
Abstract
Background
This present study aimed to evaluate the efficacy, safety, and prognostic factors of pembrolizumab in Vietnamese patients with platinum-refractory recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC).
Methods
We performed a multicenter retrospective cohort study of 62 patients with platinum-refractory recurrent or metastatic HNSCC who received pembrolizumab monotherapy (200 mg every 3 weeks) from January 2020 to June 2024 at Vietnam National Cancer Hospital – K Hospital and Hanoi Oncology Hospital. The primary endpoint was overall survival (OS); secondary endpoints included progression-free survival (PFS), overall response rate (ORR) per RECIST v1.1, and safety per CTCAE v5.0. Survival was assessed using Kaplan-Meier methods, and prognostic factors were evaluated with multivariable Cox regression.
Results
Among 62 patients (85.5% male, mean age 58.9±9.7 years), the ORR and disease control rate were 25.8% and 51.6%, respectively. Median PFS was 4.3 months (95% confidence interval [CI] 2.9-5.7), and median OS was 7.5 months (95% CI 5.9-9.1). Programmed death-ligand 1 (PD-L1) combined positive score (CPS) ≥20 was associated with improved PFS (hazard ratio [HR] 0.452, 95% CI, 0.245-0.832, P=0.005) and OS (HR 0.373, 95% CI 0.157-0.884, P=0.025). Pembrolizumab monotherapy was well-tolerated with grade 3-4 adverse events in 3.2% of patients and lack of treatment-related deaths.
Conclusions
This real-world study confirms that pembrolizumab monotherapy provides clinically meaningful efficacy and favorable safety in later-line Vietnamese R/M HNSCC patients, with enhanced benefit in PD-L1 CPS≥20, supporting its role in resource-limited settings.
Introduction
Head and neck squamous cell carcinoma (HNSCC) is a global health burden with over 890,000 new cases and 450,000 deaths annually and a reported 30% increase in incidence in recent decades. 1 In developing countries, particularly in Southeast Asia and Vietnam, HNSCC ranks among the most common cancer types, driven by risk factors such as tobacco use, alcohol consumption and betel nut chewing.2,3 Compared with Western populations, HNSCC in developing countries often presents at younger ages, with distinct disease sites, etiologies, such as lower prevalence of HPV-driven cancers and molecular profiles. 4 Challenges such as poverty, limited healthcare access, advanced-stage presentation and inadequate treatment infrastructure further complicate management in low- and middle-income countries such as Vietnam. 5
Recurrent or metastatic (R/M) HNSCC exhibits a poor prognosis, with a median overall survival (OS) of <12 months, even with the EXTREME regimen (platinum-based chemotherapy plus cetuximab). 6 For over 10 years from 2008, the outcome of R/M HNSCC patients did not improve until the immunotherapy era, when immune checkpoint inhibitors were developed. Pembrolizumab, an immune checkpoint inhibitor targeting programmed death-1 (PD-1), 7 demonstrated significantly improved OS compared with chemotherapy in patients with platinum-refractory R/MHNSCC in the KEYNOTE-040, 8 KEYNOTE-012 9 and KEYNOTE-055 10 trials. These studies established the ability of pembrolizumab to provide durable responses and extend survival in patients with R/M HNSCC. Based on these data, pembrolizumab monotherapy was approved in Vietnam in 2018 for the second or later-line treatment of R/M HNSCC. However, these trials predominantly enrolled Western populations, with limited representation from Southeast Asia. Although certain studies from the Asian region have been reported, they typically involved small cohorts or focused on first-line treatment.11-14 Consequently, the real-world benefits of pembrolizumab in Vietnamese patients with R/M HNSCC following platinum-based chemotherapy failure remain unclear.
The present study aimed to present a multicenter retrospective study on Vietnamese patients with R/M HNSCC who received pembrolizumab as a second or later-line therapy. The effectiveness, safety and predictive biomarkers were assessed to confirm the real-world outcome in this population.
Materials and Methods
Study Design
The present retrospective, multicenter cohort study included 62 patients with pathologically confirmed R/M HNSCC treated with pembrolizumab monotherapy in the second or later-line setting from January 2020 to June 2024. This study followed the STROBE reporting guidelines. 15 The data were collected from electronic medical records at Vietnam National Cancer Hospital – K Hospital and Hanoi Oncology Hospital. The primary endpoint was OS; secondary endpoints included progression-free survival (PFS), overall response rate (ORR) per RECIST v1.1 and safety per CTCAE v5.0. The protocol was reviewed and approved by the Hanoi Medical University Institutional Review Board (approval no. 1522/GCN-HMUIRB on 14th June 2024) with a waiver of informed consent due to the retrospective design. An interim safety analysis of this same cohort was previously reported in the Vietnamese Medical Journal (2025 Special Issue) as a preliminary national conference presentation. The present manuscript reports the final mature efficacy and prognostic analyses with extended follow-up.
Patients
Eligible patients were aged ≥18 years with pathologically confirmed R/MHNSCC affecting the oral cavity, oropharynx, hypopharynx, larynx or sinonasal cavities. Patients had progressed following at least one line of palliative platinum-based chemotherapy and received pembrolizumab monotherapy (200 mg every 3 weeks); they underwent at least one computed tomography (CT) scan for response assessment. Medical records were retrospectively reviewed for baseline characteristics [age, sex, smoking history (ever/never), Eastern Cooperative Oncology Group (ECOG) performance status (0-1 vs. 2), tumor location, disease status (locoregional only, locoregional + distant, distant only), human papillomavirus (HPV) status (if available), programmed death-ligand 1 (PD-L1) combined positive score (CPS, retested if necessary), prior systemic therapies (platinum-based, cetuximab)], treatment details (number of pembrolizumab cycles, treatment duration) and outcome data [tumor response, survival, adverse events (AEs)]. Patients previously treated with immunotherapy (either as monotherapy or in combination with chemotherapy) were excluded.
A total of 62 Vietnamese patients with platinum-refractory R/M HNSCC receiving pembrolizumab as second or later-line therapy were included. PD-L1 CPS was assessed using immunohistochemical (IHC) analysis with the Dako 22C3 antibody on VENTANA BenchMark ULTRA platform. Archival FFPE specimens were retrieved and tested/re-tested when not available in the records. CPS was calculated as the percentage of PD-L1-positive cells (tumor cells, lymphocytes, and macrophages) relative to the total viable tumor cells and categorized as CPS <1, 1-19, or ≥20. HPV status was determined by p16 IHC using the CINtec® p16 Histology assay (Roche Diagnostics, Tucson, AZ, USA; cat. no. 07027992001, clone E6H4TM), with positivity defined as strong, diffuse block-positive nuclear and cytoplasmic staining in ≥70% of viable tumor cells. All slides were evaluated by two experienced pathologists, with discrepancies resolved by consensus.
Treatment response was assessed using CT or magnetic resonance imaging based on RECIST v1.1 (2009). The ORR was defined as the percentage of patients achieving complete response (CR) or partial response (PR). Adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE v5.0).
Treatment Regimens
Patients received intravenous pembrolizumab monotherapy (200 mg) every 3 weeks until disease progression, intolerable toxicity,patient decision, or up to 35 cycles.
Statistical Analysis
Descriptive statistics were used for patient characteristics. Continuous variables were reported as medians (range); categorical variables [including ORR and disease control rate (DCR)] were presented as frequencies and percentages. The Chi-squared test was used to examine correlations between variables. PFS was defined as the time from initiation of pembrolizumab to documented disease progression or death from any cause, whichever occurred first. OS was defined as the time from initiation of pembrolizumab to death from any cause. OS and PFS were estimated using the Kaplan-Meier method, with subgroup comparisons using the Wilcoxon log-rank test, such as PD-L1 CPS <20 vs. ≥20. Multivariate analysis included variables with univariate P-value ≤ 0.1 and/or variables of established clinical importance, regardless of their univariate significance. Statistical analyses were performed using the SPSS software (Version 27.0) and GraphPad Prism version 10.05 (GraphPad; Dotmatics). For all comparisons, a P<0.05 was considered to indicate a significant difference.
The patient selection process is illustrated in Figure 1. Patient screening flow chart. R/M HNSCC, recurrent or metastatic head and neck squamous cell carcinoma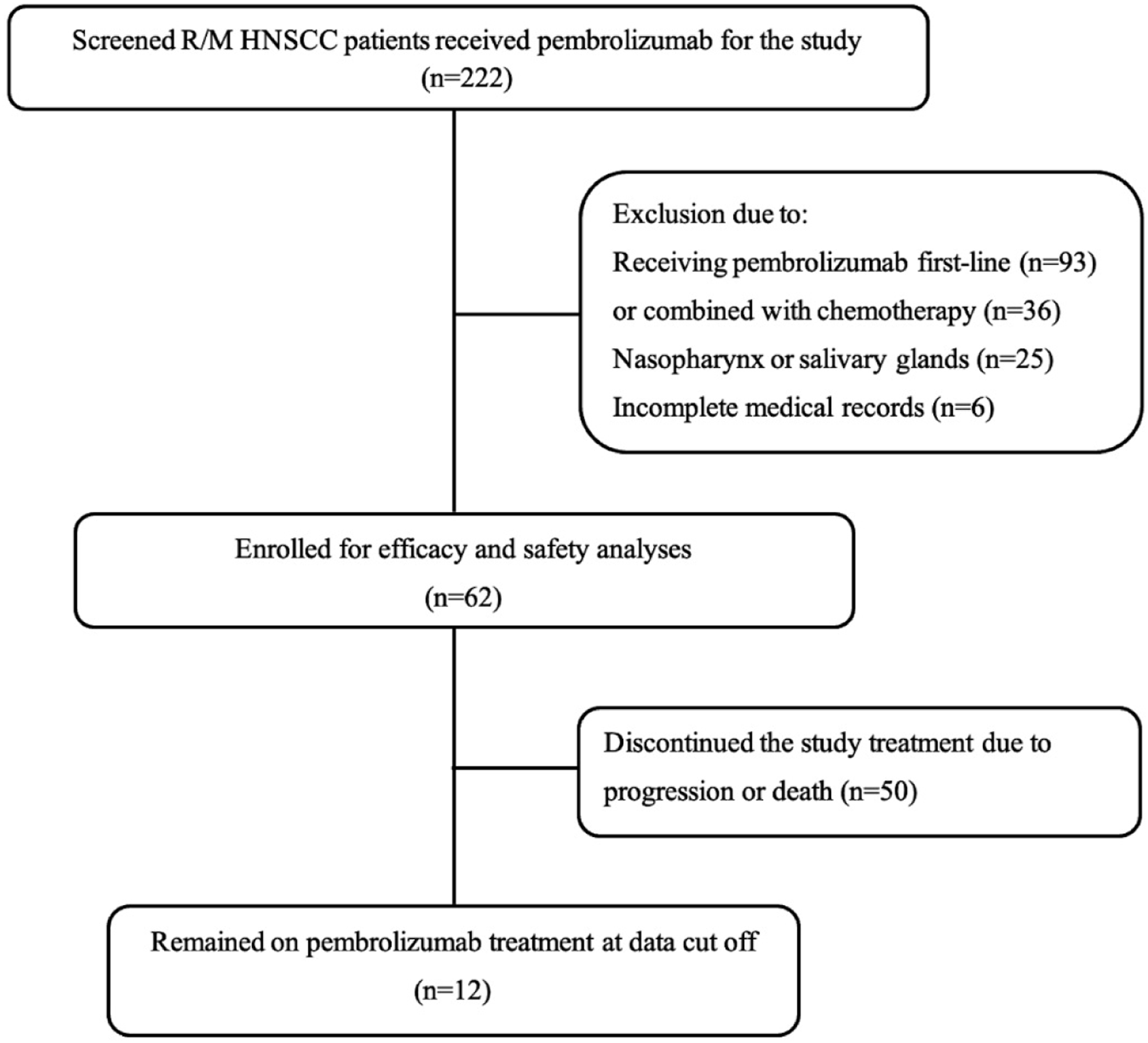
Results
Patient Characteristics and Therapeutic Information
A total of 62 patients with platinum-refractory R/M HNSCC from two Vietnamese centers were evaluated and treated with pembrolizumab monotherapy from January 2020 to June 2024 (Figure 1).
Baseline Characteristics of 62 Patients in the Present Study
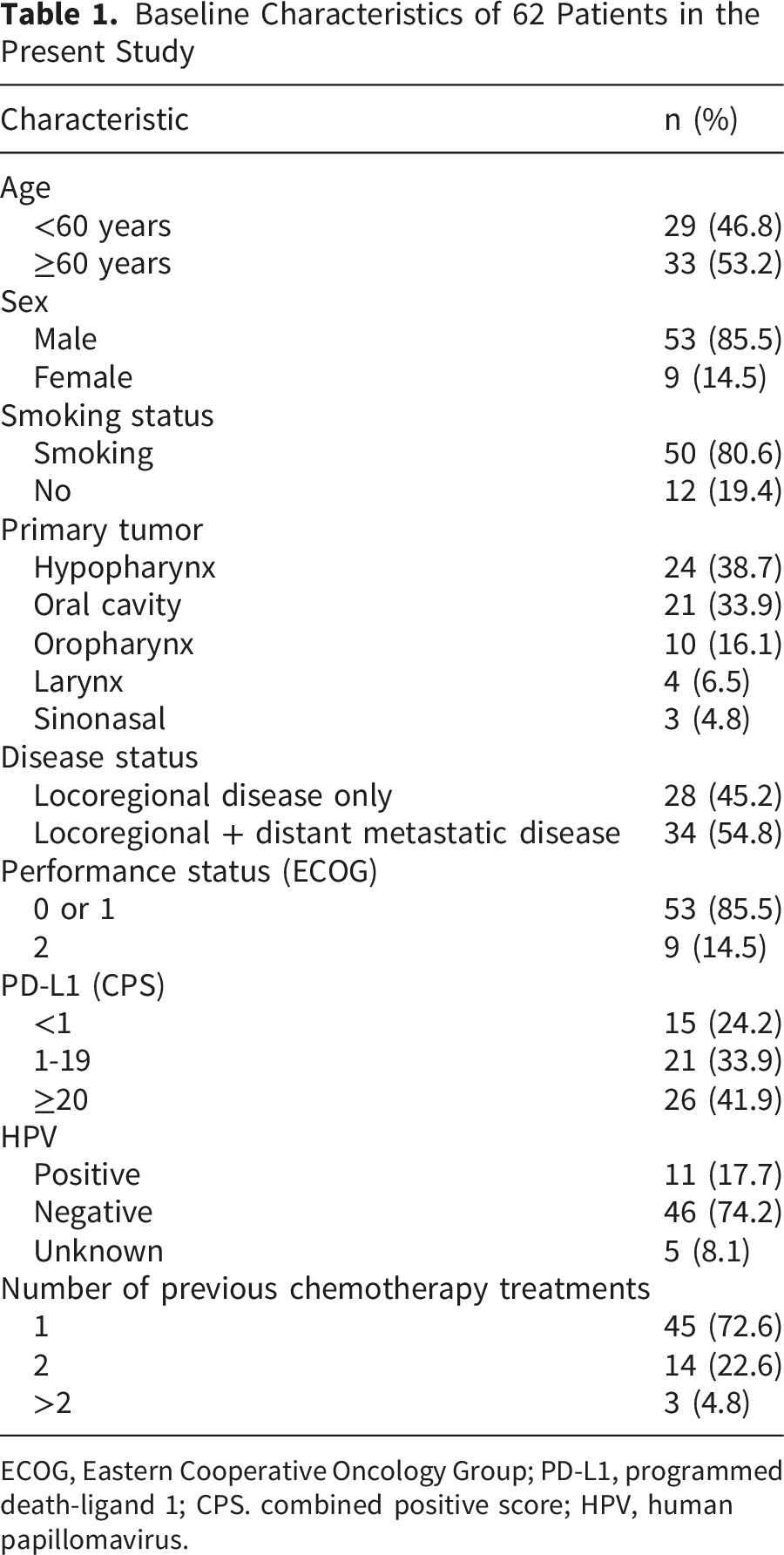
ECOG, Eastern Cooperative Oncology Group; PD-L1, programmed death-ligand 1; CPS. combined positive score; HPV, human papillomavirus.
At initiation of pembrolizumab, 28 patients (45.2 %) had locoregional recurrence only and 34 (54.8 %) had locoregional recurrence with distant metastases. No patient had distant metastases without locoregional progression.
Patients received a median of 6 cycles of pembrolizumab (range 2–35). At data cut-off, 12 patients (19.4%) remained alive and 11 (17.7%) were progression-free, including one patient who completed 35 cycles and achieved a complete response. The median follow-up period was 6.9 months (range 1.6–54.0).
Treatment Outcomes
Treatment Response and Survival Outcomes According to PD-L1 CPS
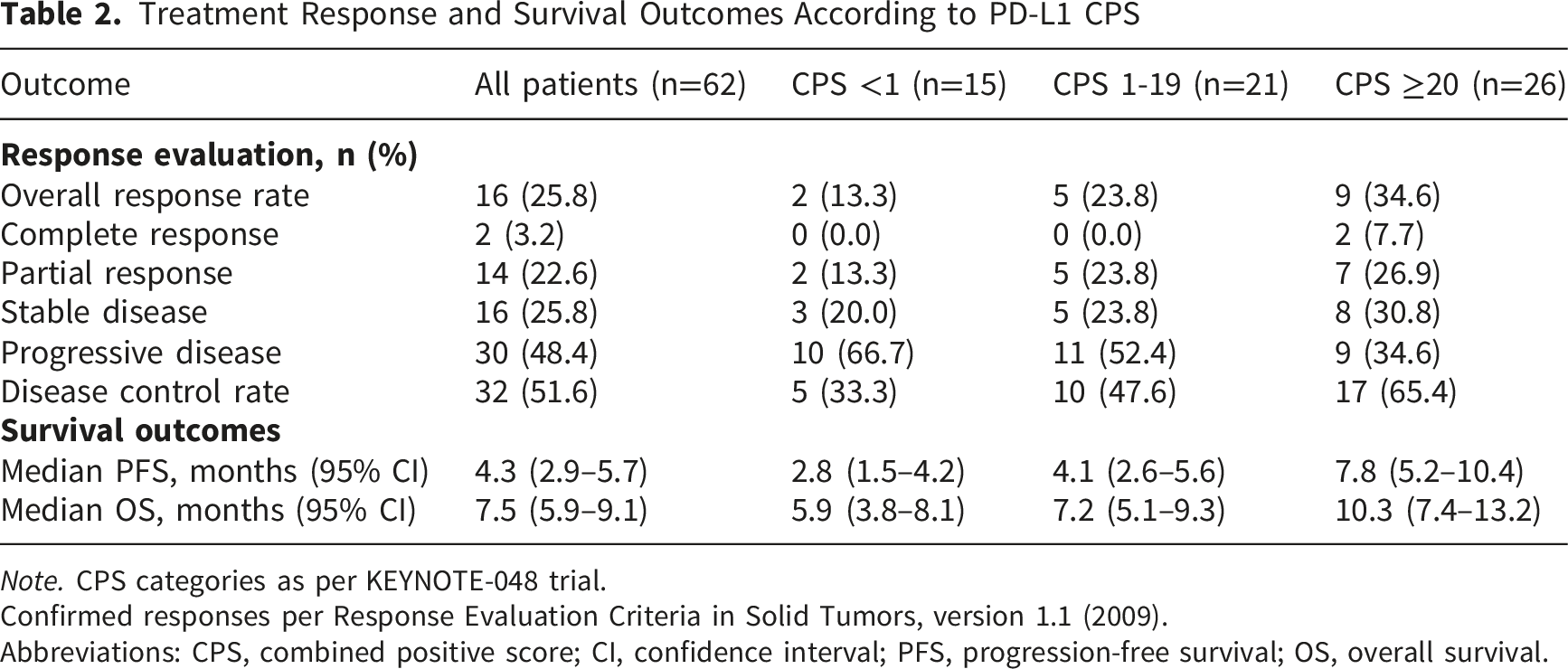
Note. CPS categories as per KEYNOTE-048 trial.
Confirmed responses per Response Evaluation Criteria in Solid Tumors, version 1.1 (2009).
Abbreviations: CPS, combined positive score; CI, confidence interval; PFS, progression-free survival; OS, overall survival.
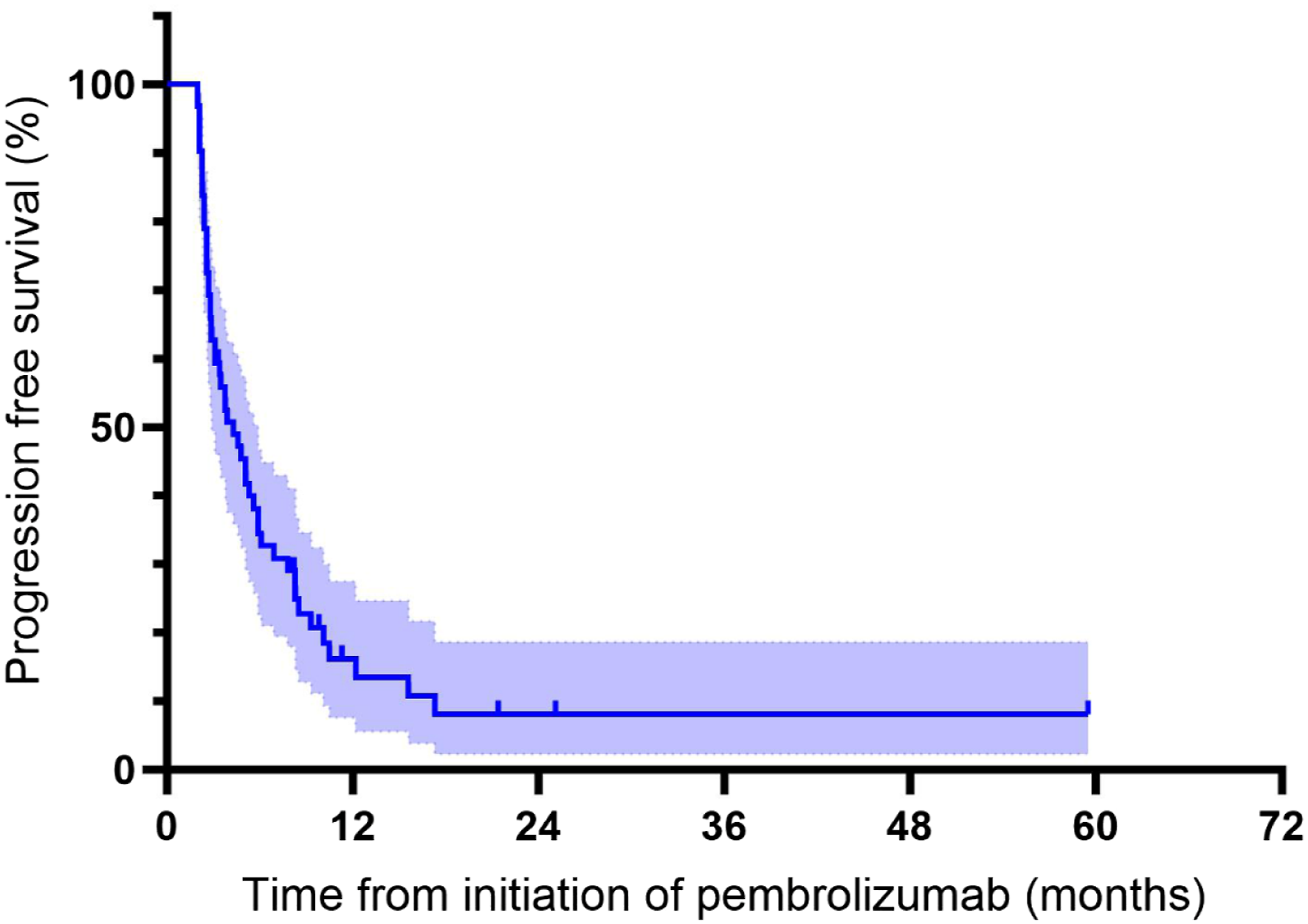
Kaplan-Meier curve for progression-free survival
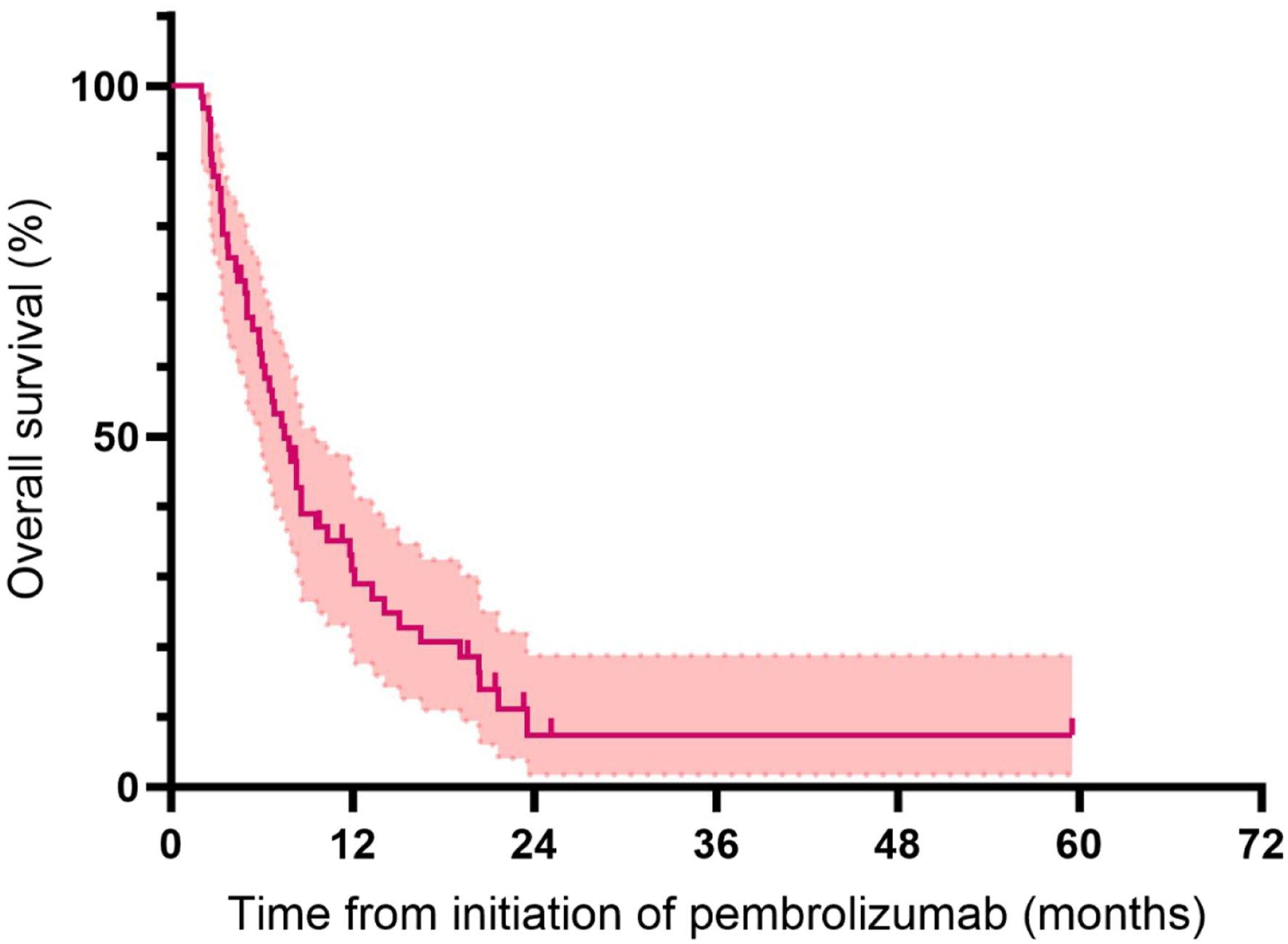
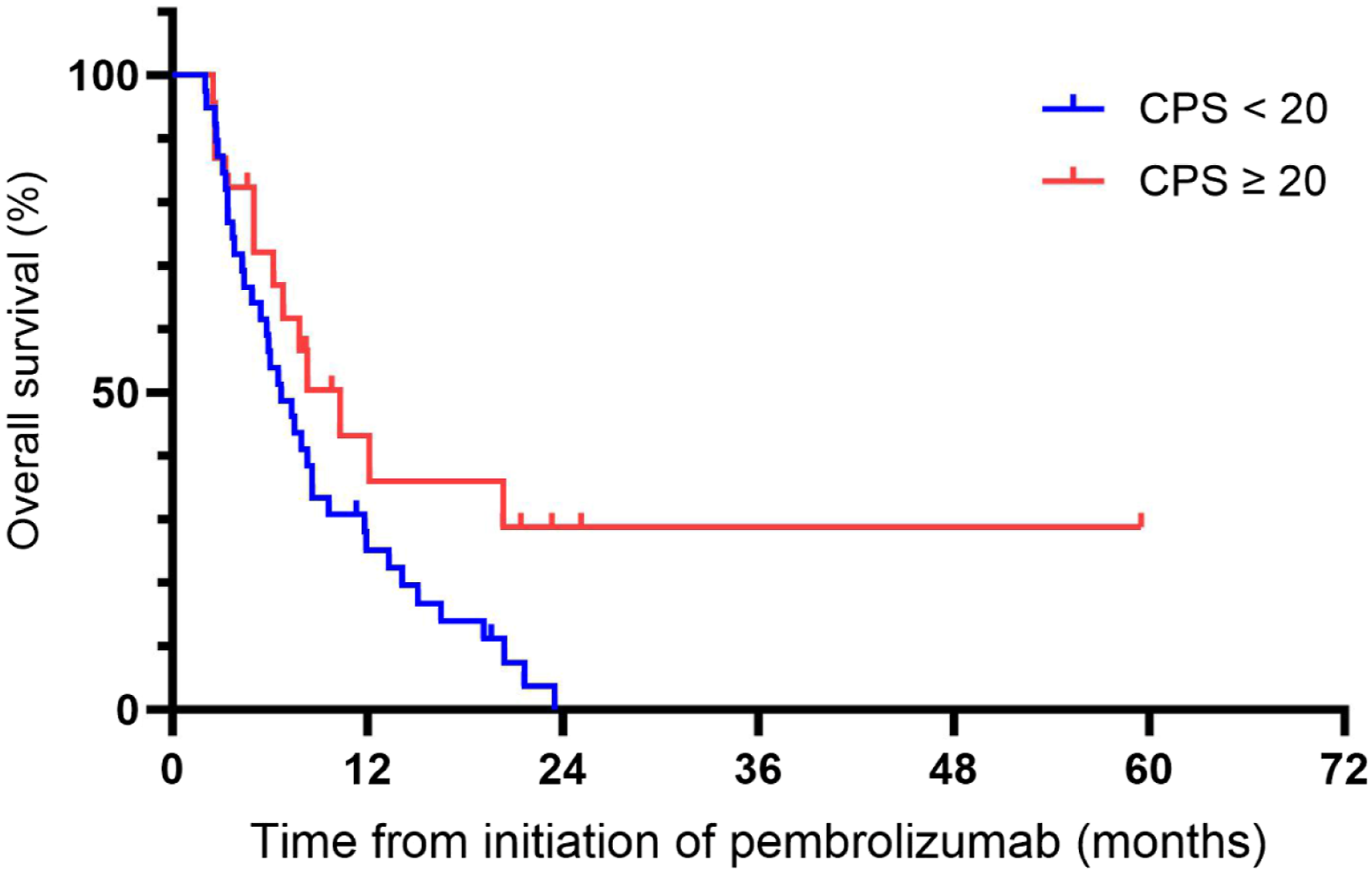
Kaplan-Meier curve for overall survival
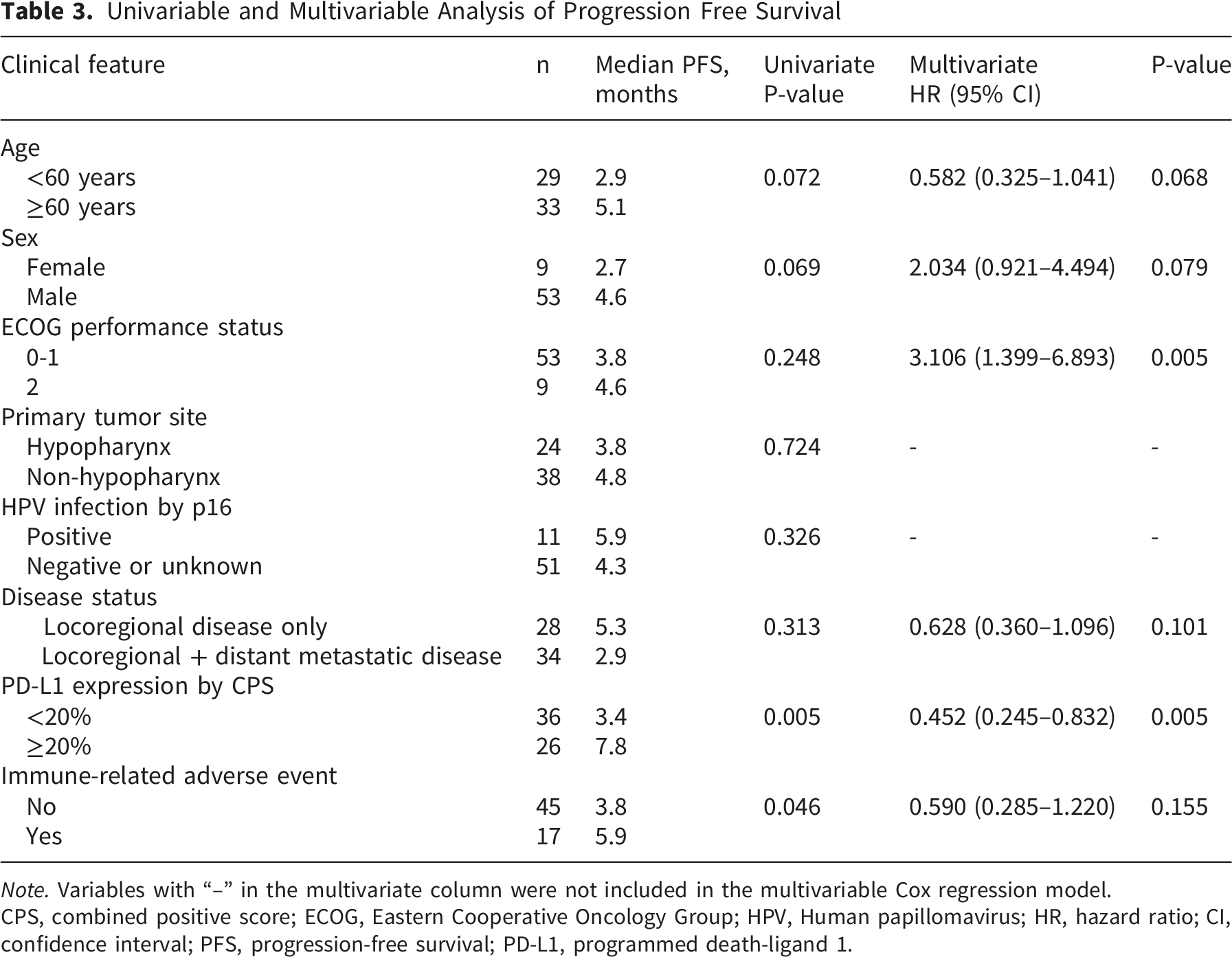
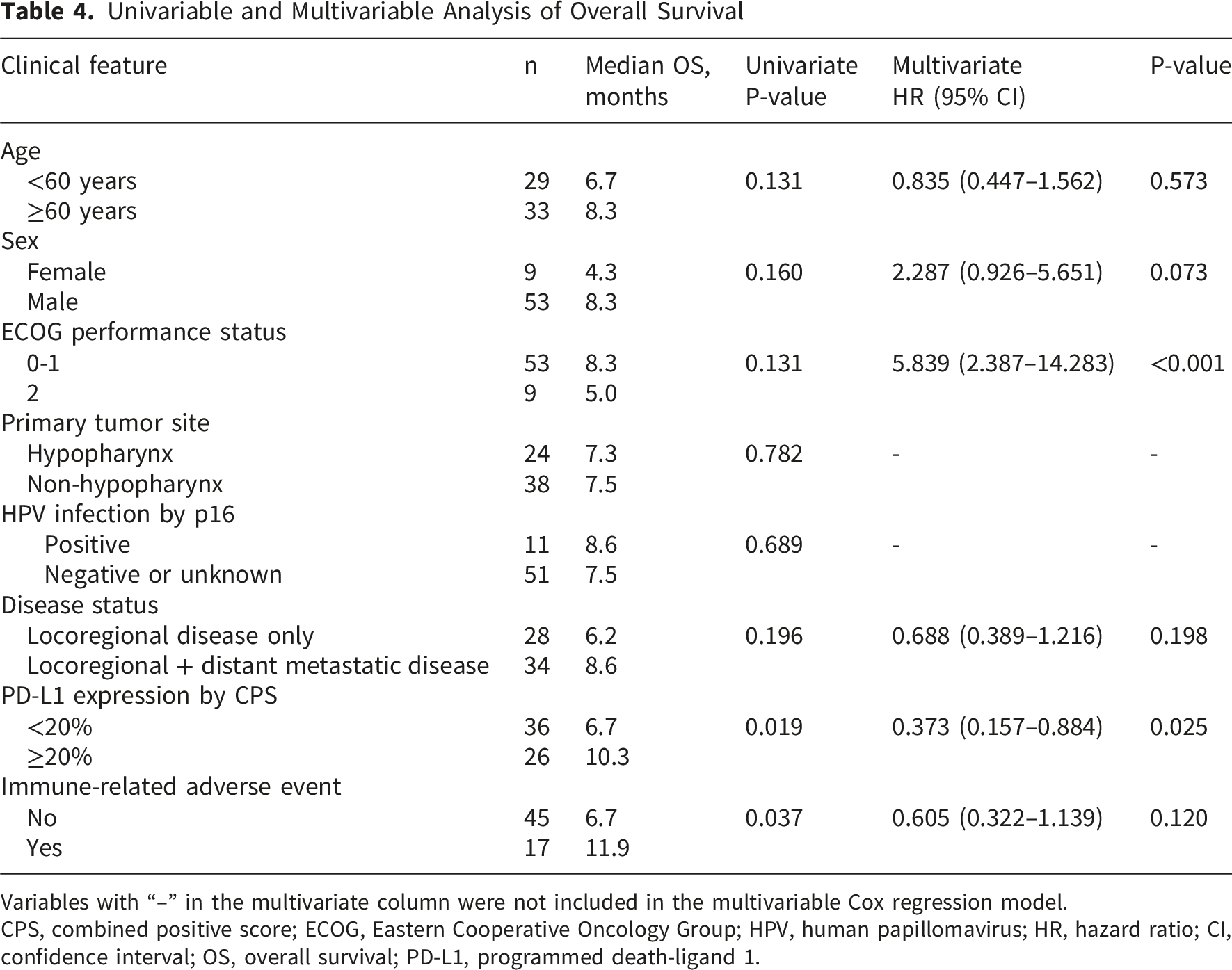
Among the three sinonasal cases, one patient achieved a PR lasting 8.2 months, whereas the other two progressed at first assessment. Subgroup analyses showed numerically higher ORR with increasing PD-L1 expression: 13.3% for CPS <1, 23.8% for CPS 1-19, and 34.6% for CPS ≥20. Median PFS and OS were significantly longer in the CPS ≥20 group (7.8 vs 3.4 months, log-rank P=0.004; 10.3 vs 6.7 months, log-rank P=0.041). Detailed efficacy outcomes by CPS categories are presented in Table 2. Kaplan-Meier curves and multivariate Cox regression analysis demonstrated that patients with high PD-L1 expression (CPS≥20) exhibited significantly improved PFS (Figure 4) and OS (Figure 5) compared with those with CPS<20 (Table 3, HR for PFS: 0.452, 95% CI, 0.245-0.832, P=0.005; Table 4, HR for OS: 0.373, 95% CI, 0.157-0.884, P=0.025). Note that ECOG performance status reached statistical significance in the multivariable model despite non-significant univariate associations; given the small number of patients with ECOG 2 (n=9), this finding should be interpreted with caution. Kaplan-Meier curves for PFS according to PD-L1 expression categories by CPS. CPS, combined positive score; PFS, progression-free survival Kaplan-Meier curves for OS according to PD-L1 expression categories by CPS. CPS, combined positive score; OS, overall survival Univariable and Multivariable Analysis of Progression Free Survival Note. Variables with “–” in the multivariate column were not included in the multivariable Cox regression model. CPS, combined positive score; ECOG, Eastern Cooperative Oncology Group; HPV, Human papillomavirus; HR, hazard ratio; CI, confidence interval; PFS, progression-free survival; PD-L1, programmed death-ligand 1. Univariable and Multivariable Analysis of Overall Survival Variables with “–” in the multivariate column were not included in the multivariable Cox regression model. CPS, combined positive score; ECOG, Eastern Cooperative Oncology Group; HPV, human papillomavirus; HR, hazard ratio; CI, confidence interval; OS, overall survival; PD-L1, programmed death-ligand 1.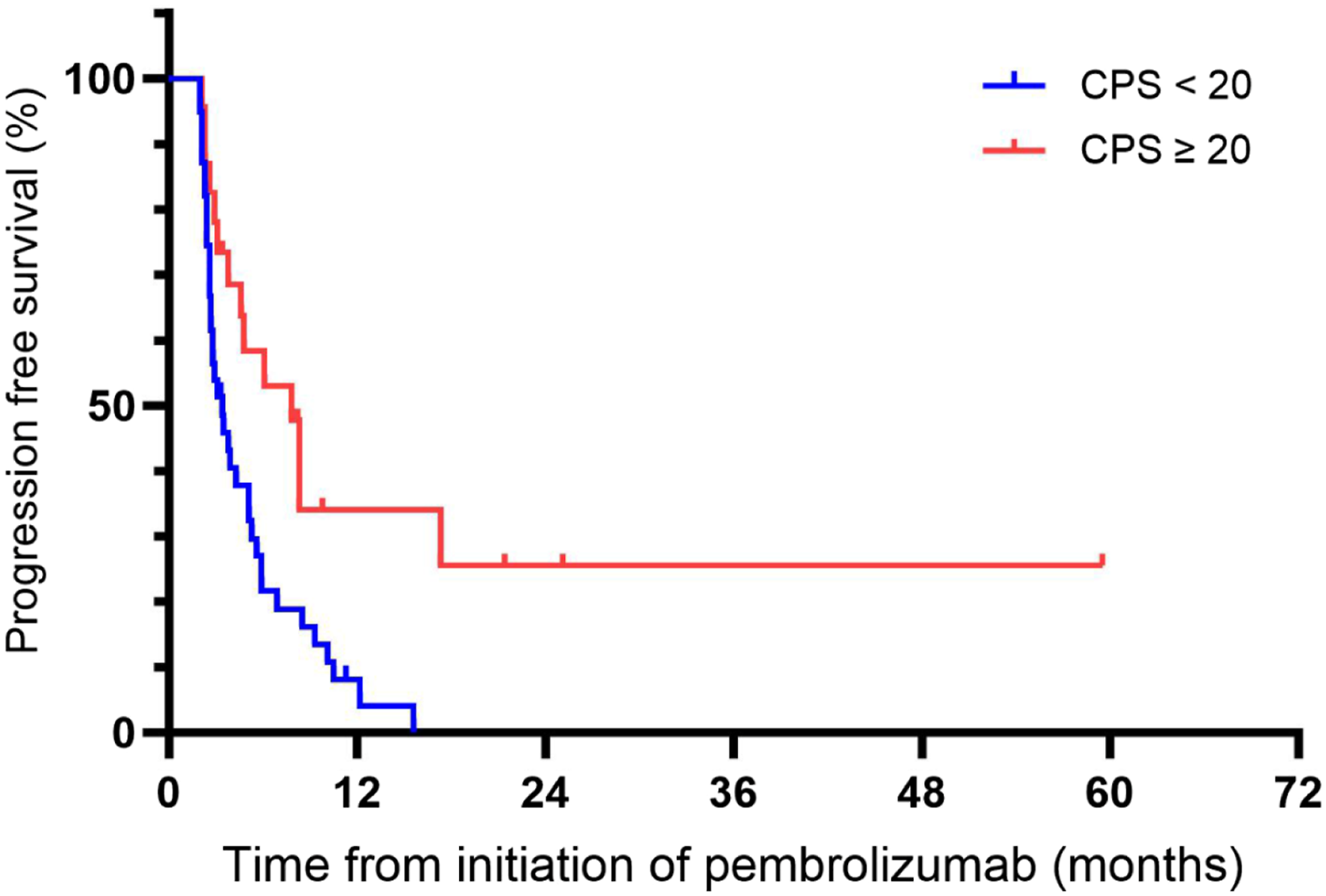
Subgroup analyses revealed numerically better outcomes in HPV-positive versus HPV-negative/unknown patients (ORR 36.4 % vs 23.5 %, median PFS 5.9 vs 4.3 months, median OS 8.6 vs 7.5 months; Supplemental Table S1), although none of these differences reached statistical significance. Similarly, patients receiving pembrolizumab as second-line therapy showed numerically superior efficacy compared with those treated in the ≥third-line setting (ORR 28.9 % vs 17.6 %, DCR 55.6 % vs 41.2 %, median PFS 4.7 vs 3.2 months, median OS 8.1 vs 6.3 months; Supplemental Table S2), with consistent trends in the CPS ≥1 subgroup (ORR 34.3 % vs 16.7 %, median PFS 5.4 vs 3.8 months).
Adverse events in 62 Vietnamese patients With recurrent or metastatic head and neck squamous cell carcinoma treated With pembrolizumab
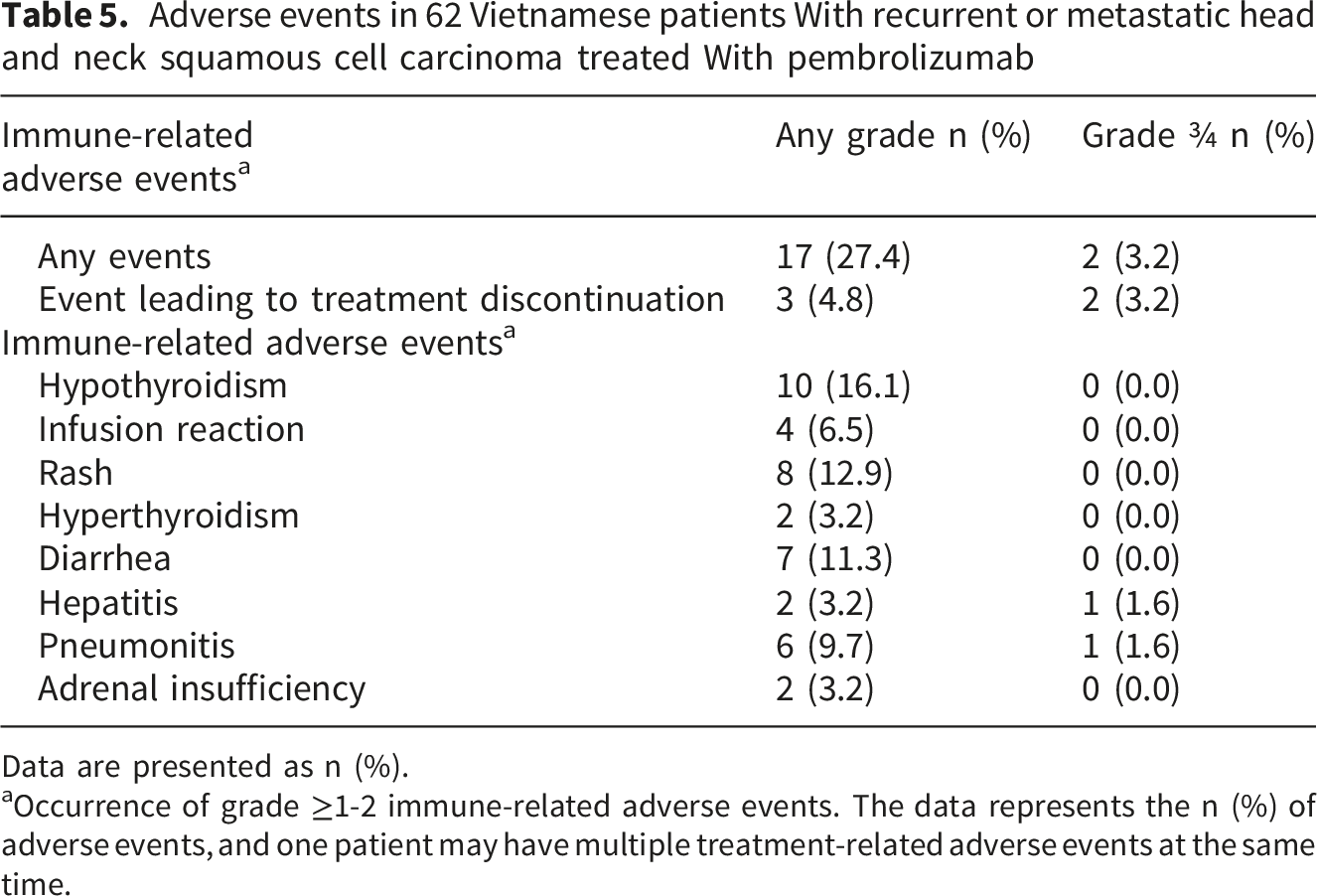
Data are presented as n (%).
aOccurrence of grade ≥1-2 immune-related adverse events. The data represents the n (%) of adverse events, and one patient may have multiple treatment-related adverse events at the same time.
Discussion
The present study provides the first multicenter real-world evidence (RWE) of pembrolizumab monotherapy in second- or later-line platinum-refractory R/M HNSCC among Vietnamese patients. The observed ORR of 25.8% and DCR of 51.6%, median PFS of 4.3 months (95% CI, 2.9-5.7) and median OS of 7.5 months (95% CI, 5.9-9.1) are consistent with Asian real-world cohorts. Hsu et al (14) reported an ORR of 31.8% with 2CR and median PFS 4.67 months in 22 Taiwanese patients. 14 Similarly, Fan et al 12 demonstrated an ORR of 20% and a median PFS of 2.58 months among 30 patients treated in second- or third-line settings. The median PFS of 4.3 months in the cohort of the present study was longer than the range of 2.0-2.7 months reported in clinical trials such as KEYNOTE-040 8 and KEYNOTE-012. 16 This disparity is likely attributable to less frequent imaging in routine clinical practice, typically every 10-12 weeks or upon clinical suspicion compared with every 6-8 weeks noted in the trial protocol. Such extended intervals may delay the documentation of radiological progression, thereby prolonging the observed PFS. Since OS was designated as the primary endpoint of the present study, the observed median OS of 7.5 months aligned with that reported in KEYNOTE-040 (7.1 months) and KEYNOTE-055 (8.4 months), reinforcing the consistent clinical benefit of immunotherapy across both controlled trials and routine practice.
Multiple studies have demonstrated that PD-L1 expression, as measured by CPS, predicts outcomes of immunotherapy in R/M HNSCC. In the present study, a CPS threshold of ≥20 was associated with significantly improved PFS and OS compared with CPS<20. The CPS≥20 cutoff, as applied in the KEYNOTE-048 trial, 17 demonstrated the efficacy of immunotherapy both as monotherapy and in combination with chemotherapy in the first-line setting. Although direct comparison with KEYNOTE-048 is limited by differences in treatment line and patient population, the findings suggest clinical relevance of the CPS≥20 threshold even in later-line therapy. In resource-limited settings such as Vietnam, using a CPS cutoff of ≥20 may enable more selective and cost-effective patient selection for immunotherapy. Prospective validation of this threshold is warranted, particularly in multicenter RWD cohorts from Asia and other low- and middle-income countries. The prevalence of PD-L1 CPS ≥20 in our Vietnamese cohort was highly consistent with real-world Asian data, including a large Chinese multicenter study reporting 41.8% in 402 patients with R/M HNSCC. 18 Similar PD-L1 expression rates have also been observed across other Asian cohorts: CPS >20 rates of 43.4% in Japanese R/M HNSCC 19 and 46.1% in Taiwanese patients, 20 together with positivity rates of 80% in Thai patients 21 and 83.6% in Korean locally advanced disease. 22 In addition, the present study addresses a key evidence gap between clinical trials and real-world setting by including R/M HNSCC patients with rare primary lesions in the nasal sinuses. One out of the three cases achieved PR, while two progressed.
The cohort (n=62) of the present study indicated male predominance and mean age of 58.9±9.7 years, which was consistent with regional epidemiology.23,24 In the present study, 17.7% of patients were HPV-positive as determined by IHC analysis of p16, 74.2% were negative and 8.1% had unknown status due to insufficient tumor samples. Although HPV-positive patients indicated numerically higher ORR and higher median PFS and OS compared with those of HPV-negative/HPV unknown status patients, the differences were not statistically significant. The role of the HPV status in second- or third-line pembrolizumab therapy remains controversial. In KEYNOTE-012, HPV-positive patients achieved a higher ORR than HPV-negative patients (32% vs. 14%). 16 Conversely, KEYNOTE-055 demonstrated comparable efficacy with pembrolizumab regardless of HPV status 10 (ORR: 16% in HPV-positive vs. 15% in HPV-negative; no differences in PFS or OS). In the KEYNOTE-040, HPV/p16-positive status trended toward greater benefit with pembrolizumab in platinum-refractory R/M HNSCC; however, the results did not reach statistical significance and were not predictive compared with those derived from PD-L1 expression. 8 Therefore, HPV status should not restrict pembrolizumab use, as both subgroups can result in survival benefits. 25
The safety profile of pembrolizumab in the present study indicates that it is well-tolerated. Notably, no treatment-related deaths were noted and the treatment discontinuation rate due to AEs was only 3.2%, with 27.4% of patients experiencing AEs overall. These results align with prior randomized controlled trials and real-world data. Two patients experienced grade 3-4 AEs: One with grade 3 pneumonitis and one with grade 3 hepatitis, both of whom responded well to intravenous corticosteroid treatment. The common irAEs noted in the present study included hypothyroidism (16.1%), rash (12.9%) and diarrhea (11.3%); these results are consistent with those reported in the KEYNOTE-040 trial, which noted hypothyroidism (15%) and pneumonitis (4%) as frequent irAEs. 8 Compared with real-world data from Asian populations, a Japanese study examined the application of pembrolizumab as a first-line therapy and demonstrated a higher AE rate (50.0%) with 6.7% grade 3 events, likely due to the inclusion of combination chemotherapy. 26 In 2025, a systematic review and meta-analysis of nine retrospective real-world studies reported a 20.5% overall AE rate for pembrolizumab monotherapy, with grade≥3 irAEs noted in 12.5% of patients in one study. 27 Variations in AE rates across these studies likely arise from data collection issues, such as inconsistent or incomplete AE reporting. Nevertheless, these findings, alongside the data of the present study, support pembrolizumab as a safe treatment option for patients with platinum-refractory R/M HNSCC.
This study has several limitations. Firstly, its retrospective design may introduce selection bias, particularly through the exclusion of patients with incomplete medical records or those with poor outcomes who were not included. Secondly, the sample size (n=62) was relatively small, limiting statistical power suggesting that subgroup analyses and HRs should be interpreted with caution due to wide CIs. Nonetheless, the present study represents the largest reported cohort of Vietnamese patients with R/M HNSCC treated with pembrolizumab, notably compared with the limited studies noted in Asian populations. Thirdly, the data were collected from only two major oncology centers in northern Vietnam; although intended to enhance representation, this approach may still contribute to selection bias and reduce generalizability. Fourthly, the observational design lacked a control group. Finally, as data were extracted from routine clinical records by individual clinicians, inconsistencies in documentation may have led to incomplete information or measurement errors, including under-reporting of adverse events.
Conclusion
The present study is the first Vietnamese multicenter RWE study which confirms the efficacy and safety of pembrolizumab in platinum-refractory R/M HNSCC with enhanced benefit observed in patients with high PD-L1 expression with CPS≥20. These data bridge trial and real-world gaps, support biomarker-driven selection and inform regional treatment strategies. Novel combinations and predictive tools are required to further improve outcomes.
Supplemental Material
Supplemental Material - Efficacy of Pembrolizumab as a Second- or Third-Line Therapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: A Multicenter Retrospective Study in Vietnamese Patients
Supplemental Material for Efficacy of Pembrolizumab as a Second- or Third-Line Therapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: A Multicenter Retrospective Study in Vietnamese Patients by Phuong Thi Bich Nguyen, Hau Xuan Nguyen, Gia Hoang Nguyen, Tai Nguyen Van, Kien Do Hung in Clinical Medicine Insights: Oncology.
Footnotes
Ethical Considerations
The study was approved by the Institutional Ethics Review Board of Hanoi Medical University, Vietnam under decision No. 1522/GCN-HMUIRB, dated 14th June 2024, which covered data collection and analysis from both participating hospitals: Vietnam National Cancer Hospital – K Hospital and Hanoi Oncology Hospital. Because of the retrospective nature of the study, the requirement for informed consent was waived. The study was conducted in accordance with the Declaration of Helsinki. All patient data were de-identified.
Author Contributions
Conception and design: Phuong Thi Bich Nguyen, Kien Do Hung. Collection and assembly of data: Phuong Thi Bich Nguyen, Hau Xuan Nguyen, Gia Hoang Nguyen, Tai Nguyen Van, Kien Do Hung. Data analysis and interpretation: Gia Hoang Nguyen, Phuong Thi Bich Nguyen. Manuscript writing (draft and revised): All authors. Final approval of manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The data underlying this study’s findings are included in the article and can be obtained from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.