
Abstract
Background
Severe pediatric malaria with neurological presentation has a spectrum of severity, from frank coma (Cerebral Malaria (CM)) to impaired consciousness and/or complex seizures without coma (malaria with central nervous system signs, CNS-M). Approximately 9-16% of pediatric CM survivors develop post-malaria epilepsy (PME), but rates after CNS-M are understudied.
Objective
Determine PME rates following severe pediatric malaria with neurologic signs, with and without coma (CM and CNS-M).
Design
Prospective cohort study.
Methods
Children 6 months-11 years who presented to a district level hospital in Zambia with CM or CNS-M between Nov 2021-June 2024 were enrolled. Children were excluded for pre-existing epilepsy or alternative explanation for acute neurologic symptoms. Primary outcome was PME at 1 year. Important covariates included coma, age, pre-illness neurodevelopment, acute hospitalization data, acute and follow-up EEG, and 1-year neurodevelopmental outcomes. Acute, 1-, 6-, and 12-month data were collected. EEGs were analyzed with conventional and quantitative methods. PME was determined by standardized screening and physician review using ILAE criteria.
Results
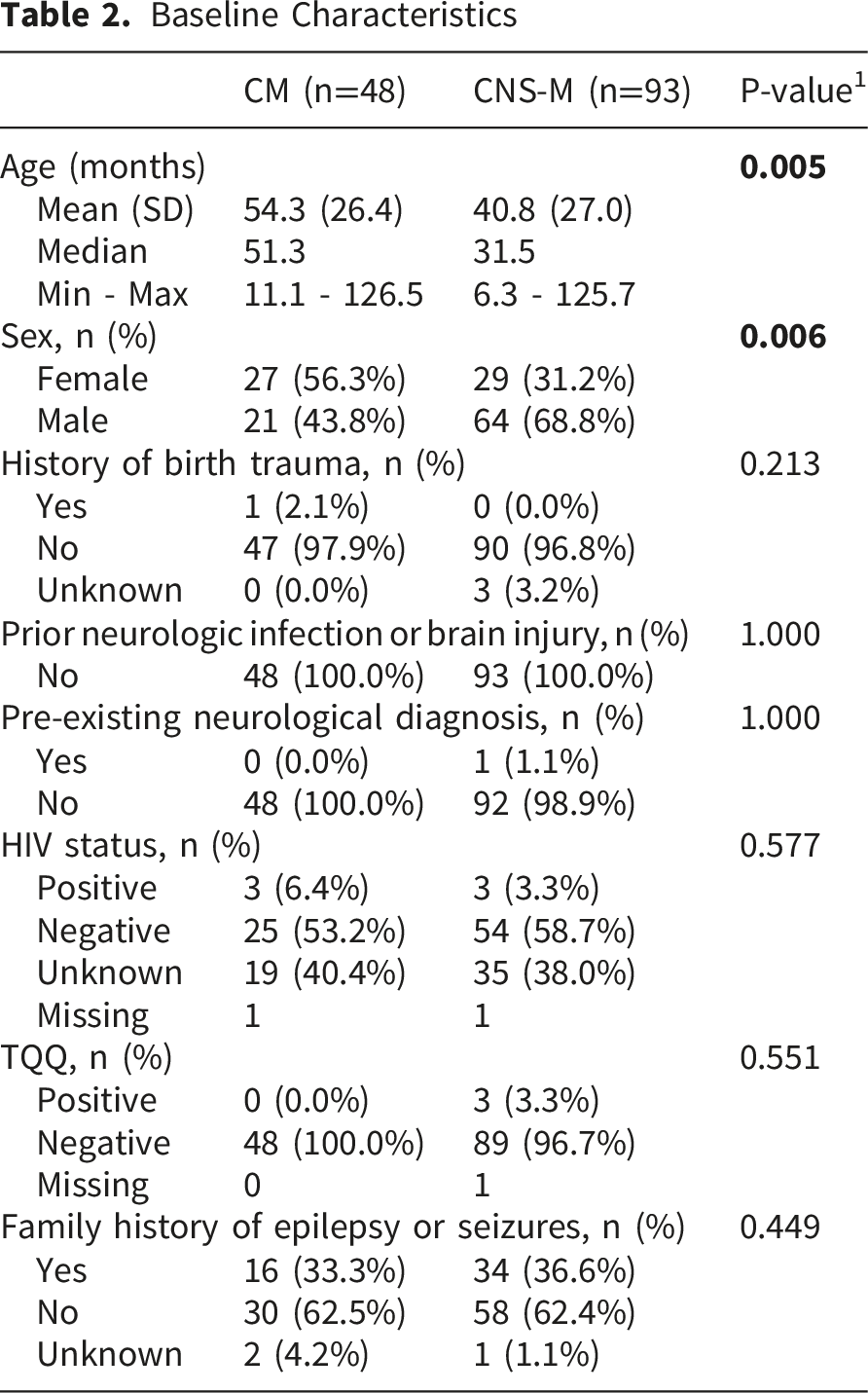
141 children met inclusion criteria, 48 had CM, 93 CNS-M. CNS-M children were younger (mean 40.8 vs. 54.3 months, p=0.005) and male predominant (64.8% vs. 43.8%, p=0.006). 18.4% of the cohort developed PME, with no significant incidence difference between CNS-M (20.4%) and CM (14.6%) groups, p=0.495. Focal epilepsy was more common in CNS-M 78.9% vs. CM 28.6% (p=0.028). There were no differences in qualitative EEG findings. Quantitative EEG measures demonstrated more severe and prolonged cortical dysfunction in CM (p<0.01).
Conclusions
CNS-M presentation was twice as frequent as CM at this district hospital. Quantitative EEG supports CM as a more severe acute illness, but PME developed in 15-20% of children within one year regardless of malarial coma. These findings suggest that severe malaria with neurologic involvement-regardless of coma during acute presentation-has significant secondary epilepsy risk.
Plain Language Summary
Severe malaria in children that is associated with coma has long been known to have a significant risk of subsequent neurologic sequelae, particularly post-malaria epilepsy (PME). However, less well understood is the risk of epilepsy after severe malaria with other neurological signs, such as confusion or complicated seizures. Some small retrospective studies suggested that all malaria with neurologic presentations has some risk, but there are limited systematic data available. We enrolled children presenting with acute malaria and neurologic signs to a rural district hospital in Eastern Zambia and followed them for one-year to assess PME outcomes in the entire group, comparing if the presence of coma impacted epilepsy risk. We found that there were approximately twice the number of children presenting with malaria and neurologic symptoms of complicated seizures or altered awareness
Introduction
Despite decades of eradication efforts, malarial infections continue to occur at high rates globally, with 249 million cases in 2022, an increase of 2 million from 2021. 1 Climate change and emergence of antimalarial drug resistance pose ongoing challenges. 1 Children, pregnant women, and those in rural areas are at highest risk, particularly in Africa, where over 90% of all malaria cases occur. 1 Cerebral malaria (CM), the most severe neurological presentation, affects 500,000 children annually, with 30% of survivors having neurologic sequelae.2-5 Of over 400,000 pediatric CM survivors annually, approximately 9-16%, will develop post-malaria epilepsy (PME),3,4,6,7 equivalent to 36,000-64,000 new pediatric epilepsy cases per year.
Severe malaria with neurologic involvement is often translated as CM; however, severe malaria with impaired consciousness and/or with complex seizures but without coma, i.e., malaria with central nervous system signs (CNS-M), is actually a more common pediatric presentation, with poorly understood pathogenesis,5,8-10 that anecdotally is not always distinguised from CM in routine clinical care. Most research on malaria with neurologic involvement only includes strictly defined CM (Glasgow coma score ≤10 or Blantyre coma score ≤ 2, with malaria parasitemia, and absence of alternative cause for coma 2 ). Thus, the long term outcomes of CNS-M are poorly delineated. One large Kenyan study showed that among all children admitted with severe malaria with neurologic involvement, less than 20% met CM criteria, yet the entire cohort showed higher rates of mortality and neurological deficit on discharge compared to non-neurological malaria. 8 Although limited, case-control studies that include CNS-M also suggest the neurologic sequelae severity and frequency may be similar to CM.5,7,11
To better understand the long-term prognosis of children who present with CNS-M and begin to explore the pathophysiology of CNS-M, we prospectively enrolled children admitted with CM or CNS-M at a rural district level Zambian hospital and followed them for one-year after discharge comparing baseline characteristics, serial EEG findings, and neurologic outcomes.
Methods
Study Design and Participants
Participants were enrolled in the observational prospective cohort study, Predicting epileptogenesis after CNS malaria, at Chipata Central Hospital (CCH) in Zambia, launched November 2021 and conducted per available published protocol 12 in accordance to STROBE criteria. 13 This primary study enrolled children to test what EEG and clinical variables are associated with PME development within two years of presentation. All eligible children in the main study cohort were included in this current study comparing CM versus CNS-M PME outcomes. Analyses were performed after all enrolled participants had an opportunity for 12-month follow-up. De-identified study data were managed using the secure, web-based data collection platform, REDCap, hosted by Boston Children’s Hospital. 14
Children six months to eleven years presenting to CCH with suspected malaria and neurologic signs were screened for inclusion in the study. Inclusion required confirmed malaria parasitemia (via rapid diagnostic test with confirmatory blood smear) and meeting the case definition for CM or CNS-M. CM was defined as a Blantyre Coma Score (BCS) of ≤ 2 in children <two years, or Glasgow Coma Score (GCS) ≤10 in children ≥ two years old with coma persisting at least 30 minutes after the last known seizure. CNS-M inclusion required complicated seizures (i.e., ≥15 minutes, focal, or multiple), or impaired consciousness without frank coma (i.e., BCS 3-4, GCS 11-14). Children were excluded if there was pre-existing epilepsy, clinically identified acute CNS co-infection, clinically identifiable toxin ingestion, head trauma within twenty-four hours or any other cause for their neurological condition besides acute malarial infection.
Patient and Public Involvement
The study design was developed with significant input from medical providers in the region, and information about this research was dispersed to the public locally for awareness with feedback from the community and local providers to ensure methodology, and particularly enrollment procedures, were culturally sensitive and appropriate.
Procedures
Data Collection Timeline
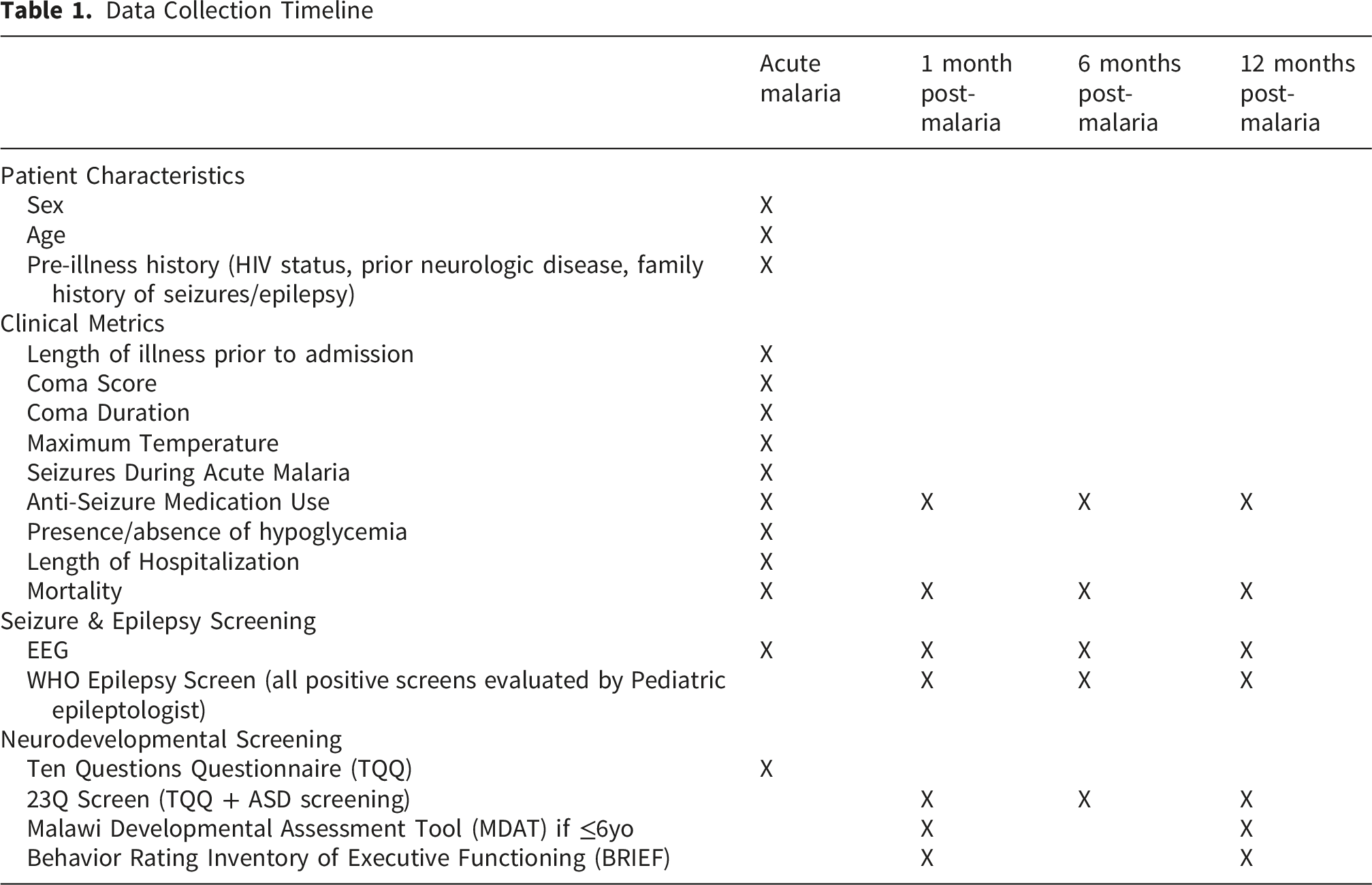
Baseline characteristics collected at enrollment included sex, age, HIV status per caregiver report, and the Ten Questions Developmental Screen (TQQ). TQQ is a regionally validated screen that can identify at least modest neurodisabilities in children 2 and older. 15 Clinical hospitalization data captured included illness duration prior to admission (classified as ≤1 day, 1-2 days, 2-3 days, 3-5 days, 5-10 days, or >10 days), seizures recorded during admission (classified as none, one <15 minutes, or one seizure >15min OR multiple seizures), most severe coma score (BCS or GCS), coma duration from onset to resolution where applicable, maximum temperature, presence of hypoglycemia (defined as <3mmol/l), antiseizure medication (ASM) usage, hospitalization length, and mortality. Follow-up data was collected at one, six, and twelve months post-malaria infection, including a standardized epilepsy screening questionnaire previously used in pediatric CM studies in the region, 3 23Q Developmental Screen, an expanded TQQ with Autism Spectrum Disorder screening validated in Uganda, 16 neurodevelopmental assessment by Malawi Development Assessment Tool (MDAT) 17 if ≤ six years old, and Behavior Rating Inventory of Executive Functioning (BRIEF) Global Executive Composite Scores (BRIEF-P version used in under six years). 18 MDAT scores were compared as pass/fail for age, using standardized cutoffs from regional norms, across four developmental domains (gross motor, fine motor, social, and language). 17 BRIEF Global Executive Composite mean scores were used for comparison between groups, Responses for all items were scored as (1) “Never”, (2) “Sometimes”, and (3) “Often”, with the higher score indicating worse behavioral dysregulation.
Within 48 hours of admission and again at each follow-up, standard 30-minute EEG was recorded by trained EEG technologists, using Natus equipment, XLTEK software with standard international 10–20 system, at sampling rate of 256Hz. EEGs were assessed via secure web-based access by a board-certified pediatric epileptologist (AAP) for qualitative (visual) interpretation. Clinical reports were provided to inform care. For research purposes, three pre-specified outcomes were coded: (1) slowing -utilizing standard norms for age to categorize as no slowing, diffuse slowing, focal slowing, or mixed focal and diffuse slowing; and (2) epileptiform activity, classified as present or absent interictal epileptiform discharges, and (3) electrographic seizures (per ACNS criteria 19 ). If these could not be determined due to technical limitations, the EEG was excluded from that measure. Quantitative EEG (qEEG) analyses, in which digital EEG recordings are transformed, processed and analyzed via mathematical algorithms, were performed to quantify brain activity differences between the CM and CNS-M groups. EEGs were pre-processed using the Harvard Automated Processing Pipeline for Electroencephalography, 20 using low-pass filtering (100 Hz), electrical line noise removal (50 Hz), bad channel rejection, and amplitude-determined artifact rejection. Studies were excluded from qEEG analyses if pre-processing quality was insufficient. Frequency bands, measures of brain waves speed in hertz (Hz), were categorized per conventional EEG bands (delta [0.5-4 Hz], theta [4-8 Hz], alpha [8-13 Hz], beta [13-25 Hz], gamma [25-60 Hz]). Average relative band-power over the entire epoch on a channel-by-channel basis and average approximate entropy, a measure of brain wave complexity 21 was also computed.
Outcomes
All positive epilepsy screens were referred for consultation by a board-certified pediatric epileptologist (AAP), and the primary outcome of PME was made per International League Against Epilepsy criteria, 22 requiring one of the following: (1) an unprovoked seizure at least two weeks post discharge for CM or CNS-M (defining CM/CNS-M as a potentially epileptogenic insult, and therefore a sufficient corroborating risk factor with a single unprovoked seizure, consistent with post-traumatic epilepsy definition 23 ), (2) clinically probable unprovoked seizure(s) and abnormal EEG, (3) at least 2 unprovoked seizures separated by 24 hours. Epilepsy classification as focal, generalized and mixed was determined by clinical semiologies and EEG findings. Secondary outcomes included MDAT, NESS, and BRIEF scores, and qEEG frequency band and approximate entropy comparisons.
Statistical Analyses
The duration of this study was determined by the five-year NIH career development award that supported the research. To maximize sample size and power, consent was sought from the caregivers of all eligible admissions for the duration of the enrolment period which was pre-specified to allow for at least 12-months follow up for the last enrolled.
Demographic, clinical, and EEG metrics were compared between CM and CNS-M groups. Means and standard deviation were used for continuous variables and counts with percentages for categorical variables for summary statistics. Student’s t-test was conducted for continuous variables (Wilcoxon rank sum test for smaller sub-samples) and Fisher’s exact test for categorical variables. qEEG data were aggregated for each group at each time point (admission, one-month, six-month, and 12-month), for comparison. Cohen’s d was calculated for qEEG findings to demonstrate effect size. Comparisons between groups were performed based upon available data; missing data reported. Data analysis was performed using SAS v.9.4.
A proportion of enrolled children (n=21) overlapped with the randomized, placebo-controlled clinical trial of aggressive antipyretic therapy (FEVER) 24 from November 2021-June 2022 seven of whom received the intervention. In FEVER, the intervention was shown to decrease maximum temperature and reduce seizure severity. Sensitivity analyses removing (4 CM, 3 CNS-M) participants exposed to the FEVER intervention from the analyses were performed to assess the potential impact of this intervention on results.
Results
There were 183 children who met initial inclusion criteria for whom caregivers consented to participate; 61 with CM and 122 with CNS-M. 42 (13 CM, 29 CNS-M) did not complete 12-month assessments, thus were excluded from main analyses. Among those excluded, there were no significant differences between proportion of CM and CNS-M, nor in baseline demographics or reasons for loss to follow-up, including mortality (Supplemental material: Group comparisons Table s1, Causes of mortality Table s2). 141 remaining participants were included in main analyses (CM n=48, CNS-M n=93). Figure 1. Study flow diagram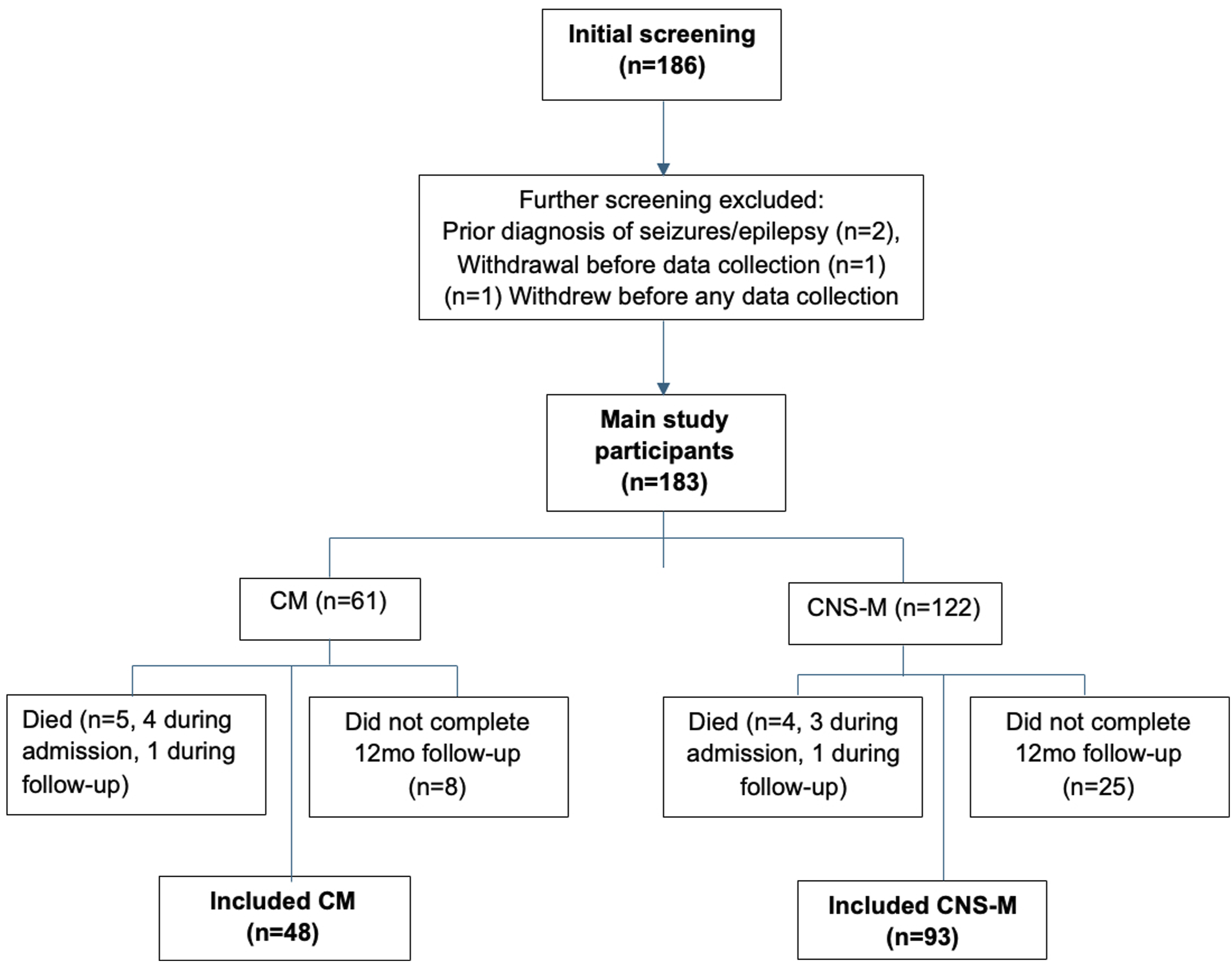
Baseline Characteristics
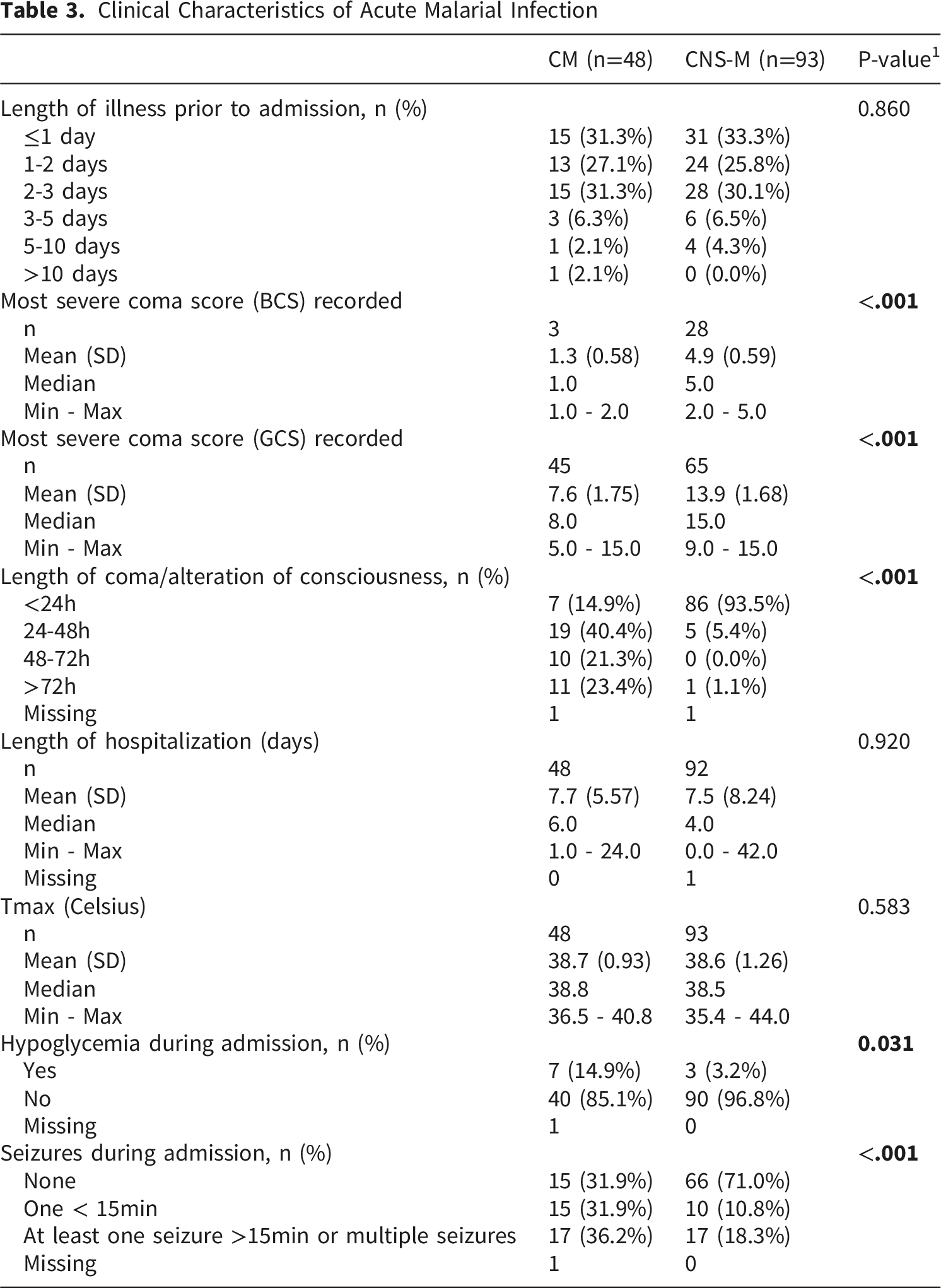
Clinical Characteristics of Acute Malarial Infection
An overall PME rate of 18.4% (26/141) by 12 months was found. PME rates were not statistically different between groups. CM had a 14.6% (7/48) rate and CNS-M 20.4% (19/93) rate, p=0.495. Despite the baseline age difference in between CM and CNS-M groups, PME rates remained not statistically different between the two groups when controlling for age, p=0.503 (Supplemental materials, Table s3). Proportion of males who developed epilepsy was also not significantly different (5/9 (55.6%) male in CM versus 14/19 (73.6%) male in CNS-M, p=0.188), neither was mean age (43.8 months in CM vs 40.92 months in CNS-M, p=0.400). However, type of epilepsy (focal versus generalized/mixed) was statistically different between groups, with 2/7 (28.6%) CM patients having focal epilepsy compared to 15/19 (78.9%) of CNS-M patients, p=0.028. Figure 2. PME outcomes. (A) Epilepsy occurrence by 12 months post-illness did not differ significantly between groups, with 14.6% in CM and 20.4% in CNS-M cohort developing PME, p=0.495; (B) Distribution of epilepsy diagnoses by first positive screening showed expected increase with time; (C) Proportion of males and females between groups were not significantly different (55.6% male in CM versus 73.6% male in CNS-M), p=0.188; (D) Percentage of focal epilepsy was significantly higher in the CNS-M group (78.9% vs 28.6% in CM), p=0.028
ASM usage at CCH during acute illness on PME outcomes was not different between groups, with 4/32 of CM patients and 4/21 of CNS-M patients who received ASMs developing PME, p=0.698. Usage of ASM did suggest a lower risk of developing PME overall (OR 0.66, 95% CI [0.26, 1.64], with this association still seen when the groups were analyzed independently, with lower risk of PME with ASM use seen in the CM cohort (CM (OR 0.57, 95% CI [0.11, 2.95]); CNS-M (OR 0.88, 95% CI [0.26, 3.00])); however, these findings did not reach statistical significance. Figure 3. Impact of ASM usage on PME risk. Although not statistically significant, usage of ASM did suggest a lower risk of developing PME overall (OR 0.66, 95% CI [0.26, 1.64], which remained present when segregated by cohort (CM (OR 0.57, 95% CI [0.11, 2.95]); CNS-M (OR 0.88, 95% CI [0.26, 3.00]))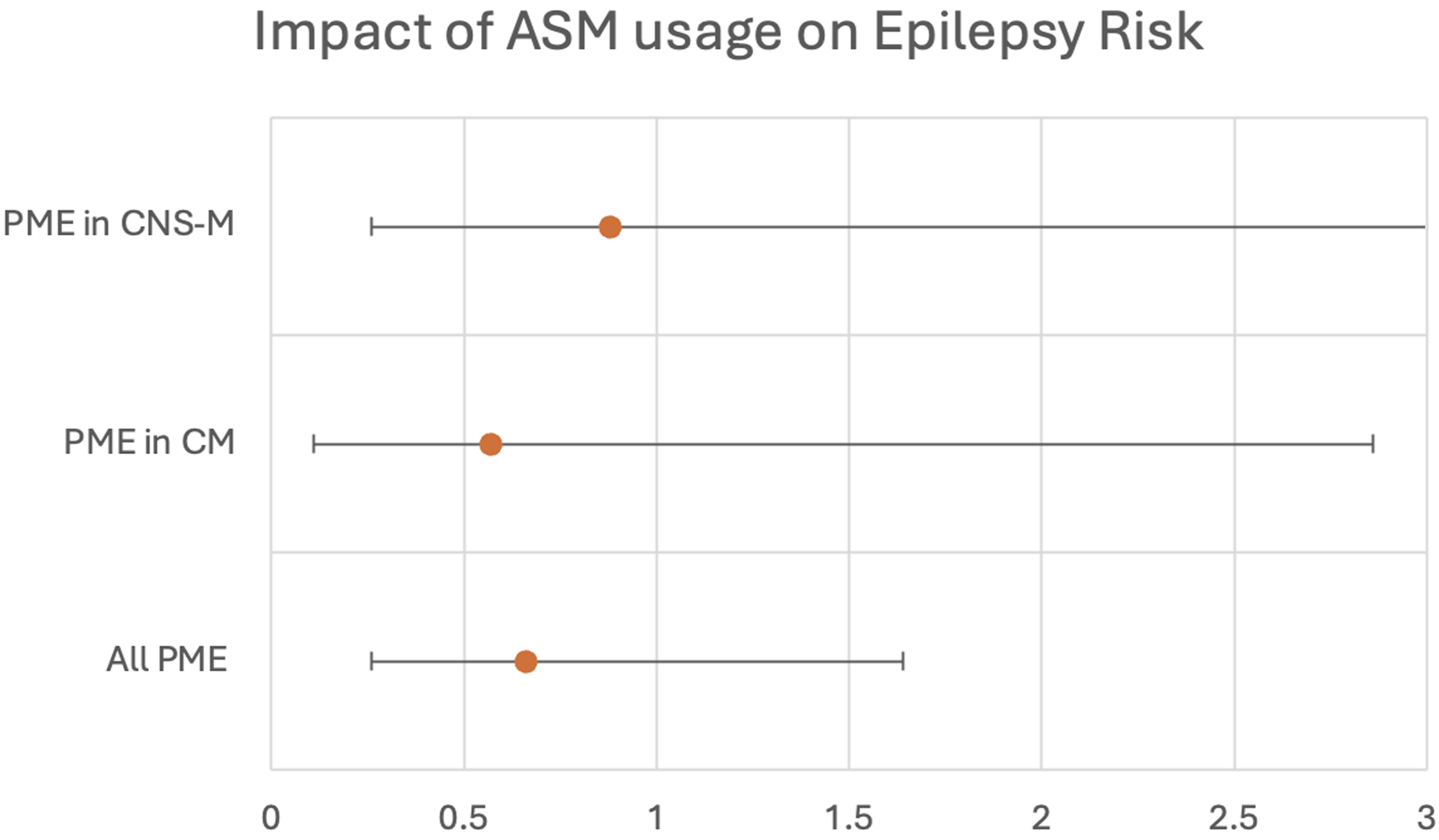
On qualitative EEG review, CM children had more frequent slowing at admission (44/48, 91.7%) compared to CNS-M (60/89) (4 studies excluded as indeterminate), 67.4%), p=0.001, as expected given comatose presentations (although EEGs were done within 48 hours of admission, so CM participants could have resolved coma by time of recording). There was increased epileptiform activity in CM (14/47 (1 study indeterminate), 29.8%) versus CNS-M (12/90 (3 studies indeterminate), 13.3%) at admission, p=0.024. Presence of acute electrographic seizures was not statistically different between groups, with 3 CM and 1 CNS-M, p=0.112. At one-, six- and 12-month EEGs, there were no significant differences across groups in any visual measure. Figure 4. Visual EEG Findings. Reporting the percentage positive of relevant metric out of those that could be reliably classified; if missing study or unable to determine due to technical limitations, study was excluded for that metric. Children with CM had higher rates of slowing (91.7% vs 67.4%, p=0.001) and epileptiform activity (29.8% vs 13.3%, p=0.024) upon admission; there were no other significant differences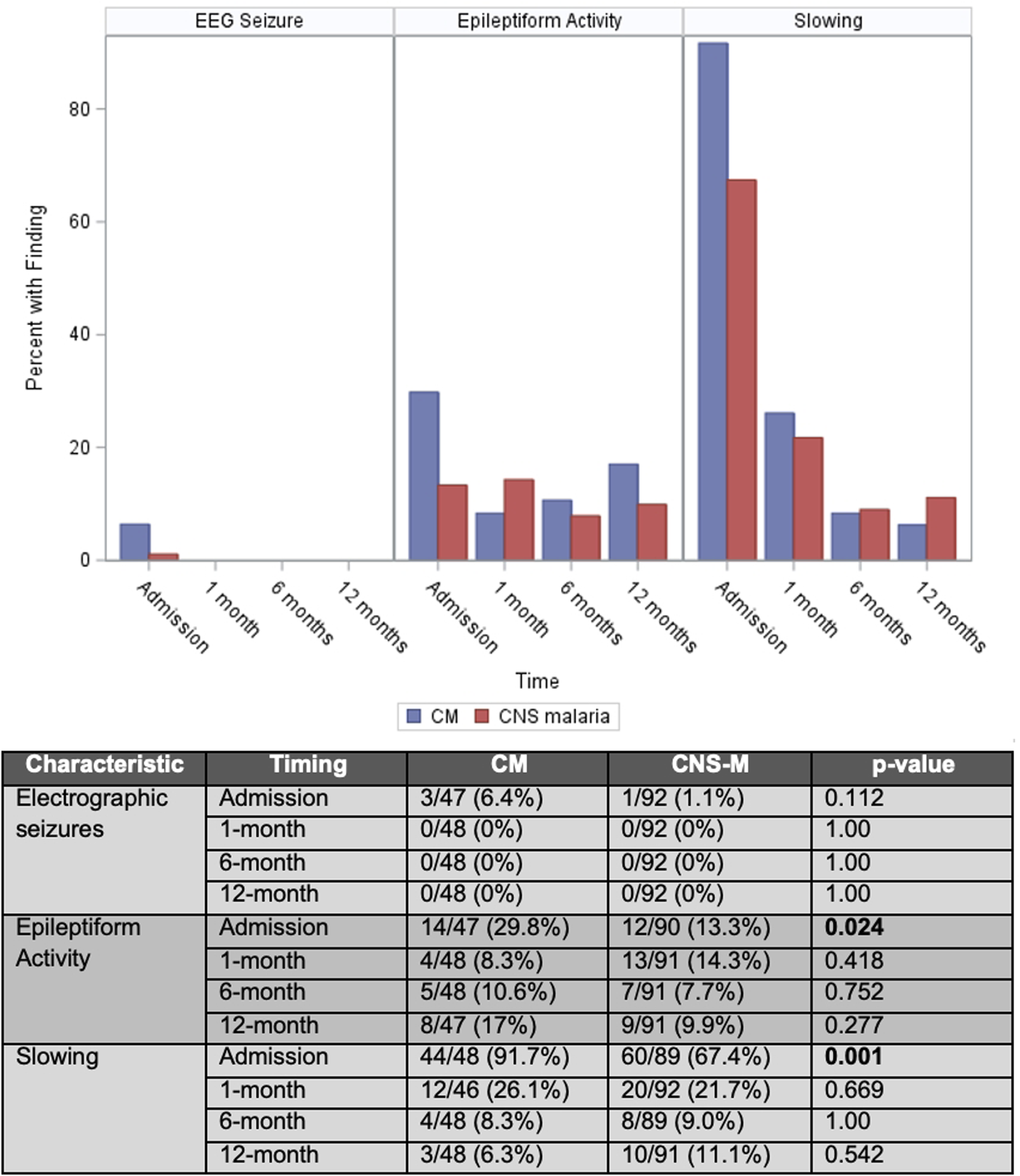
During acute illness, qEEG findings identified CM with significantly increased delta power (0.931 ± 0.007 vs. 0.892 ± 0.004), reduced theta power (0.035 ± 0.002 vs. 0.067 ± 0.002) and alpha power (0.010 ± 0.001 vs. 0.016 ± 0.001), p< 0.01. Gamma frequency activity, which was lower but not significantly so at admission in CM, became significantly lower by one-month (0.009 ± 0.001 vs 0.013 ± 0.0001), p<0.001. By six months, gamma frequency was now higher in CM versus CNS-M (0.015 ± 0.002 vs. 0.013 ± 0.0008), p<0.01; CM also had significantly lower delta power (0.781 ± 0.007 vs. 0.808 ± 0.005), higher theta power (0.127 ± 0.004 vs. 0.118 ± 0.003, higher alpha power (0.051 ± 0.002 vs 0.040 ± 0.001), and higher beta power (0.024 ± 0.001 vs. 0.019 ± 0.001) compared to CNS-M, p<0.01. By 12 months, the differences were less marked but remained significantly different in delta power, which remained lower in CM (0.769 ± 0.008 vs. 0.783 ± 0.006), alpha power higher in CM (0.057 ± 0.003 vs 0.050 ± 0.002), and higher beta power in CM (0.025 ± 0.001 vs 0.022 ± 0.001), p<0.01. Approximate entropy (ApEn) was significantly different between groups in the acute and early recovery (1-month phases), with lower ApEn in CM vs CNS-M at admission (0.385 ± 0.013 vs. 0.508 ± 0.008, p<0.01) and at one month (0.0531 ± 0.010 vs 0.555 ± 0.008, p<0.01). There were no significant differences between groups at six- or twelve months in qEEG. Figure 5. Quantitative EEG Findings across Frequency Band Power and Approximate Entropy. (A) Differences in frequency band content shows that acutely, CM patients had increased delta and lower theta and alpha frequency content, by 1-month, only gamma power was significantly lower. By 6-months, there was a separation between groups that showed a significant difference across all frequency bands, with CM having lower delta, and higher theta, alpha, beta, and gamma frequency power. By 12-months, delta power remained lower in CM, and alpha and beta power remaining higher. (B) Approximate Entropy (ApEN) was significantly lower in CM for up to a month acute malarial illness, but then normalized by 6 months, remaining similar across groups at 12-months. The magnitude of difference was most notable for ApEN during acute illness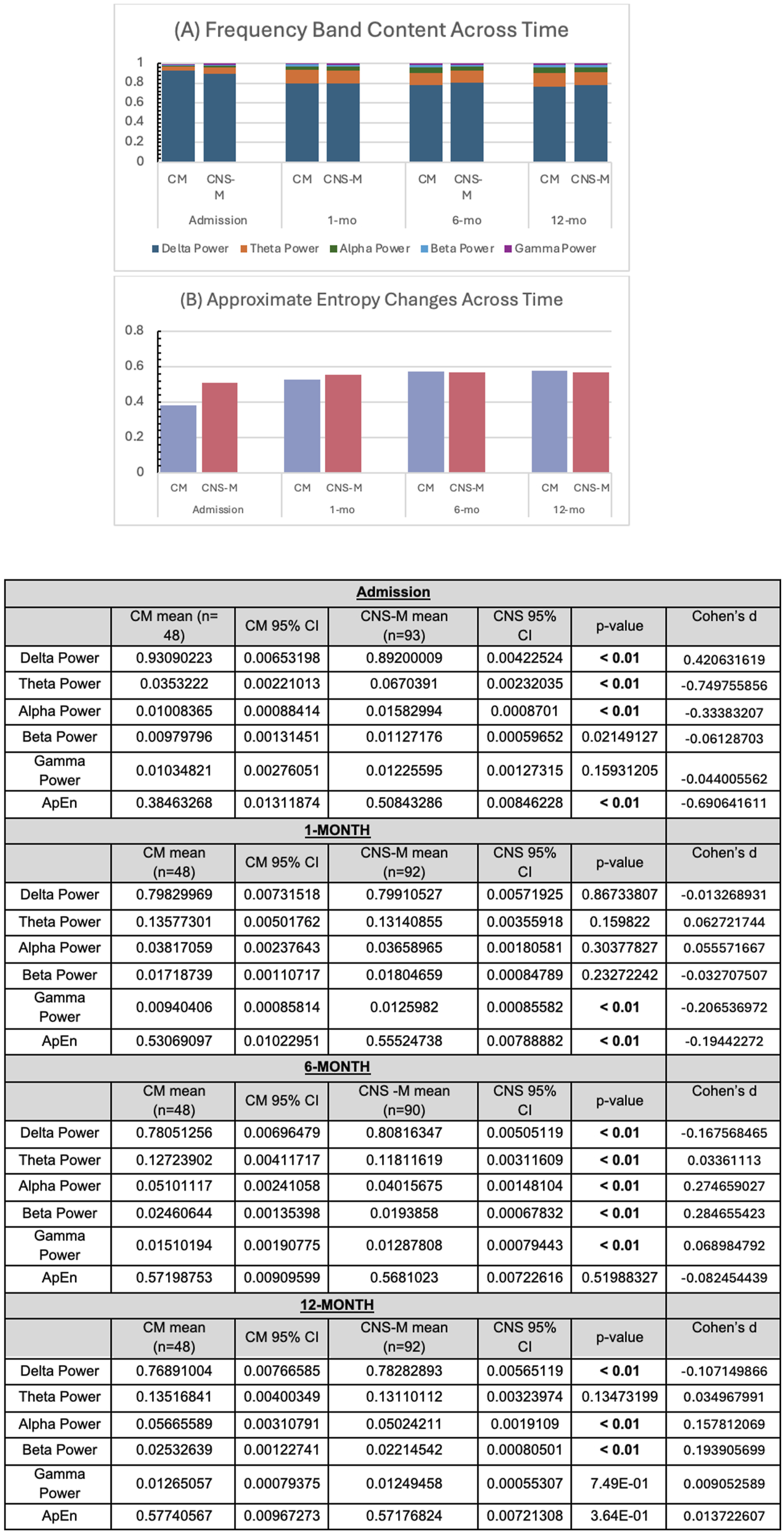
For children under age six years, MDAT failure rates per neurodevelopmental domain (gross motor, fine motor, language, and social development) were computed using normative age cutoffs.
17
Out of the 113 children who were eligible and completed MDAT at one month, 19% failed in at least one domain with no significant difference between groups (20% (7/35) CM vs 19% (15/78) CNS-M, p=0.924). Out of the 107 children who were eligible and completed MDAT at 12-months, 13% failed in at least one domain with no significant difference between groups (15% (5/33) CM vs 12% (9/74) CNS-M, p=0.672). There were also no significant differences between CM and CNS-M groups in failure rates at 1- and 12-mo respectively when compared across individual domains: Gross motor 2.9% vs 7.7%, p=0.433 and 6.9% vs 5.6%, p=1.00; Fine motor 8.6% vs 7.7%, p=1.00 and 7.1% vs 7%, p=1.00; Language 5.7% vs 7.7%, p=1.00 and 7.1% vs 7.1%, p=1.00, Social 11.4% vs 11.5%, p=1.00 and 10.3% vs 6.9%, p=0.686. Figure 6. Percentage of each cohort that failed the Malawi Developmental Assessment Tool. There was no significant difference across domains between CM and CNS-M patients (Gross motor 1mo, p=0.433, 12mo, p= 1.00; Fine motor 1-mo p=1.00, 12-mo p=1.00, Language 1mo p=1.00, 12mo p=1.00, Social 1mo p=1.00, 12mo p=0.686)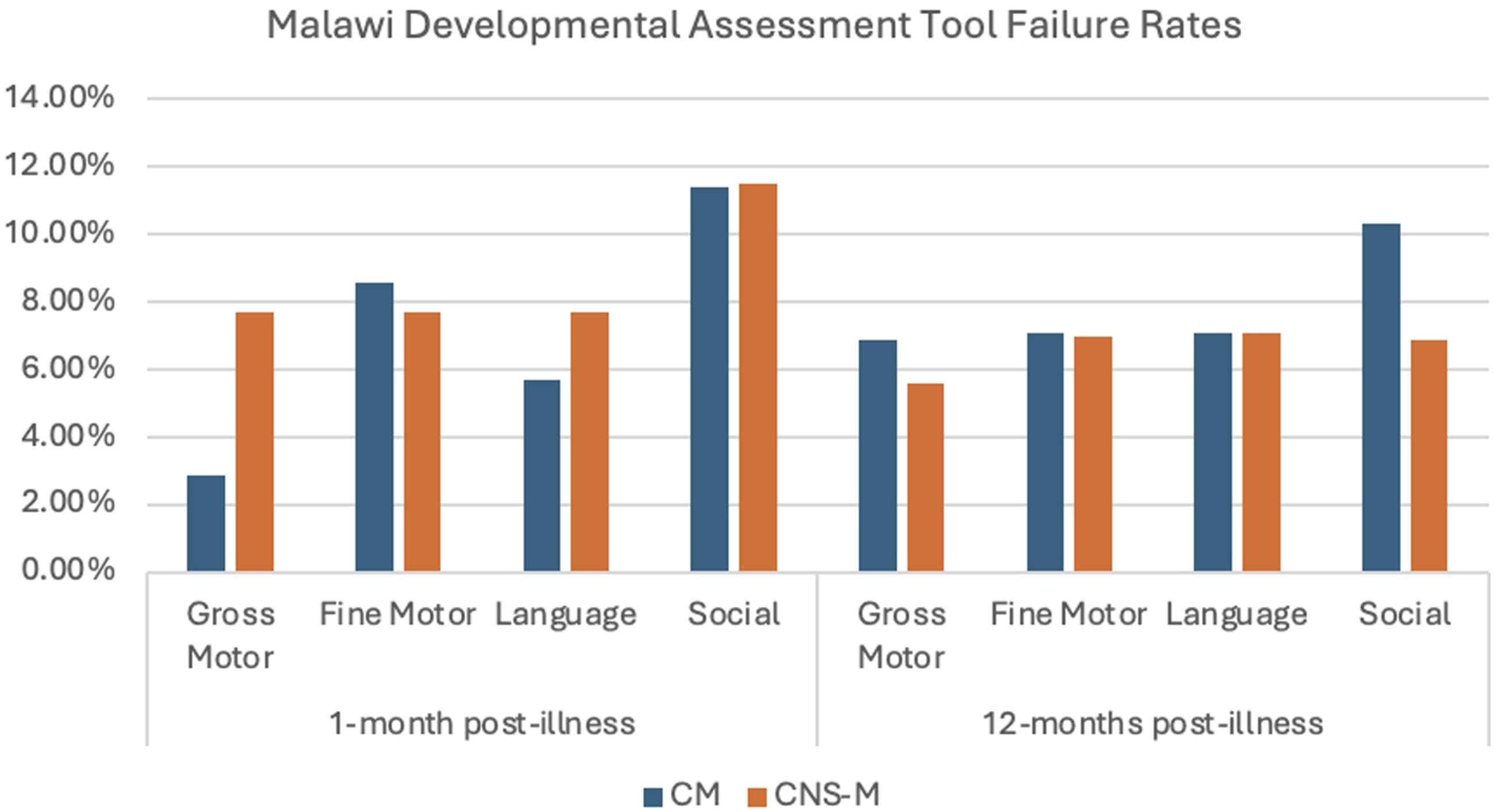
Behavioral outcomes assessed by composite BRIEF score means were compared between groups, stratified due to different versions used for under 6 years and 6 years and over. For those under 6 years of age, possible raw global composite score range was 63 (all “never”) -189 (all “often”), and for those over 6 years of age, it was 86 (all “never”) – 258 (all “often”). At one-month, mean scores for under six years were 69.3 (SD 8.30) in CM and 70.9 (SD 16.72) in CNS-M, p=0.581, and for over six years of age, mean scores were 90.9 (SD 5.6) for CM and 90.5 (SD 8.85) for CNS-M, p=0.900. At 12-month reviews, under six-year-old mean scores were 65.7 (2.68) for CM and 67.7 (10.78) for CNS-M, p=0.317 and over six-year-old means 87.4 (1.88) for CM and 88.8 (3.51) for CNS-M, p=0.297.
Sensitivity analysis excluding the seven study participants included in the overlapping FEVER study 24 who received the intervention (30mg/kg load of acetaminophen followed by 15mg/kg acetaminophen plus ibuprofen, 10mg/kg, every six hours, for 72h) noted several findings. When the children who received aggressive antipyretics in the context of the clinical trial were removed from the analysis, the increased frequency of hypoglycemia in CM no longer reached significance (6/44 CM (14%) vs 3/90 (3.3%), p=0.058) compared to whole cohort (6/48 CM, (14.9%) vs 3/93 CNS-M (3.2%), p=0.031). Additionally, the six-month qEEG findings of decreased theta and gamma power in CNS-M compared to CM was no longer significant. The directionality of the findings was not different in the sensitivity analysis compared to the primary analysis. Full sensitivity analyses available in Supplementary Material, tables s4.1-4.8.
Discussion
In this prospective cohort study of Zambian children admitted to a rural district hospital for malaria with a spectrum of neurological signs and symptoms, we found that CNS-M was twice as frequent as CM, and that children with CNS-M and CM had similar neurologic outcomes, most notably high PME rates at one-year post-illness.
Our entire cohort (CNS-M and CM) had an overall rate of 18.4% PME at one-year post-malaria, notably higher than the 9-16% by two years post-malaria that is reported in the literature.3,4,7 This could be attributed to CNS-M inclusion. Additionally, participant caregivers underwent detailed counseling and close monitoring for seizures, including routine epilepsy screens with EEG, and low threshold for pediatric epileptologist consultation, which may have facilitated capturing subtler focal and non-motor seizures. Finally, we utilized the 2014 ILAE definition for epilepsy 22 developed in context of traumatic brain injury literature, counting CM/CNS-M as a potentially epileptogenic injury thus allowing a single unprovoked seizure to meet diagnostic criteria with this risk factor, 23 compared to the older standard requiring two unprovoked seizures separated by 24 hours. These factors allowed more sensitive and early capture of PME.
Delayed epilepsy diagnoses lead to higher seizure-related morbidity and mortality. Self-limited, non-motor seizures often are not recognized as seizure until occurrence of a more dangerous convulsive event, even if multiple non-motor seizures occur. 25 Given the relatively brief period between the index event and epilepsy presentation in PME and the PME incidence, our findings highlight the need and probable utility of dedicated discharge counseling after acute pediatric malaria with neurologic symptoms on signs/symptoms of different seizure types, and close follow-up for screening of seizure occurrence. The short latency between the malaria infection and epilepsy development, as well as the high rates of epilepsy, also make PME an ideal condition for studying human epileptogenesis, and a potential model for interventions to mitigate acquired epilepsy development after an epileptogenic insult.
The pathophysiology of CM and neurological outcomes, which have been more extensively studied than CNS-M, are still not fully understood. Multiple mechanisms have been identified, from parasitized red blood cell sequestration in cerebral vasculature leading to decreased perfusion and hypoxia, cerebral edema, and microvascular hemorrhages as well as blood brain barrier breakdown, cytokine, and inflammatory responses. 26 Whether CM and CNS-M share pathophysiology remains unknown. In our study, length of illness prior to admission was not significantly different between groups, and was consistent with the typical short time course (24-72h) of severe malaria with neurological signs reported in the literature. 27 This suggests that CNS-M is not simply an early stage of CM. Our study supports CM as causing more severe acute neurological dysfunction with CM children having higher rates of hypoglycemia, clinical seizures, interictal epileptiform activity, and qEEG findings suggestive of more severe cortical dysfunction demonstrated by more marked slowing and decreased entropy. A notable limitation of our study was the lack of assessment for malaria retinopathy. 28 Standard retinal examinations are usually not possible in an awake, ill, and often uncooperative child. Future studies utilizing rapid, mobile phone based retinal images in CNS-M could potentially help determine if the retinal findings of CM are also seen in CNS-M. 29
Alternatively, CNS-M may have different pathophysiological mechanisms than CM. The most common feature of CNS-M in this study was complex seizures. Febrile seizures in general do carry a risk of subsequent epilepsy, with literature reporting approximately occurrence in approximately 2-10% of children, with higher risk in complex febrile seizures.30,31 However, the rates after malaria with complex seizures is notably higher than this, with work from Kenya showing a PME rate of 11.5% after CNS-M7, and our study showing a rate of 20.4%. This suggests that febrile convulsions due to malaria are different than general febrile seizures, and at the minimum, carry a significantly higher risk warranting different anticipatory guidance than is appropriate after a single complex febrile seizure in the setting of a non-malarial fever.
Further studies on CNS-M are needed to better understand risk factors by age, particularly as mean age did not differ in PME outcomes, suggesting younger children are overall at higher risk of sequelae in both groups. There were also a higher proportion of males (68.8%) in the CNS-M cohort, which may be due to cultural norms, 32 with male children being brought for medical attention for what would be considered a less severe condition compared to the more severe presentation of CM, which had a more proportional ratio (43.75% male). Data from Zambia looking at the impact of healthcare user fees has suggested that prioritization of a female child’s healthcare is less than a male child’s, with user fees associated with less female presentations. 33
As noted, our qEEG data was consistent with expected more severe findings in the comatose- or recently so- CM patients. During the recovery phase, however, a shift was seen from increased lower frequency content in CM to CNS-M. This may reflect normalization, as CNS-M was younger on average, and brain wave frequencies are normally slower in younger children, with increased delta and theta frequency activity expected. The one-month and six-month differences for gamma frequency activity are more intriguing. While not reaching level of significance acutely, CNS-M had more gamma frequency activity at admission, which became statistically significant by one-month, but by six-months had significantly lower gamma frequency to CM. Our group previously found acute increased gamma frequency is associated with PME risk, supporting a hypothesis that gamma frequency activity is a biomarker of epileptogenesis, with an initial peak at time of brain insult, followed by slow decline over the critical period of epileptogenesis.12,34 The gamma frequency pattern and slightly higher PME rate found in the CNS-M group is supportive of this hypothesis, however this must be interpreted with caution given lack of statistical significance. Further studies are required to better determine the relevance of the qEEG findings.
Due to the more common presentation of overt seizures in the CNS-M group, we suspect the CNS-M group were more likely to receive ASMs prior to admission than CM, although a limitation of our study was that this data was not captured systematically. In our setting, pre-hospitalization ASM usage was predominantly diazepam, with phenobarbital also rarely available. Out of the 53 children who received ASMs in the hospital, the majority received diazepam and phenobarbital, with rare use of carbamazepine and levetiracetam. Levetiracetam was only consistently available through a medication grant to the hospital and thus use limited. The availability and use of these specific ASMs highlights the limitations of acute seizure care in lower resource settings, such as Zambia. While epilepsy outcomes did not differ between groups, there was a trend of reduced risk of epilepsy with ASM usage, raising the question of whether ASMs should be more routinely given in children with malaria with neurological involvement-even in absence of overt seizures-particularly when EEG is not accessible (and non-convulsive seizures cannot be reliable excluded), if safe options are available. 35 While it has been shown that levetiracetam is a safer and equally efficacious option to phenobarbital in CM35, accessibility remains limited.
Notably, our one-year neurodevelopmental and behavioral outcomes showed some risk of impairment after severe malaria with neurologic signs, particularly in the social domain, with no difference between CM and CNS-M groups, which was consistent with studies from Kenya that found that CNS-M (defined as malaria with complex seizures) had similar risk to CM of developing at least one neuro-impairment post-infection.5,7 Data from Kenya and Uganda has similarly shown executive function impairments and behavioral outcomes did not differ significantly across different neurologic presentations with malaria11,36
A significant strength of this study was being one of the larger prospective cohort studies looking at malaria with neurological involvement with and without coma, with detailed monitoring for PME outcomes, including routine follow-up EEGs and clinical assessments. This allowed for more sensitive capturing of PME data across the cohort. However, there were several important limitations. First, despite efforts to optimize referrals, given geographic barriers, full representation of the regional CM and CNS-M rates is limited, and mortality, specifically, may be underrepresented. Notably, CM mortality is typically over 15%, 37 in comparison to 8.3% in our cohort. This could suggest the most severe cases of CM did not reach our district hospital before death, but conclusions are limited as this study was not powered to assess mortality. Another limitation was the absence of data regarding pre-hospitalization ASMs, limiting understanding of their impact on acute seizures and EEGs during admission. There was also a relatively high attrition rate to withdrawal or inability to trace despite best retention efforts, although impact of this was felt minimal, as there were no significant group differences amongst missing participants. Additionally, while one of the larger prospective studies on neurological malaria, sample size was still limited in assessing sub-group comparisons. Finally, follow-up beyond one year would be important to fully assess long-term neurological sequela.
Conclusion
This prospective cohort study done amongst rural Zambian children identified early (within one year of illness) PME development in approximately one out of every 5 children who survived severe malaria with neurologic signs, including those without coma. While the association in pathophysiology between CM and CNS-M is not well understood, this study’s findings demonstrate an important target for global pediatric epilepsy care. Epilepsy is one of the three leading causes of disability in children aged 5-19 years globally, 38 and acquired causes, particularly in low- and middle-income countries, are a large contributor, with malaria being a significant risk factor for children. Given the high rates of PME after severe malaria with neurologic signs, this population is an important target for education and improved clinical follow-up, to reduce lag time to epilepsy diagnosis in this identified high-risk group and ultimately reduce associated seizure-related morbidity and mortality.
Supplemental Material
Supplemental Material - Following Severe Pediatric Malaria, Epilepsy Screening Is Needed Even Among Children Without Coma: Findings From a Prospective Cohort Study
Supplemental Material for Following Severe Pediatric Malaria, Epilepsy Screening Is Needed Even Among Children Without Coma: Findings From a Prospective Cohort Study by Archana A. Patel, Shaida Nishat, Rasesh B. Joshi, Suzanna Mwanza, Joseph Kasolo, Angela Masempela, Thelma Musakanya, Tina Mwale, Violet Nambeye, Rosemary Nyirongo, Ruth G. Tembo, Nicole O’Brien, Karl B. Seydel, Christopher Cortina, Bo Zhang, Maitreyi Mazumdar, Alexander Rotenberg, Gretchen L. Birbeck in Journal of Central Nervous System Disease
Footnotes
Acknowledgements
The authors thank the participating families in Chipata, Zambia as well as Dr. Mbinga Mbinga and the Paediatrics Department at Chipata Central Hospital, where the research was conducted.
Ethical Considerations
Appropriate ethical approvals for this study were obtained from Boston Children’s Hospital (where data was hosted) (IRB-P00038309), the University of Zambia Biomedical Research Ethics Committee (REF 1186-2020), and the National Health Research Authority of Zambia (NHRA-2683/09/09/2025).
Consent to Participate
Written informed consent was obtained from caregivers for all included children in local languages by native-speaking research team members. If the caregiver was illiterate, the consent was read with a witness, and acknowledged by thumbprint.
Author Contributions
AAP, GB, SN, SM, MM, and AR were involved in study conception, and design. AAP, SM, JK, AM, ThM, TM, VN, NO, RN, KS, and RT were involved in data collection. SN, RS, CC, BZ, and AAP planned and executed data analyses. AAP drafted the initial manuscript, and all authors provided revisions and final approval for publication, as well as agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute Of Neurological Disorders And Stroke of the National Institutes of Health under Award Number K23NS118051 (AAP), with additional support from NIEHS Pilot Grant P30 ES 000002 (AAP, MM), and NIH/NINDS grants R01NS102176, R01NS111057 and R35NS122265 (GB). SN and ThM also received support from the MIT Center for International Studies. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AAP received research grants from NIH/NINDS and NIEHS for the proposed work, has served as a paid consultant for the World Health Organization and Noviguide/Global Strategies and serves on the medical advisory boards of ROW foundation which supplies anti-seizure medications through a donation grant to Zambia and Neurotech foundation, which supplies EEG training and supplies to low resourced regions, including Zambia; GB has received research grants from NIH/NINDS to support the proposed and other work, is on the Editorial board for Lancet Neurology and the Lundbeck Foundation’s Neurotorium and is a consultant for Blue Spark Technologies and Neuro Tech; MM has stock in Pfizer; and AR is co-founder of Neuromotion, PrevEp and Galibra, and has consulted, served on advisory board or received research support from Abbvie, Autifony, Biomarin, CRE Medical, Encoded, Epihunter, Neuroelectrics, Neural Dynamics, NeuroRex, Roche, Takeda, and is listed as inventor on patents pertaining to brain stimulation, drug delivery and gene therapy that are unrelated to the present work. The remaining authors have no conflicts of interest to disclose and declare that the research was conducted in the absence of any relevant commercial or financial relationships.
Data Availability Statement
Full data set available upon review of reasonable written request and establishment of an approved data sharing agreement from relevant institutions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.