenuating mutations are often host range mutations that affect replication in some cells but not in others. As an example, Reovirus type 1 (Lang) disseminates through the blood and causes an ependymitis in the brain while type 3 (Dearing) disseminates through the neural route and causes a neuronotropic encephalitis in the brain. Differences in the comparative replication of two virus variants can account for their relative degrees of virulence. Attenuated variants usually will replicate or spread less rabidly in one or several tissues associated with the pathogenic process. 16 Viral growth rate, the effectiveness of immune cells to kill infected cells, speed of immune activation, formation of memory cells, and longevity of immune cells all determine the cumulative viral load (time-integral of the number of infected cells). 17 The study of virulence variants can provide important insights into pathogenesis, and carries the potential for development of attenuated live virus variants and immunotherapy.
The objective of this systematic review is to elucidate the potential use of various oncolytic viruses and their fragments in the treatment of GB. While a recent systematic review by Winkler et al., 2023, 18 explored the clinical progress of oncolytic virotherapy in glioblastoma, there remains a lack of focused analysis on the safety and toxicity profiles of these treatments. Our review specifically focuses on this by systematically synthesizing evidence on side effects and tolerability. We synthesized both published research and forthcoming clinical trials to evaluate the efficacy and safety of oncolytic viruses in reducing tumor cell proliferation, inducing apoptosis, and augmenting immune responses against CNS tumors. Additionally, we examine associated adverse effects and identify future directions for research.
2. Methods
This systematic review was carried out under the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA). 19 The study was prospectively registered on PROSPERO (CRD420250636791). The main objective was to investigate the safety and tolerability of virotherapy treatment, primarily for glioblastoma patients. The review protocol is available from the corresponding author upon reasonable request. No amendments to the protocol were made.
2.1 Inclusion and Exclusion Criteria
2.2 Data Search and Screening
We systematically searched PubMed, Embase, Ovid, Scopus, Cochrane databases, and https://ClinicalTrials.gov from their respective dates of inception through May 9th, 2025 (the date the search was executed), using the following Medical Subject Headings (MeSH) terms and keywords. The full search strategy is also provided in Supplementary File. For multiple publications from the same phase trial, we used the most recent/complete report. For separate studies with suspected patient overlap, we extracted data from the largest or longest-follow-up cohort and documented overlaps narratively; unresolved overlaps were grouped for qualitative synthesis without additive counting.
Two independent reviewers, who worked independently, performed preliminary title/abstract and full-text screening, and conflicts were solved by mutual agreement. We used the Rayyan tool in the screening process. The PRISMA flowchart summarizes the study screening and selection process (Chart 1). PRISMA flow diagram showing our search strategy and the screening phase. Eventually, 43 trials were included (24 published, 19 ongoing trials)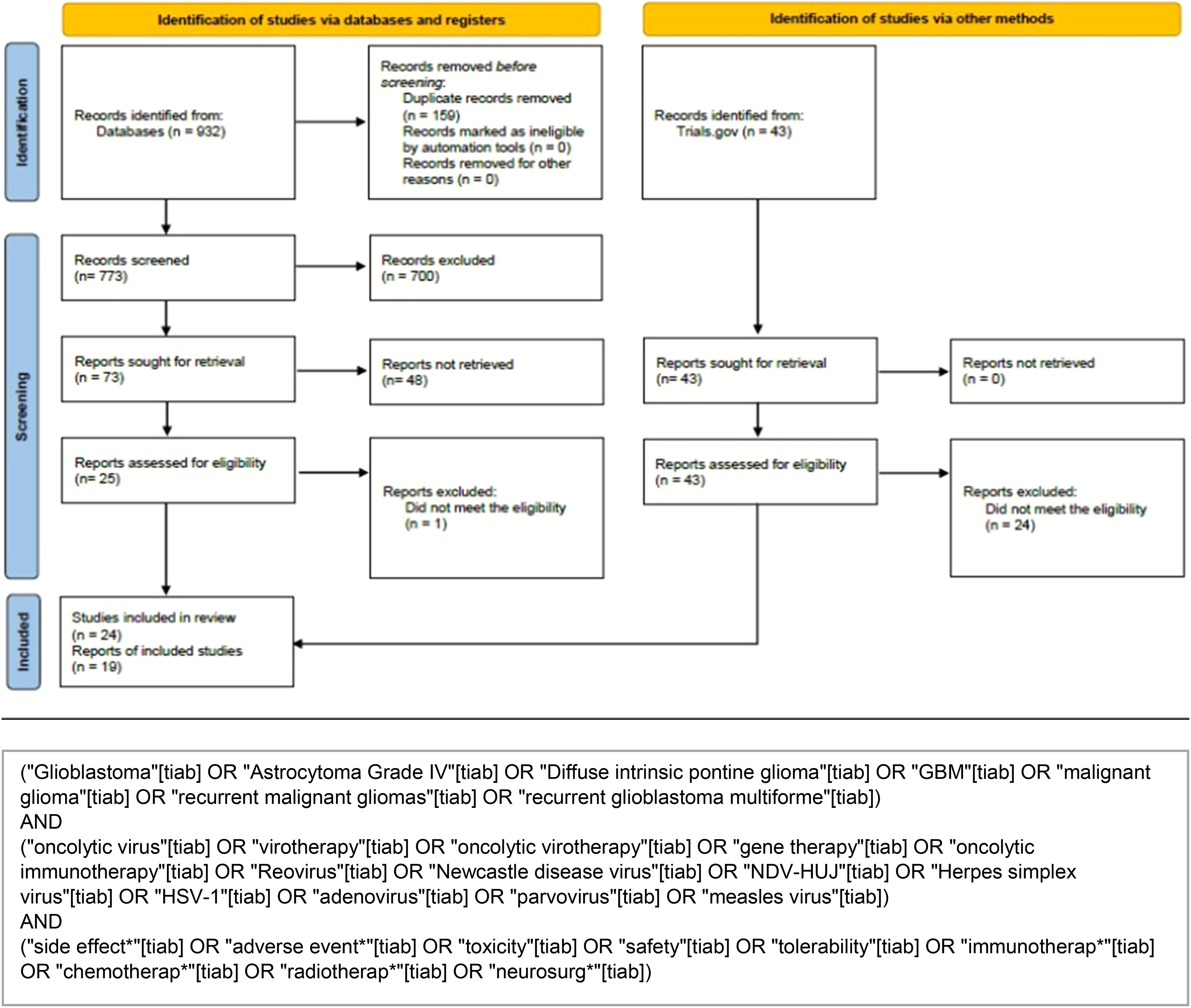
2.3 Data Items
We sought the following primary outcomes: safety and tolerability, measured by incidence and grade of adverse events (CTCAE criteria). Secondary outcomes: overall survival (OS, months), progression-free survival (PFS, months), objective response rate (ORR, %). Other variables extracted: participant age, Karnofsky Performance Status (KPS), prior treatments (chemotherapy, radiotherapy, surgery, specific agents), virus type, dose, administration route, and study phase. When data were missing or unclear, we did not impute values but noted the absence in tables.
2.4 Study Risk of Bias Assessment
The internal validity of the included studies was assessed independently by two reviewers. Any disagreements were resolved by consensus or through consultation with a third reviewer. We used the Cochrane RoB 2.0 tool, which assesses bias across five domains: (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result. For each domain and each study, we assigned a judgment of “Low risk,” “Some concerns,” or “High risk” (or “Low,” “Moderate,” “Serious,” “Critical,” as appropriate for the tool). A summary of the risk of bias for each study is presented in (Fig1/Summary Table7).
2.5 Effect Measures
For OS and PFS, we extracted medians and ranges. For adverse events, we calculated proportions (events per 100 patients). For response outcomes we reported frequencies. No meta-analysis was performed, so pooled effect estimates (e.g., risk ratios) were not calculated.
2.6 Data Synthesis
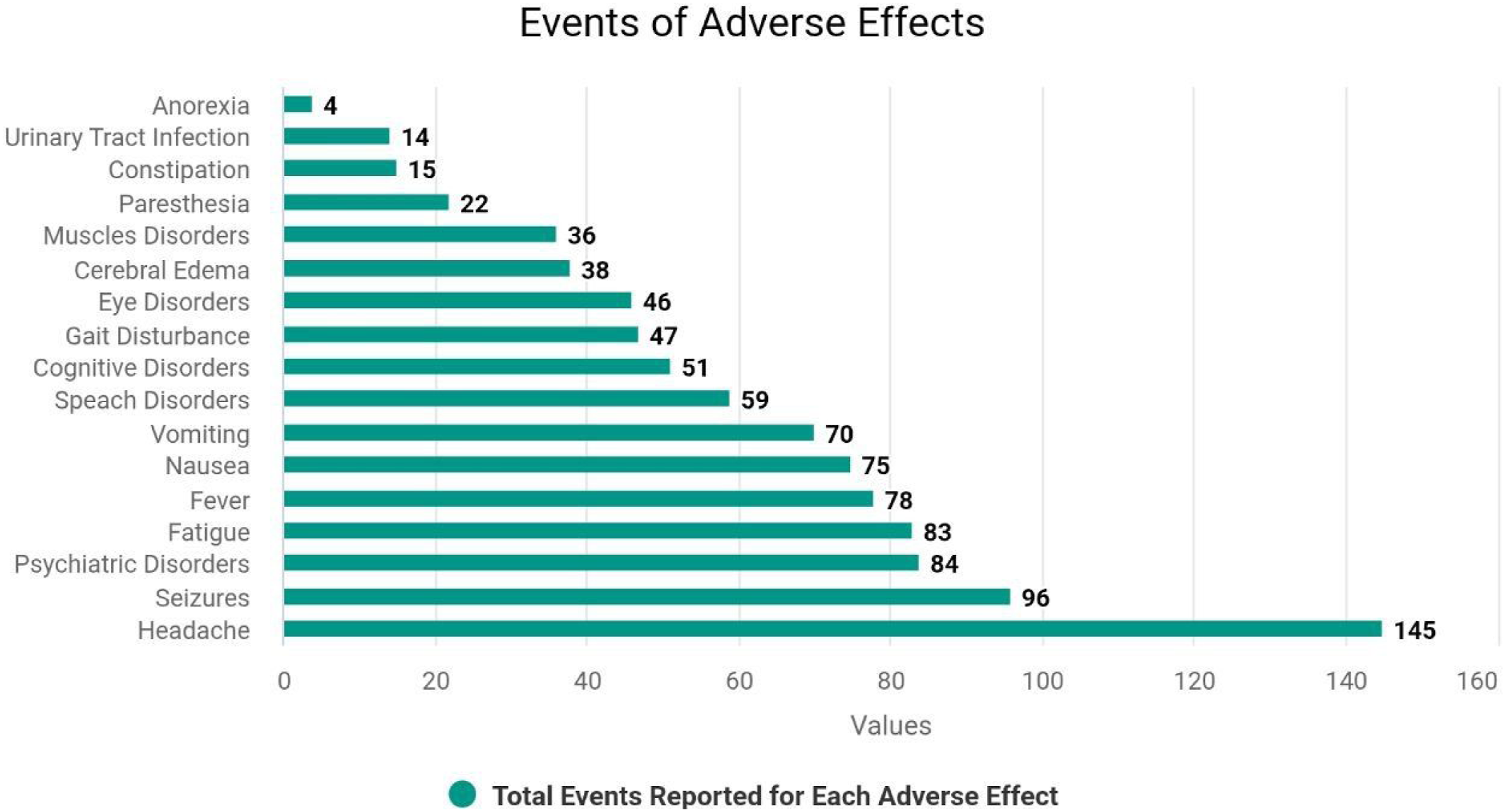
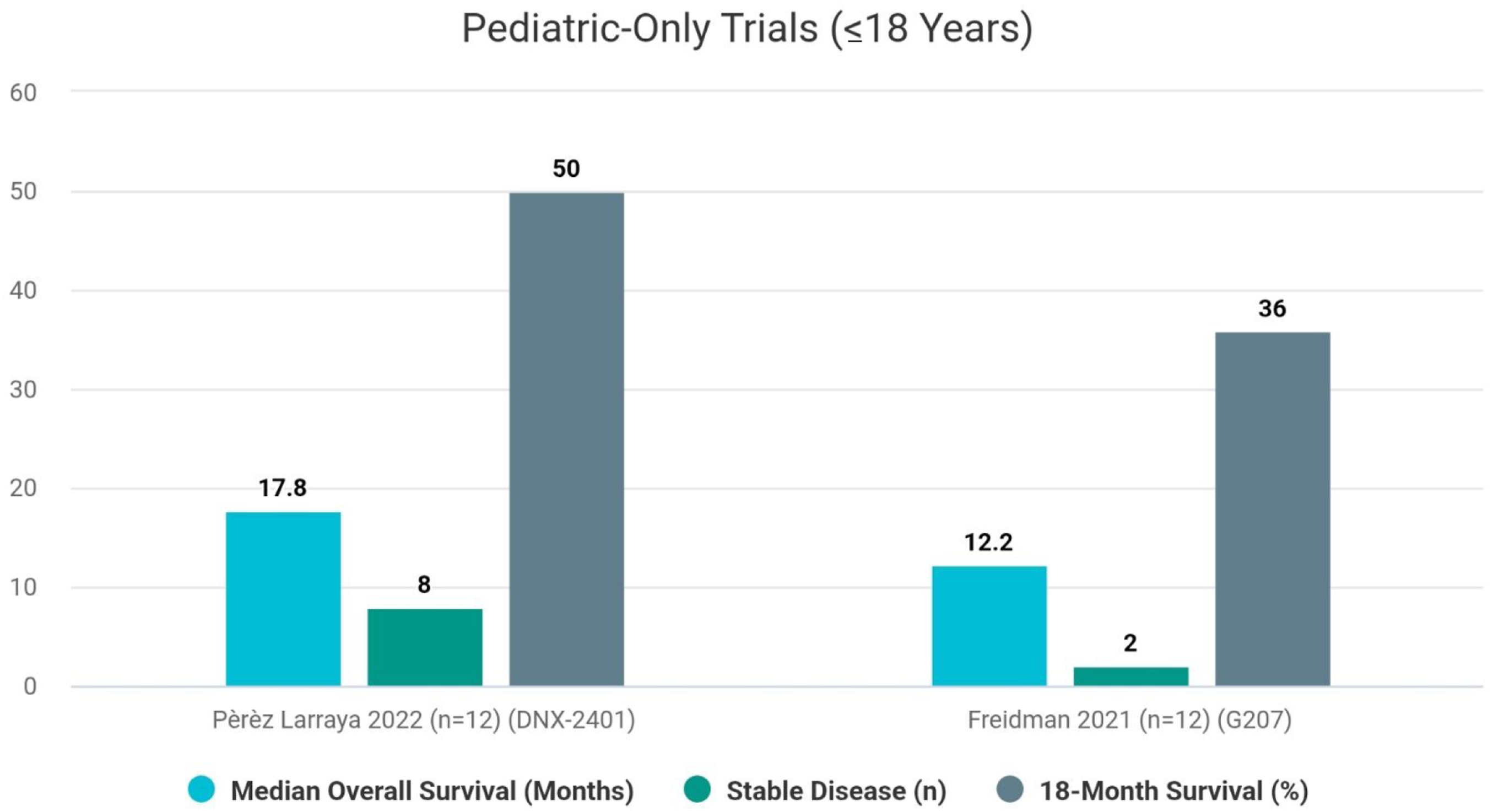
Studies were grouped for synthesis by virus class (HSV-1, adenovirus, reovirus, measles, poliovirus, parvovirus, NDV) and by age (adult vs pediatric), based on the prespecified subgroups (Item 5). Missing summary statistics (e.g., standard deviations) were not imputed; we reported available data only. No data conversions were performed. Results were tabulated in structured tables Number of studies for each previous treatment. Cht: Chemotherapy, RT: Radiotherapy, TMZ: Temozolamide, BEV: Bevacizumab Total events reported across all the 24 published trials for each adverse effect. General effects (e.g., headache, fever and fatigue) along with seizures and psychiatric disorders had the most events Main outcomes for pediatrics-only trials. We noticed that both trials included the same sample size; however, Larraya et al., who studied DNX-2401 (Adenovirus) had higher survival and SD cases Total number of patients compared to the total number of adverse events that occurred for each virus class included in the study. Adenovirus and HSV-1 had a similar No. of patients, but a significant difference in side effect incidences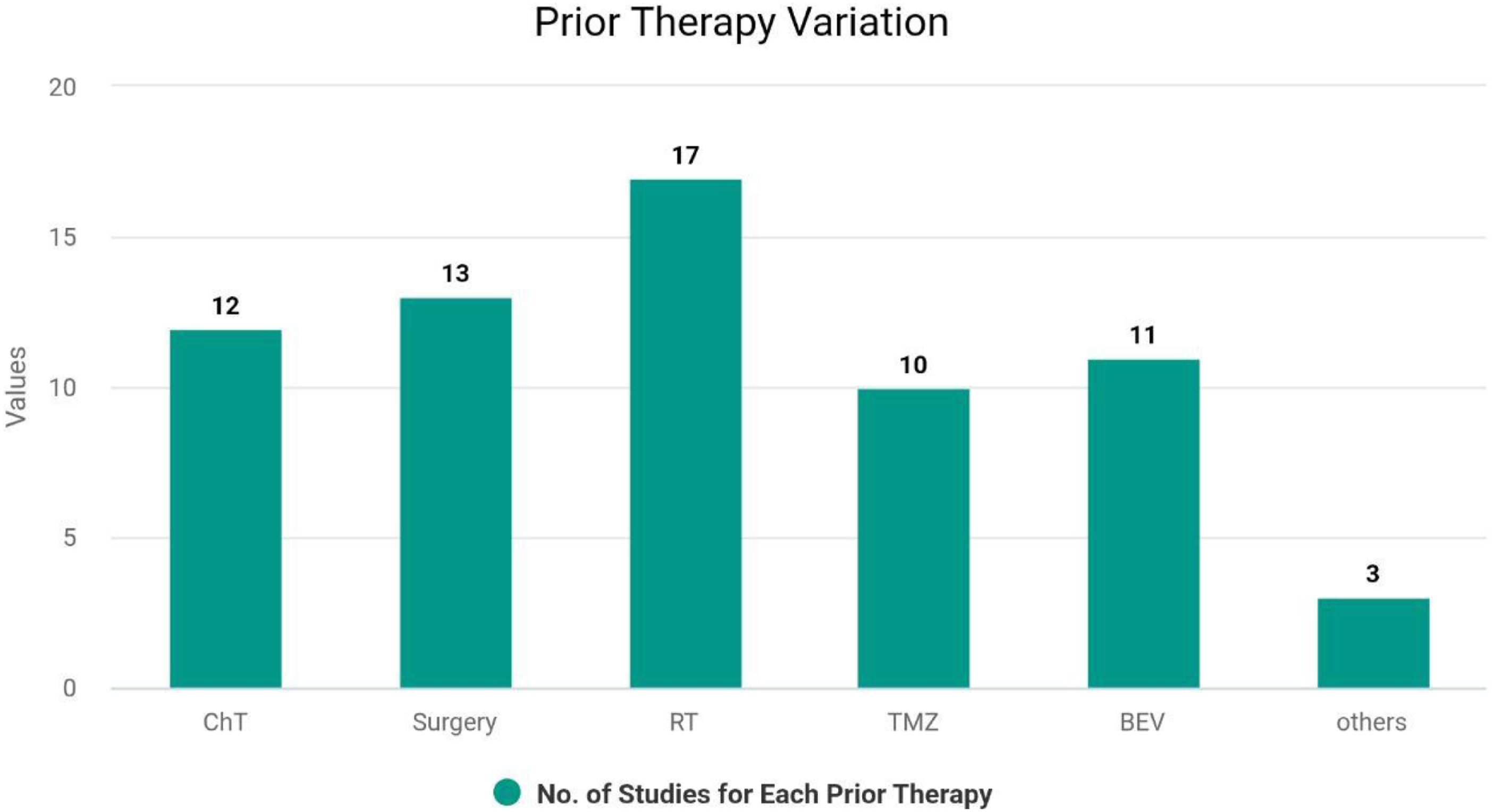
2.8 Reporting Bias Assessment
Risk of bias due to missing results was assessed by searching https://ClinicalTrials.gov for unpublished trials and comparing registered outcomes with reported outcomes in corresponding publications. We did not construct funnel plots due to the small number of studies per outcome and lack of meta-analysis.
3. Results
The search yielded 975 records. After removing 159 duplicates, 816 records were screened by title/abstract. 700 records were excluded, leaving 116 full-text reports assessed. Of these, 73 were excluded (reports not retrieved or do not meeting the inclusion criteria). Out of 43 included studies, there were 24 published studies and 19 registered studies on https://ClinicalTrials.gov, totalling 462 patients in the virotherapy groups across all 43 studies.20-43 See PRISMA flow diagram (Chart1). We included a summary of the included studies, baseline characteristics, outcomes and adverse event incidents in the
3.1 Summary & Baseline
3.1 1 Included Population
Across included studies the mean age of 45 to 55 years, and an inclusion age of ≥18 years, except for two published studies28,32 and six registered studies, which had a pediatric population target ( age < 18 years). In addition, Freeman et al.,2006 partially included young patients (11-58) and had the lowest mean age (44.5 years) among non-pediatric specific studies.
The main pathology was Grade IV malignant glioma. Moreover, 18 published and 9 registered studies included recurrent glioblastoma, with a total of 190 recurrent cases. The Karnofsky Performance Status (KPS) score for inclusion in both published and registered studies was KPS ≥ 70 in 22 studies (12 published studies),20-24,28,29,34,38,40,41,43 KPS ≥ 60 in 18 studies (11 published studies).25-27,30,31,33,35-37,39,42 One published study had a KPS lower limit of 50 32 along with two registered studies.
3.1 2 Virus Class & Administration
The majority of included studies focused on herpes simplex viruses (HSV-1) (n=10) and adenoviruses (n=7). Other virus classes include reovirus (n=2), Measles (n=1), Poliovirus (n=1), Protoparvovirus (n=2), and NDV (n=1). Most studies employed intratumoral (I.T) administration, while four studies used intravenous (I.V) with NDV, Protoparvovirus, and reovirus.
3.1 3 Prior Therapy
Variation in prior treatment is observed among the included studies as shown in (Chart 2) and
3.1 4 Risk of Bias Assessment
A summary of the risk of bias assessment for the 24 included studies is presented in (Fig1) and detailed in (Supplementary Table 7). Overall 90% of studies were judged as having a high risk of bias because of the randomization process mostly due to insufficient reporting of the randomization concealment process.
3.2 Adverse Effects
The results of adverse effects across the included studies revealed considerable heterogeneity in both the frequency and type of reported toxicities. Headache (n=145), fever (n=78), and fatigue (n=83) were among the most common adverse effects.
In addition, neurological adverse events were among the most prevalent, such as seizures (n=96), which were reported in up to 26 cases in Desjardins 2018, and frequently noted in Freeman 2006 and Farshad Nassiri (2023). Moreover, speech disorders had 59 incidents across the included studies (mostly reported in Desjardins 2018). Otherwise, paresthesia had 22 cases reported (mostly in Desjardins et al., 2018), muscle disorders (including dystonia and muscle weakness) had 36 cases reported, mostly in Farshad Nassiri 2023 & F. Lang 2018. Finally, pyramidal tract syndrome (n=30) was mostly reported in Desjardins 2018.
As for gastrointestinal disorders, there was also a notable frequency of some symptoms like nausea (n=75), vomiting (n=70) and constipation (n=15), mostly noticed in Pérez-Larraya 2022, F. Lang 2018 and Farshad Nassiri 2023. There were also other less frequent but important adverse events: psychiatric disorders (n=84) (notably reported in F. Lang et al., 2018), cognitive disorders (n=51) (especially in Farshad Nassiri 2023), eye disorders (n=46) (mostly in Desjardins 2018 and F. Lang 2018), cerebral edema (n=38) (mostly Farshad Nassiri 2023), urinary tract infection (n=14) and gait disturbance (n=47). The total number of events for each adverse effect reported in all published trials is summarized in Supplementary Table 5 and Chart 3.
To enhance the clinical interpretability of safety outcomes, adverse events were further considered according to severity using the Common Terminology Criteria for Adverse Events (CTCAE). Within the literature evaluated for this analysis, the most commonly reported toxicities were Grades 1–2 toxicities, such as headaches, fever, and fatigue. On the other hand, Grade 3–4 adverse events were relatively rare but important for clinical interpretation, especially neurological toxicities like seizures, brain edema, cognitive impairment, and focal neurological deficits. Although reporting was inconsistent, Grade 3–4 toxicities only made up a smaller fraction of adverse events, which were generally manageable. However, it should be acknowledged that reporting regarding CTCAE grading varied within each study analyzed here; thus, direct comparison is not feasible. Nevertheless, based on the data, it is clear that oncolytic virotherapy presents itself as a fairly safe approach with relatively uncommon severe toxicities that can be managed.
3.3 Progression and Response Outcomes
Generally, we observed a wide variability in Progression-free survival (PFS). Short PFS (≤3 months) was reported in the majority of studies.24,33,34,43 Longer PFS (>6 months) appeared in fewer trials.20,28,40 The longest PFS was reported by Perez-Larraya 2022 (10.7 months). 28 Overall survival (OS) also varied, but was mostly under one year. However, a few trials reported longer survival, ranging from ≤6 months23,33,40 to longer than 12 months in selected cases.28,35,36,42
3.3 1 Response Outcomes
Stable disease was more frequently observed than tumor shrinkage, indicating possible cytostatic rather than cytotoxic effects (e.g., Galanis 2024: >90% stable disease in both cohorts). Nevertheless, in the setting of immunotherapy, stable disease could mean immune-controlled tumor growth or delayed effects or pseudo-progression. 44 Partial response was reported in multiple studies (e.g., Pérez-Larraya 2022, Nassiri 2023), while complete response occurred in only a few isolated cases.20,32,36 While Complete Responses (CRs) were rare, often 1–2 patients per study (e.g., Desjardins 2018: 2 CRs). 20
3.3 2 Mortality and Long-Term Survivors
Regarding safety and long-term survivors, some studies reported promising 1-year or 2-year survival rates (Todo 2022 (1): 1-year SR of 84.2%, Pérez-Larraya 2022: 18-month SR of 50%, Maruyama 2023: 1-year SR of 92.3%). Others, like Ning et al., 2024 and Kicielinski et al., 2014, showed poor long-term survival with all patients dying early due to tumor progression.
3.4. Pediatric Subgroup Results
Although the review focused primarily on adult patients, pediatric data (e.g., Pérez-Larraya et al., 2022 and Friedman et al., 2021) suggest age-dependent differences in both safety and efficacy. Children tolerated oncolytic virotherapy relatively well, with high disease control rates but persistent gastrointestinal symptoms (e.g., 7 nausea, 14 vomiting in Pérez-Larraya et al.,) (Chart 4).
4. Discussion
As the results show wide variation in terms of efficacy and tolerability of oncolytic viruses. Regarding PFS and OS, Jiang et al., also reported in their systematic review on malignant glioma a variation in median OS from 3.25 to 20.2 months after treatments. 45 This wide variability in PFS and OS likely reflects differences in viral platforms, dosing schedules, and tumor burden. Challenges like tumor immune evasion, the blood-brain barrier, tumor heterogeneity, immunosuppressive microenvironment, and therapeutic resistance, may explain the variability in overall survival. Among these, intratumoral heterogeneity is considered the main challenge. Recent studies revealed major intercellular differences in gene expression within a glioblastoma tumor, even in the same patient, highlighting the fundamental complexity of treating the tumor. 46
Since objective tumor shrinkage was uncommon, the frequent observation of stable disease may indicate an immunomodulatory effect of virotherapy, delaying tumor progression rather than inducing regression. Moreover, a recent first-in-human clinical trial revealed persistent T-cell mediated cytotoxicity following a single oncolytic virus treatment among patients with glioblastoma. In addition, the study detected robust T-cell infiltration in the tumor parenchyma. These findings indicate that oncolytic virus therapy not only stabilizes disease but also induces long-lasting T-cell immunity and cytotoxicity acting as an immune-activating and tumor microenvironment remodeling therapeutic approach.9,47
However, when assessing the efficacy of immunotherapy, one must take into account its unique features. Stable disease may actually indicate a beneficial antitumor effect. Moreover, delayed effects and pseudo-progression complicate the efficiency assessment, suggesting that criteria need revision in further studies. Collectively, these findings highlight that the oncolytic virotherapy impact extends beyond direct oncolysis and includes substantial immunomodulatory effects. Emerging evidence supports durable immune activation and long-term responders in a subset of patients.12,15 Moreover, although most patients eventually succumbed to the disease, a minority of long-term survivors across multiple studies suggests a durable benefit in select patients, possibly due to host factors or viral-tumor interactions.
Unlike previous reviews that emphasized efficacy or biological mechanisms, we concentrated on adverse events, providing clinicians with critical insight into safety risks associated with various oncolytic viral vectors. Determining the best-tolerated virus remains challenging due to variations in sample sizes and the small number of studies analysed. Nevertheless, a comparative assessment of the two most frequently investigated viral vectors-Herpes Simplex Virus Type 1 (HSV-1) and adenovirus-is warranted.
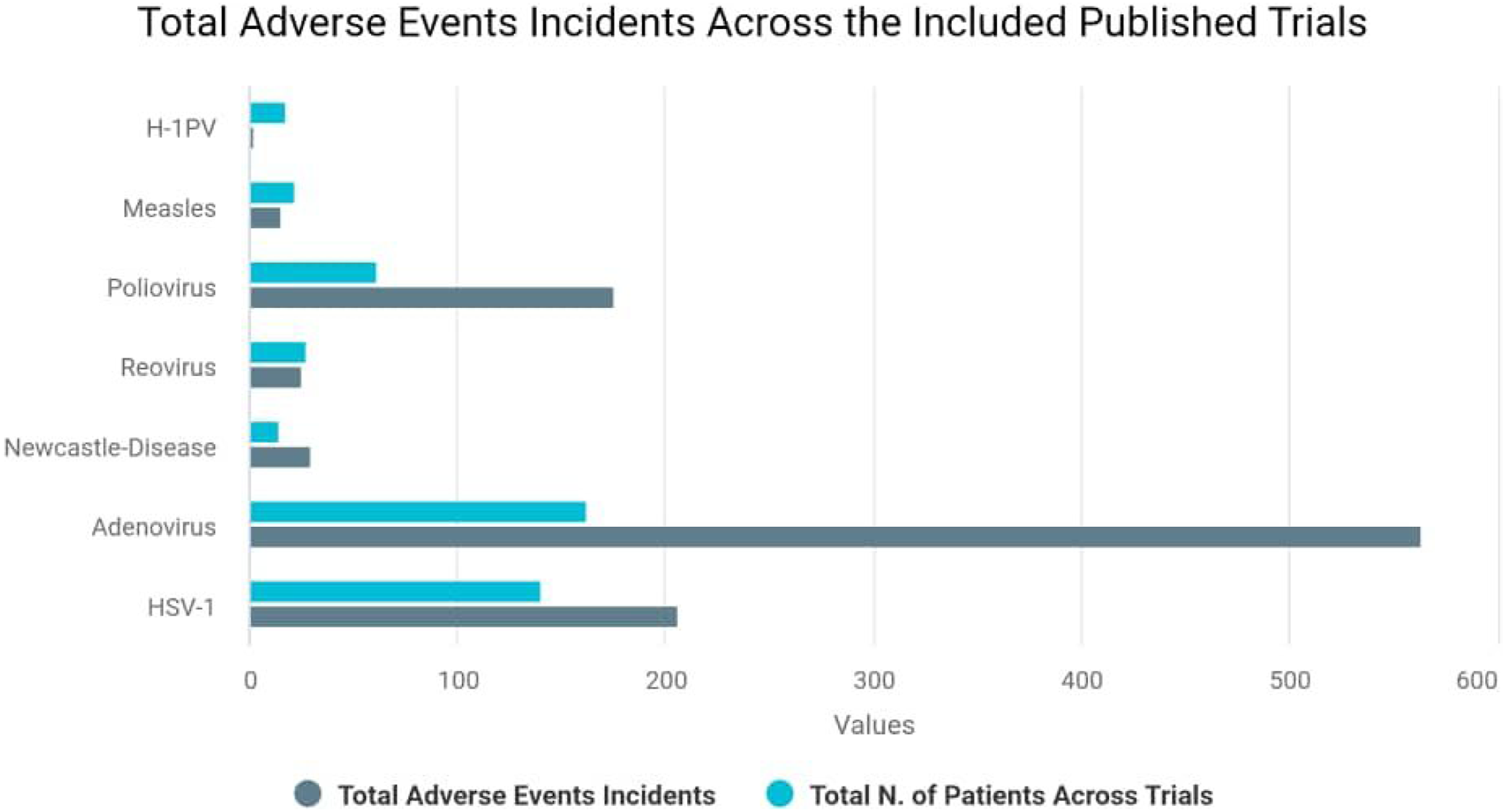
Notably, while the cumulative number of patients treated with adenovirus (n=162) across studies was nearly equaled to HSV-1 (n=140), the incidence of reported adverse effects was comparatively higher in the adenovirus group. Although trials that studied HSV-1 have the second-highest patient enrollment and AE incidence, the relatively proportional AE-to-patient ratio and the neurotropic trait of HSV-1 (which makes it tumor specific) suggest acceptable tolerability.
Conversely, poliovirus trials have a modest sample size but relatively high AE incidence, suggesting a possible overrepresentation of toxicities. Whereas, both reovirus and measles virus trials exhibit low AE incidence and small patient populations, pointing to either high tolerability or underrepresentation in clinical data. Thus, HSV-1 may be more suitable for higher-risk patients due to its favorable safety profile, whereas adenoviruses may be considered for lower-risk patients who are more likely to tolerate adverse events and benefit from their potentially higher efficacy. Chart 5 shows the total number of patients and total adverse events for each virus class across studies.
The route of OV administration represents a critical determinant of both efficacy and safety. In our review, the majority of included trials (22/24 published studies) employed intratumoral (IT) injection, with the remainder using intravenous (IV) delivery (NDV-HUJ, Freeman 2006) or convection-enhanced delivery (CED; Delta24-RGD, van Putten 2022). IT injection provides direct tumour targeting but has limited spatial distribution within the tumour parenchyma, particularly for infiltrative GBM.21,22,31 IV administration offers the advantage of non-invasiveness and potential systemic immune priming, but is severely limited by the blood-brain barrier (BBB) — which restricts passive viral diffusion — as well as by pre-existing neutralising antibody titres and rapid viral clearance. CED bypasses the BBB by delivering virus via pressurised infusion through implanted catheters, enabling wider intraparenchymal distribution.27,31 However, it requires specialised infrastructure and expertise, and carries risks of catheter-related complications, as underscored by recent predictive models for intracranial infection following high-grade glioma surgery. 48 Engineered viral capsid proteins or encapsulation in cell carriers/nanoparticles may partially mitigate the limitations of intravenous delivery – an active area of research. These considerations highlight the importance of optimizing delivery strategies in order to balance therapeutic efficacy with safety.
Fever and fatigue were among the most common adverse effects, and these results are consistent with Ong et al., who recently published a systematic review on oncolytic viral therapy for non-melanoma skin cancer and cutaneous lymphoma that identified 11 published studies involving a total of 20 patients and reported fever or flu-like symptoms as the most common adverse event. 49
In addition, neurological symptoms—especially seizures, speech disorders and cognitive disturbances—emerged prominently in several trials, often with viruses known for CNS tropism, such as HSV-1, 50 which could be associated with direct viral neurotropism or with the central nervous system (CNS)-targeted interventions. However, according to fourteen included studies, seven (50%) reported that patients who did not receive additional treatment (chemotherapy, radiotherapy, or immunotherapy) experienced no adverse effects.21,22,24,25,27,40,41 In contrast, among the remaining seven studies, three (21%) reported that patients who did not receive additional treatment nevertheless developed adverse effects.34,38,42 The other four studies (29%) indicated that patients who received additional treatment also developed adverse effects.20,26,33,39 In a study involving 125 patients with newly diagnosed glioblastoma and MGMT-unmethylated promoter status, participants were divided into two arms: an experimental arm (n = 83), which received veliparib with radiotherapy followed by adjuvant veliparib and temozolomide, and a standard arm (n = 40), which received concurrent temozolomide with radiotherapy followed by adjuvant temozolomide. Reported neurological adverse effects in the experimental arm included headache (69%) and seizures (11%), whereas in the standard arm headache (50%) and seizures (5%) were observed. 51 Another study randomized 80 patients with recurrent glioblastoma to receive either pembrolizumab with bevacizumab (cohort A, n = 50) or pembrolizumab monotherapy (cohort B, n = 30). Neurological adverse effects in cohort A included headache (16%) and seizures (6%), while in cohort B headache (30%) and seizures (7%) were reported. 52 Collectively, these findings highlight the difficulty attributing adverse effects such as seizures or headaches to a specific additional treatment or to potential synergistic interactions among therapies. Overall, the evidence remains inconclusive, and further studies are warranted to clarify these associations. Other less frequent adverse effects like gastrointestinal disorders (e.g., nausea, vomiting and constipation) may be secondary to intracranial effects (increased ICP, oedema) or may reflect systemic immune responses or treatment-related toxicity.
In comparing the AE-to-100 patients ratio for virus groups that were studied by more than one trial, we find the following values: HSV-1: 147%, adenovirus: 348%, and reovirus: 93%. However, we should indicate that across all included trials most adverse effects were grade I or II with some trials reporting some grade IV effects.20,23,31,32,34-36,41 Most of these were neurological effects (e.g., seizures, confusion, speech disorders, hydrocephalus, vision field defect, cerebral herniation, cerebral edema, hemiparesis and meningitis) along with general effects (e.g., headache, fatigue) and bone marrow effects (e.g., neutropenia and lymphopenia). These were all manageable, except for one event that occurred in one patient in Puten et al., 2022 trial who developed diverticulitis leading to sigmoid perforation and sepsis, which resulted in death. Moreover, some studies reported adverse effects that were possibly or likely related to the administered virus, most of which were fever, fatigue, seizures, brain edema, meningitis, speech disorders, and bone marrow dysfunctions (lymphopenia, neutropenia, leukopenia and anemia).21-24,26,29,31-34,36,40-43 However, this was uncommon in most cases, and a direct causal relationship between these effects and the viruses was not confirmed. An important but under-discussed challenge in interpreting OV therapy outcomes is the phenomenon of pseudoprogression, in which virus-induced local inflammation and immune cell infiltration, hence can mimic tumour progression on standard MRI imaging, potentially leading to premature trial discontinuation or misclassification of treatment failure. Among our included studies, Friedman et al. (2021) explicitly reported one case of pseudoprogression in the G207 (HSV-1) cohort. The iRANO (Immunotherapy response assessment in neuro-oncology criteria) analogous to iRECIST criteria used in systemic immunotherapy, were developed to address this challenge by allowing for a confirmatory scan prior to declaring progressive disease.44,53 Future GBM virotherapy trials should adopt iRANO criteria to avoid underestimation of true immunological benefit. Advanced imaging modalities, including MR spectroscopy and amino acid PET, may further improve the discrimination between true progression and pseudoprogression in this context.
Finally, among pediatric-only trials,28,30 Friedman 2021 evaluated the G207 (HSV-1) and reported 21 adverse events with a median OS of 12.2 months. In contrast, Pérez-larraya et al.'s investigation of DNX-2401 (adenovirus) documented a significantly higher number of adverse events (85 events), yet demonstrated an improved median OS of 17.8 months. These findings suggest that while DNX-2401 may have greater toxicity but could offer extended survival benefits in pediatric populations. The observed disparity in adverse events between adenovirus and HSV-1 should be interpreted with caution, as the included trials did not report prior therapies (e.g., bevacizumab), which may represent a confounding factor.
Notably, gastrointestinal toxicity appeared more pronounced in pediatric patients, with vomiting reported in 58% of cases, 28 compared to an average of 15% in adult studies (Supplementary Table 5). Hence, supporting the observation of age-dependent differences and underscoring the need for age-specific monitoring and supportive care strategies in oncolytic virotherapy. Pediatric and adult glioma patients likely differ in both tolerability and immunological responses to oncolytic virotherapy. Children exhibit higher baseline blood-brain barrier permeability and more robust innate immunity, potentially increasing neurotoxicity risk but also accelerating viral clearance – a trade-off that may reduce efficacy.54,55 Adults, in contrast, have a more immunosuppressive tumor microenvironment (e.g., higher Treg and TGF-β levels), which could enhance viral persistence but also limit antitumor immune activation. 56 These age-dependent differences underscore the need for separate dose-finding and immunomonitoring studies in pediatric versus adult trials.
It is important to consider the risks associated with delivery methods of oncolytic viruses, as intratumoral administration is frequently employed in oncolytic virotherapy protocols. Consequently, surgical and procedure-related complications should be included in the overall safety assessment of these therapies. Among these complications, intracranial infection (ICI) which might lead to meningitis and cerebritis represents one of the most serious postoperative complications. A recent study identified low preoperative Karnofsky Performance Status score and prolonged drainage tube placement as important predictors of postoperative ICI. Furthermore, a new accurate nomogram was developed to predict ICI following high-grade gliomas surgery, which can help in identifying high-risk patients who could benefit from personalized prophylactic measures. 48
These findings should be interpreted cautiously, particularly when comparing different viral platforms. Apparent differences in safety or efficacy may simply reflect variations in study design, sample size, or patient selection rather than genuine biological distinctions between viruses. In addition, survival outcomes are influenced by several confounders, including prior treatments and tumor heterogeneity. Therefore, the current evidence does not allow firm conclusions about whether any one oncolytic virus is superior to another.
4.1 Limitations
Several limitations that we encountered while performing this systematic review should be acknowledged. First, the studies included exhibited high heterogeneity in terms of study design, patient groups, virotherapy platforms, outcome definitions, and follow-up periods. This variability makes it hard to directly compare results between studies and limits the findings generalizability. Hence, efficacy and safety findings will have to be reviewed with caution. Second, most studies were early-phase trials with small sample sizes and did not have control groups, which limits the generalizability and strength of the findings. Third, reporting inconsistencies were noted among most trials, and others failed to provide complete data on survival outcomes or objective response rates. In particular, vital outcomes such as progression-free survival (PFS), overall survival (OS), and survival rate (SR) were not uniformly defined or reported, making direct comparison difficult. Therefore, a meta-analysis could not be conducted.
4.2 Implications for Clinical Practice
The observed pattern of stable disease suggests a role for virotherapy as a maintenance or adjunctive strategy, rather than as a curative approach. Safety concerns—especially neurotoxicity—should be a primary consideration in trial design and patient consent. Moreover, this systematic review’s results suggest that combining oncolytic virotherapy with standard treatment (surgery and chemotherapy) contributes to improving the overall survival rate of glioblastoma patients and treatment outcomes. This was also indicated by Xiangxing’s study, which found that combining oncolytic virotherapy with chemotherapy or immune checkpoint inhibitors (ICIs) for solid tumor treatment had better efficacy than combining oncolytic virotherapy with chemotherapy. Moreover, they indicated that oncolytic virotherapy combined with pembrolizumab can enhance safety and efficacy for patients with solid tumors (however, no GB case was included in this study). 57
Combination therapies have a logical basis, as the mechanism of antigen release and spreading induced by OV increases the immunogenicity of the tumour. This may work in combination with immune checkpoint inhibitors to restore T-cell functionality, as well as turning “cold” tumours into “hot” tumours.58,59 Moreover, OV therapy could help increase infiltration of CAR-T cells and avoid immuno-suppression, establishing OV as an immune-modulating platform. In addition, growing evidence supports integrating oncolytic virotherapy with adoptive cell therapies, such as CAR-T cells and T-cell engager cells. Oncolytic viruses may facilitate the entry and infiltration of immune cells within the tumour micro-environment while also regulating certain inhibitory mechanisms preventing proper T-cell activity in solid tumours.60,61 These synergistic mechanisms position oncolytic virotherapy as both a direct cytotoxic modality and a potent immune-modulating platform that enhances other immunotherapeutic strategies.
4.3 Recommendations for Future Research
Future research on oncolytic virotherapy (OV) requires further refinement and systematic development to optimize both efficacy and safety. One important direction is the enhancement of OV monotherapy efficacy through strategies that promote viral replication within tumor cells, strengthen direct oncolytic effects, and elicit more robust antitumor immune responses, while carefully balancing antitumor and antiviral immunity.62,63 Another promising avenue involves improving systemic delivery, such as engineering viral capsid proteins to reduce immunogenicity and evade preexisting neutralizing antibodies, and employing innovative delivery platforms, including cell carriers or nanoparticles, to overcome complement activation, immune clearance, and potential hepatotoxicity.46,64 In parallel, recent studies in melanoma have identified preliminary biomarkers that may predict treatment response.62,64 However, immunotherapy faces considerable challenges in solid tumors of the central nervous system (CNS), including gliomas, due to the blood-brain barrier, tumor heterogeneity, immunosuppressive microenvironments, immune evasion, and therapeutic resistance. These factors likely contribute to the observed variability in OV efficacy among patients. Emerging evidence suggests that distinct CNS compartments exert diverse immunological functions that influence both local and systemic immunity, further complicating treatment outcomes. Future studies incorporating genomic and immune profiling are needed to identify predictive biomarkers, optimize patient selection, and guide personalized OV-based immunotherapy strategies in CNS malignancies. 46
Conducting randomized controlled trials (RCTs) comparing oncolytic virotherapy to standard salvage regimens is urgently needed. In addition, combination strategies, including immune checkpoint inhibitors or CAR-T cells, could synergize with oncolytic virus-mediated immunogenicity and minimize adverse effects. Additionally, oncolytic viruses can serve as a foundation for developing new immunotherapeutic approaches, particularly when employing CAR-T cells and bi-specific T-cell engagers. 3 Moreover, given that many tumor cells exhibit altered metabolic pathways, investigating how oncolytic viruses can exploit or modulate this metabolic phenotype could unveil novel strategies for selective tumor targeting. Elucidating the molecular mechanisms through which viral replication interacts with tumor metabolism may not only improve oncolytic virus design but also open avenues for synergistic combination therapies involving metabolic inhibitors. 65 Finally, more studies are required on new techniques that may help oncolytic viruses to increase their impact and improve overall patient survival, including nanoparticles in newly diagnosed patients, screening OVs in 3D-organoids resembling the patients’ tumors, and using multi-omics analysis to better understand the GB microenvironment.3,66
5. Conclusion
This systematic review highlights the emerging potential of oncolytic viruses as a novel therapeutic strategy for glioblastoma. This systematic review highlights the emerging, though still investigational, potential of oncolytic virus therapy for glioblastoma. While objective radiological responses were infrequent, disease stabilisation was commonly observed across trials, and — in the context of recent mechanistic evidence of persistent T-cell activation and spatial immune reorganisation — may reflect immune-mediated tumour control rather than purely cytostatic activity. A subset of patients achieved durable long-term survival, suggesting that certain host or tumour factors may predict benefit from OV therapy. Regarding safety, oncolytic virus therapies were generally well tolerated, with most adverse events being Grade 1–2 (mild to moderate). Serious treatment-related complications were rare. These findings support the continued and expanded investigation of OV therapy in clinical trials. However, the current evidence base does not yet support the use of OV therapy as a standard-of-care intervention for GBM. Large-scale, randomised, Phase III trials with standardised endpoints, validated immune response criteria (iRANO), and prospective biomarker analyses are urgently needed to confirm long-term survival benefits and to identify patient subgroups most likely to benefit. The integration of OV therapy within multimodal treatment strategies, including immune checkpoint inhibitors, CAR-T cells, and novel delivery platforms, represents the most promising direction for future research, offering cautious optimism for this challenging disease.
Supplemental Material
Supplemental Material - Advances and Future Expectations in Oncolytic Virus Therapy for Glioblastoma: A Systematic Review of Clinical Trials
Supplemental Material for Advances and Future Expectations in Oncolytic Virus Therapy for Glioblastoma: A Systematic Review of Clinical Trials by Nour Kenaan, MD, George Bashour, MD, Nina Kheyrbek, MD, Saddik Haddad, MD, Moustafa Sardini, MD, Moaz Sabbagh, MD, Zein Alabdin Hannouneh, MD, George Ansstas, MD/MSc, Zuheir Alshehabi, MD/PhD in Clinical Medicine Insights: Oncology
Footnotes
Ethical Considerations
Not applicable (this study did not involve patients or human tissue/samples).
Authors’ Contributions
NK conceived the study, designed the review methodology, led the development of the research protocol, and was the primary writer of the manuscript. All authors contributed to literature screening, data extraction, and original draft writing. GB assisted in interpretation of results and drafting of specific sections of the manuscript. GA and ZA provided critical revisions, supervised the overall project, and ensured the scientific accuracy and integrity of the final manuscript. All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available from the corresponding author upon reasonable request. The data extraction forms are provided as Supplementary File. Extracted data and analytic code are available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.