
Abstract
Despite the estimated 776 million coronavirus disease 2019 (COVID-19) cases globally, little is known about its impact on immune-mediated neurological disorders such as neuromyelitis optica spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody disorder (MOGAD). Scattered case reports, and reviews address this association, but none have collectively examined the impact of COVID-19 infection or vaccination on established and new-onset NMOSD and MOGAD. Reviewing all published reports of COVID-19 infection and vaccination in NMOSD and MOGAD from December 2019 to October 2024, this report examined the effects of infection and vaccination on patients with established disease and the occurrence of new-onset NMOSD and MOGAD. Outcomes associated with COVID-19 infection in NMOSD and MOGAD patients revealed similar hospitalization rates but a notable difference in deaths in NMOSD patients treated with rituximab. Following COVID-19 infection, twice as many patients developed new-onset MOGAD compared to NMOSD, with a similar larger number of patients who developed MOGAD than NMOSD post-COVID-19 vaccination. While the heavy female predominance in NMOSD is well-established, a greater ratio of male to female patients developed MOGAD post-infection and post-vaccination. Clinicians should closely monitor NMOSD patients with COVID-19 infection, particularly those receiving B-cell depleting therapies, among whom mortality was more frequently reported. The rise in NMOSD and MOGAD following COVID-19 infection and vaccination cases warrants further investigation of the underlying immunological mechanisms. Molecular mimicry and a bystander immune-mediated injury likely play a greater role in central nervous system damage than does direct viral injury.
Keywords
Introduction
An estimated 776 million reported cases of coronavirus disease 2019 (COVID-19) have been documented globally as of January 2025, with over 103 million of in the United States of America. 1 Early in the pandemic, several case reports on COVID-19 infection and multiple sclerosis (MS) were published, with fewer reports on COVID-19 infection in neuromyelitis optica spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody disease (MOGAD). In recent years, an increasing body of data has emerged on the impact of SARS-CoV-2 infection and vaccination in central nervous system (CNS) demyelinating disorders. Although they may share some clinical features, NMOSD and MOGAD differ from MS and each other in having distinct serum autoantibodies, pathogenesis, clinical outcomes, and targeted treatment options.2-5 Despite vaccinations, the risk of COVID-19 infection remains, and new-onset NMOSD and MOGAD have been reported following COVID-19 infection and vaccination.4,6-14
SARS-CoV-2 virus can cross the blood-brain barrier and facilitate the access of COVID-19 antibodies and other autoantibodies to the CNS. ACE-2 receptors that are utilized by the virus to gain access to cells are expressed in the glia and neurons, but there is debate if this virus is directly neurotropic. A study analyzing the CSF of patients with COVID-19 infection revealed evidence of neuroinflammation, including activated T-cells and natural killer cells. Autopsy studies of patients who died with COVID-19 infection showed macrophage infiltrates, CD8+ T-lymphocytes, and microglial activation in the brain, even without any detectable virus.15,16
In this review, we summarize the impact of COVID-19 infection and vaccination in patients with NMOSD and MOGAD, and we identify the occurrence of new-onset cases of these disorders. Previous work on the impact of COVID-19 infection in MS has demonstrated an association of infection with an MS exacerbation. 17 Moreover, coronaviruses have been considered as a possible etiologic agent in MS after two coronaviruses were isolated from autopsy brain tissue of two MS patients who died. 18 Murray’s group used in situ hybridization and detected coronavirus RNA in 50% of their MS brain samples. 19 These observations suggest a potential role for coronaviruses in CNS demyelination, extending beyond MS to related disorders such as NMOSD and MOGAD. Certain strains of coronavirus mouse hepatitis virus have been shown to cause CNS demyelination following resolution of infection in mice, with lesions histologically resembling those seen in patients with MS.20-22 Together, these findings raise concern for similar associations in NMOSD and MOGAD following COVID-19 infection and vaccination.
Methods
A narrative review approach was chosen to account for the various study designs in the literature – including case reports, case series, and systematic reviews – and to provide a comprehensive overview of COVID-19 infection and vaccination in NMOSD and MOGAD. A literature search was conducted on the PubMed, SCOPUS, EMBASE, Cochrane, Google Scholar, and Ovid databases to identify relevant articles reporting on NMOSD or MOGAD and COVID-19 infection or COVID-19 vaccination. The searches were run in November 2024, with an updated search completed on December 16, 2024. The search strategy included keywords COVID-19, COVID-19 infection, SARS-CoV-2, COVID-19 vaccine, vaccination, neuromyelitis optica, neuromyelitis optica spectrum disorder, and myelin oligodendrocyte glycoprotein antibody disease.
Inclusion/Exclusion Criteria
Publications were included if they were in English and reported either: (1) established NMOSD and MOGAD diagnosis with outcomes following COVID-19 infection, or (2) new-onset NMOSD or MOGAD cases occurring after infection or vaccination, provided they met diagnostic criteria and had reported positive aquaporin-4 or MOG antibody levels. Cases were excluded if they did not have sufficient clinical data (e.g., unclear diagnosis or missing antibody status) or if the data were duplicated from previously included publications. When available, data on antibody testing methods (e.g., cell-based assay [CBA] and antibody titers) were extracted and summarized (Supplementary Table 1). Each study was carefully reviewed to avoid duplication or overlapping cohorts. When uncertainties regarding study inclusion or exclusion arose, these were discussed with SD or KWR to reach consensus.
Study Section
The first reviewer (JH) screened all of the articles, selected the relevant articles for inspection and excluded duplicates. All eligible articles were retrieved and managed in a single reference manager (EndNote).
Data Extraction
The same reviewer extracted the following information from each article into an Excel spreadsheet: author, publication year, country, study design, patient demographics data, disease duration, clinical presentation, disease-modifying therapy (DMT), MRI findings, COVID-19 laboratory findings, NMOSD or MOGAD antibody status, vaccine name, number of doses, number of days post-vaccine, key findings, and clinical outcomes. The vaccines that were used varied by country; therefore, we categorized them into platform types – non-replicating (NR) viral vector, mRNA-based, and inactivated – and by their corresponding product names (Supplementary Table 2). Descriptive data analysis was conducted to present data as frequencies and percentages from reported cases in a case analysis approach.
Results
COVID-19 Infection in Patients With Established NMOSD
Summary of COVID-19 Infection in NMOSD
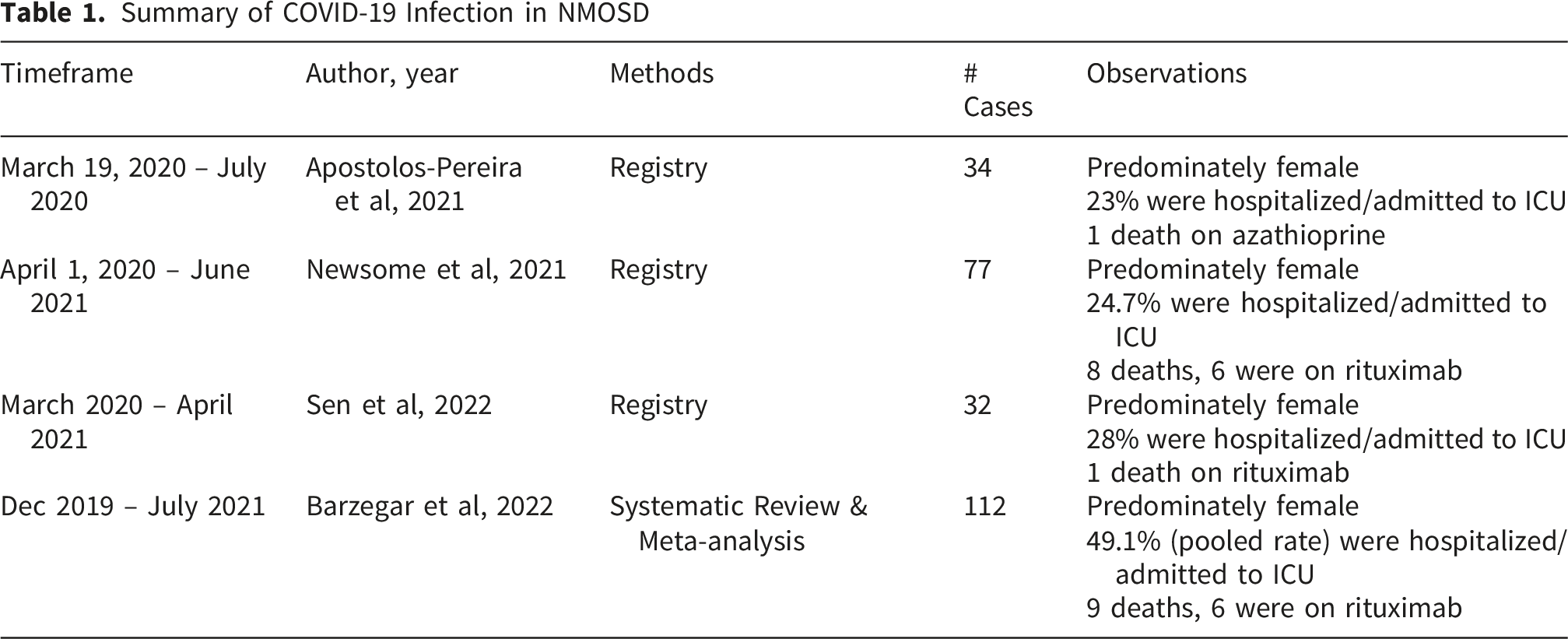
In reported NMOSD cases with COVID-19 infection, more than 50% of patients were treated with rituximab. However, the Brazilian cohort differed, with approximately 47% receiving mono- or combination therapy with azathioprine, followed by 44% on mono- or combo-therapy with rituximab. Most were fully ambulatory. The most common comorbidities reported were hypertension, diabetes, obesity, and dyslipidemia. At least a quarter of the cases required hospitalization and/or admission to the intensive care unit (ICU). Among those, a total of 19 deaths occurred, with an estimated 68.4% of the deaths occurring in those treated with rituximab.2,5,23,24
The US Food and Drug Administration (FDA) has approved four treatments for NMOSD: eculizumab in 2019, inebilizumab and satralizumab in 2020, and ravulizumab in early 2024. Several of the clinical trials for these treatments overlapped with the pandemic. During the open-label period of the N-Momentum trial, 17 cases of COVID-19 infection were reported in NMOSD subjects treated with inebilizumab, all of whom were women; 53% required hospitalization and/or ICU admission, and two deaths occurred due to COVID-19-related complications. 25 Two other cases of COVID-19 infection were reported in inebilizumab-treated NMOSD, both with favorable outcomes and did not require hospitalization.23,24 Eculizumab and ravulizumab were utilized and/or studied in several disease states during the pandemic with no new safety signals. Among eight reported cases of COVID-19 infection in eculizumab-treated NMOSD patients, one required hospitalization/admission to ICU.2,23,24,26 During the satralizumab clinical trials, five mild to moderate cases of COVID-19 infection were reported, all of which resulted in complete recovery.27,28
COVID-19 Infection in Patients With Established MOGAD
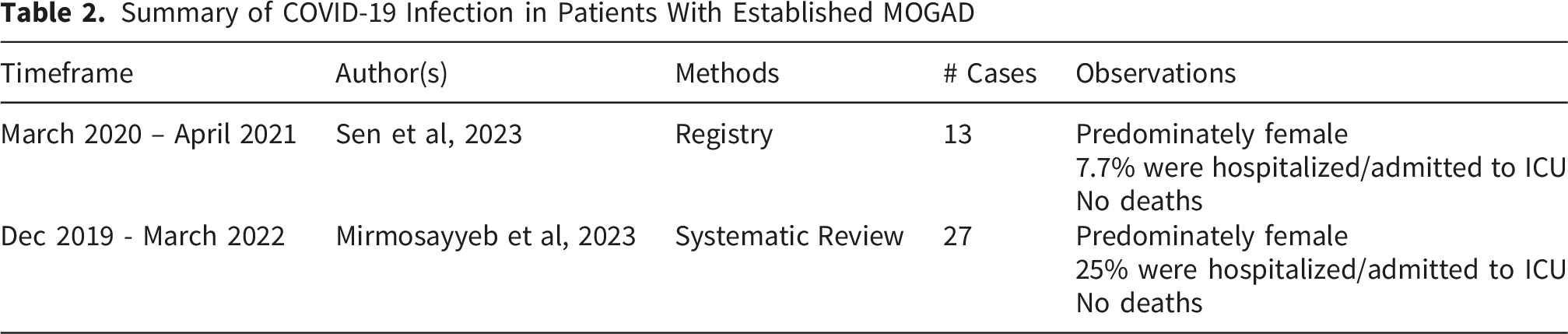
Summary of COVID-19 Infection in Patients With Established MOGAD
COVID-19 Infection and New-Onset NMOSD
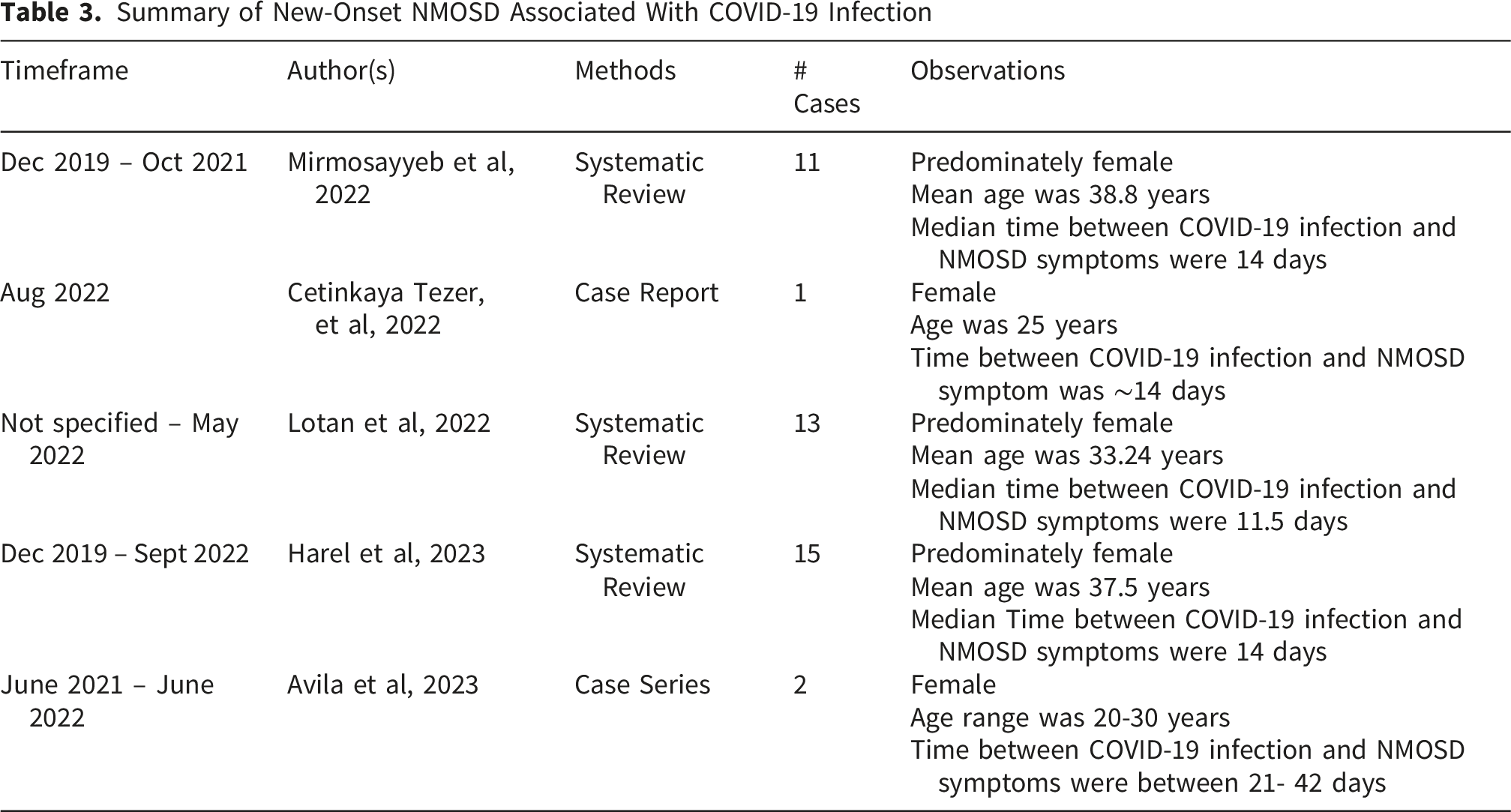
Summary of New-Onset NMOSD Associated With COVID-19 Infection
COVID-19 Infection and New-Onset MOGAD
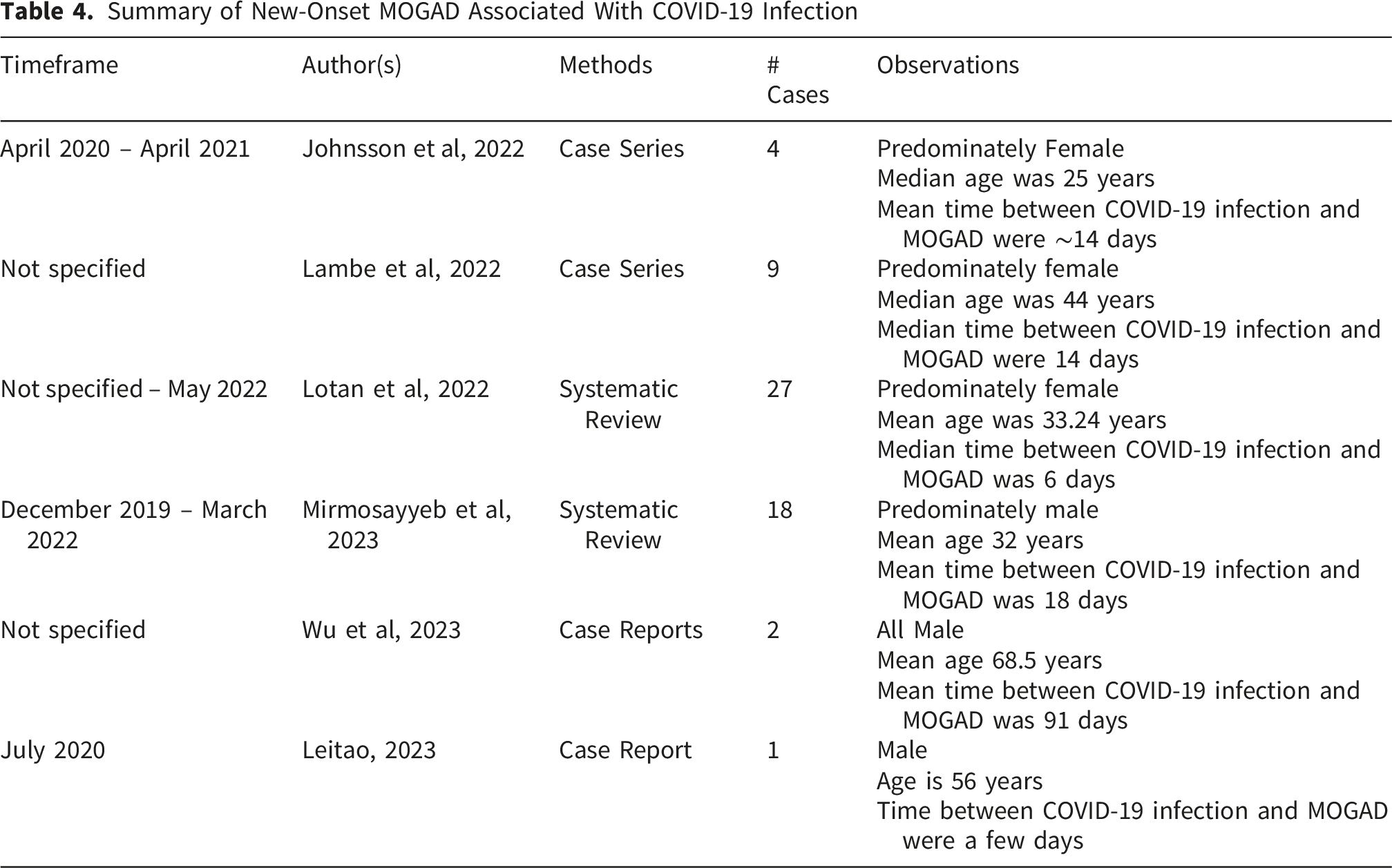
Summary of New-Onset MOGAD Associated With COVID-19 Infection
New-Onset NMOSD Post-COVID-19 Vaccine
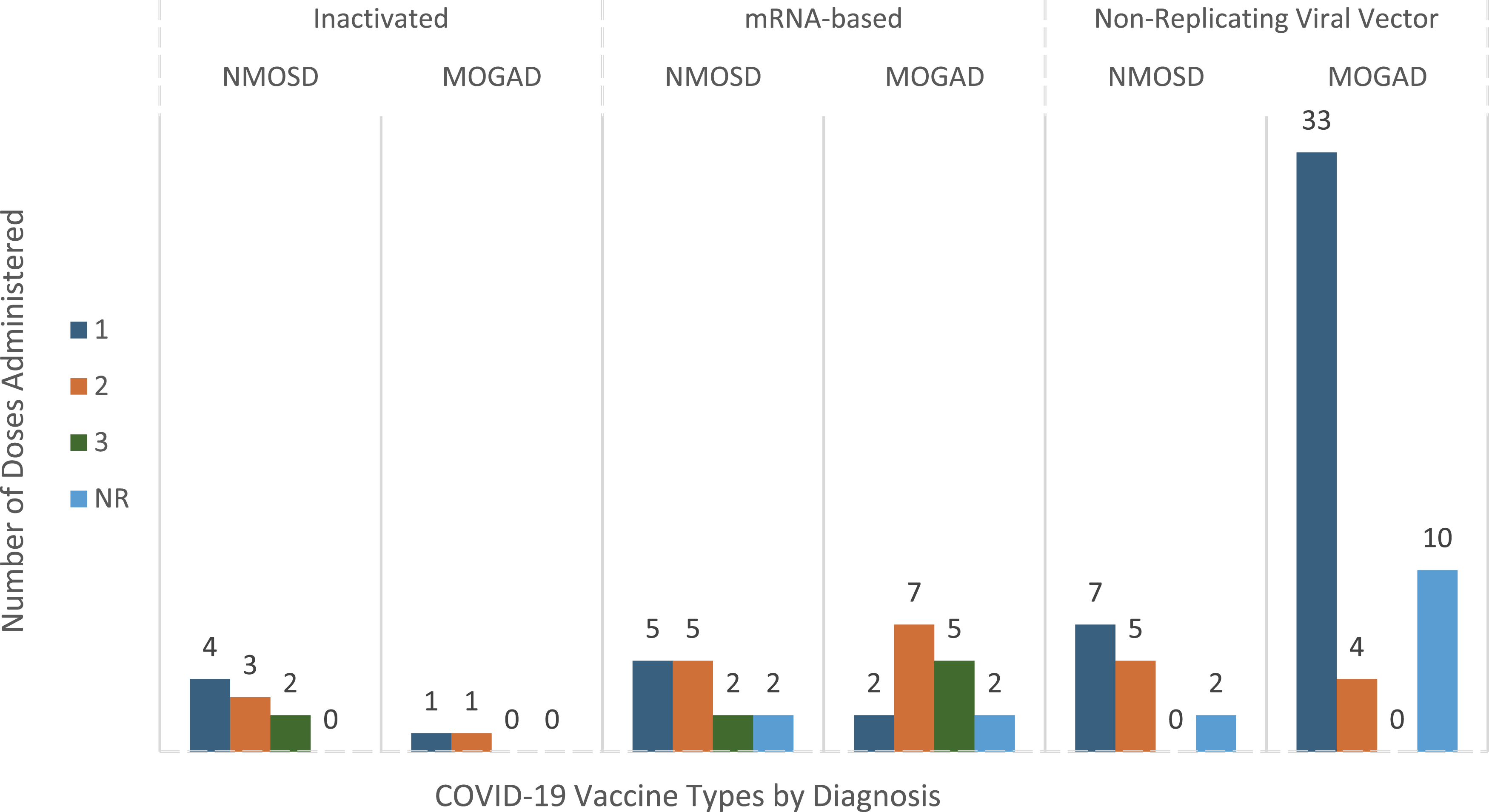
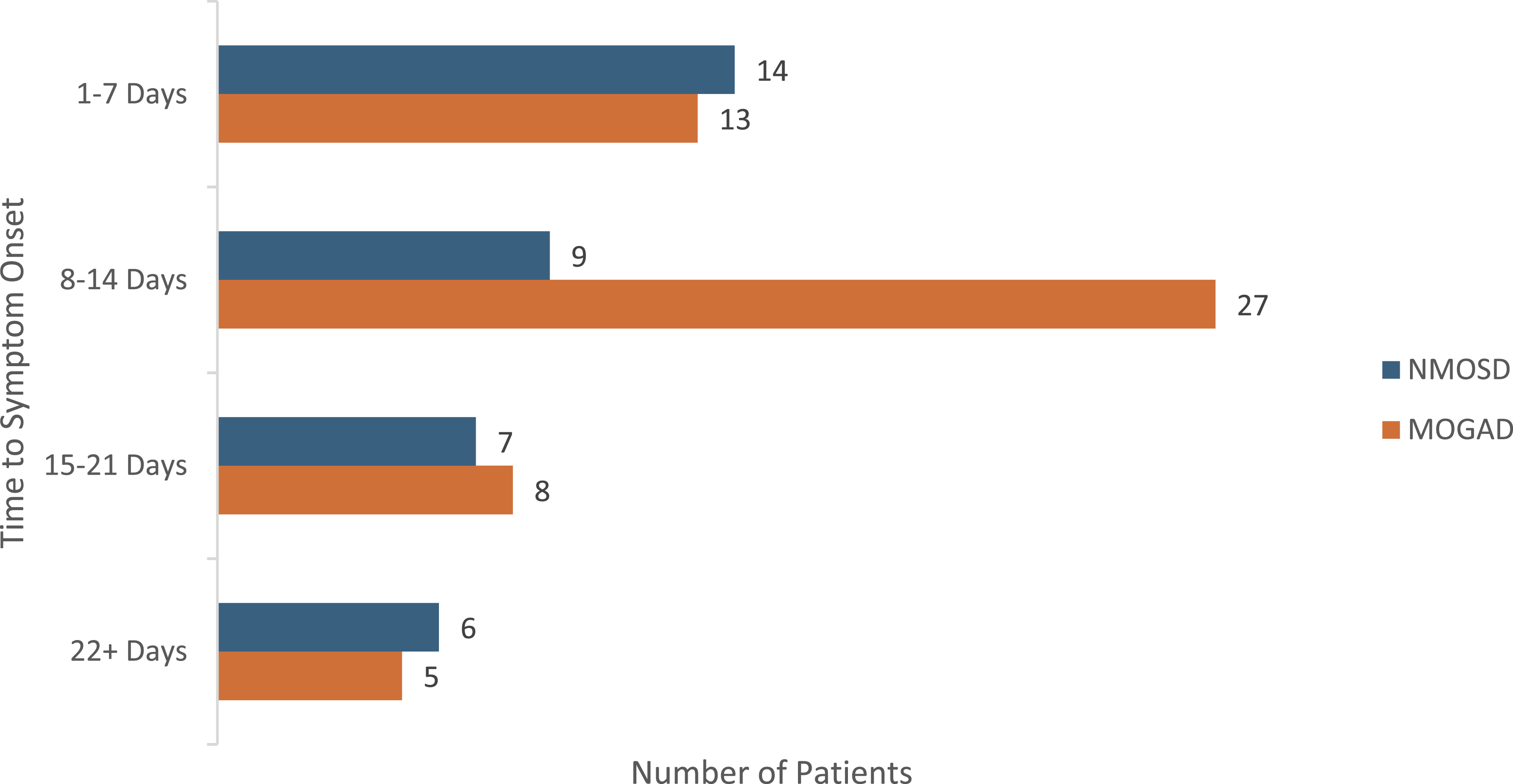
After eliminating double-seronegative and duplicate cases from numerous reviews, registries, observational studies, and case series/reports, 37 unique cases of new-onset seropositive NMOSD following COVID-19 vaccination were identified. The geographic distribution of these cases showed that India accounted for the highest number of reported cases. Females comprised 68% of cases, with a mean age of 49 years at the time of presentation. TM presenting as either isolated TM or LETM occurred in 70% of the cases, followed by brainstem/area postrema syndrome (APS) and ON (Figure 1). All had positive AQP4-IgG antibodies (S1). Neurological symptoms most frequently occurred after their first COVID-19 vaccine (43%), followed by the second (35%) and third dose (11%). Four cases did not report the vaccination dose; therefore, percentages are based on the number of cases with available dosing information. However, all cases did report the vaccine type: 38% received a non-replicating viral vector vaccine, 38% received a mRNA-based vaccine, and 24% received an inactivated vaccine (Figure 2). The mean time between vaccination and the onset of neurological symptoms was 14 days (range: 1–42 days) (Figure 3), with a median of 10.5 days. A single outlier case of 81 days was excluded from the analysis due to uncertainty regarding its temporal relationship with vaccination. Most patients had a favorable outcome with IVMP and/or PLEX treatment. However, several patients experienced only partial recovery; fewer had no recovery, and one death occurred due to respiratory insufficiency and complications following cyclophosphamide treatment.7,33-42 Post-vaccination clinical presentation in MOGAD and NMOSD. Figure 1 presents the distribution of initial clinical phenotypes following COVID-19 vaccination in patients with new-onset neuromyelitis optic spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody disease (MOGAD). Transverse myelitis (TM), including both isolated TM and longitudinally extensive transverse myelitis (LETM), accounted for the majority of cases (70%) in NMOSD. Simultaneous ON and TM at onset occurred in 6% of MOGAD cases and in 0% of NMOSD cases. Only cases with available clinical presentation data were included; cases with missing data were excluded. Abbreviations: ADEM: acute disseminated encephalomyelitis; APS: area postrema syndrome; LETM: longitudinally extensive transverse myelitis; MOGAD: myelin oligodendrocyte glycoprotein antibody disease; NMOSD: neuromyelitis optica spectrum disorder; ON: optic neuritis; TM: transverse myelitis. ON & LETM indicates the simultaneous occurrence of optic neuritis and longitudinally extensive transmyelitis Analyzing post-vaccine NMOSD and MOGAD by vaccine type and dose. Number of reported cases of new-onset neuromyelitis optica spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody disease (MOGAD) by vaccine platform (inactivated, mRNA-based, and non-replicating viral vector) and the number of doses (first, second, third, and not reported [NR]). In both NMOSD and MOGAD, neurological symptoms most often occurred following the first dose. Non-replicating viral vector vaccines accounted for the largest proportion of reported cases, particularly among MOGAD cases. Numbers above each bar indicate the total number of reported cases corresponding to the number of doses represented by the bar. Only cases with available dosing information were included for the dose-specific comparisons. Cases with missing data are shown as NR. Abbreviations: MOGAD: myelin oligodendrocyte glycoprotein antibody disease; NMOSD: neuromyelitis optica spectrum disorder; NR: not reported Timing of symptom onset following COVID-19 vaccination in new-onset NMOSD and MOGAD. Distribution of time to symptom onset following COVID-19 vaccination in patients with new-onset neuromyelitis optica spectrum disorder (NMOSD) and myelin oligodendrocyte glycoprotein antibody disease (MOGAD). For NMOSD, the mean time to onset was 14 days (range: 1-42 days), while for MOGAD the mean time to onset was 13 days (range: 2-42 days). The median time to symptom onset was 10.5 days for NMOSD and 11 days for MOGAD. A single case (81 days) was excluded due to uncertainty regarding its temporal association with vaccination. Only cases with available data on time to symptom onset were included. Abbreviations: MOGAD: myelin oligodendrocyte glycoprotein antibody disease; NMOSD: neuromyelitis optica spectrum disorder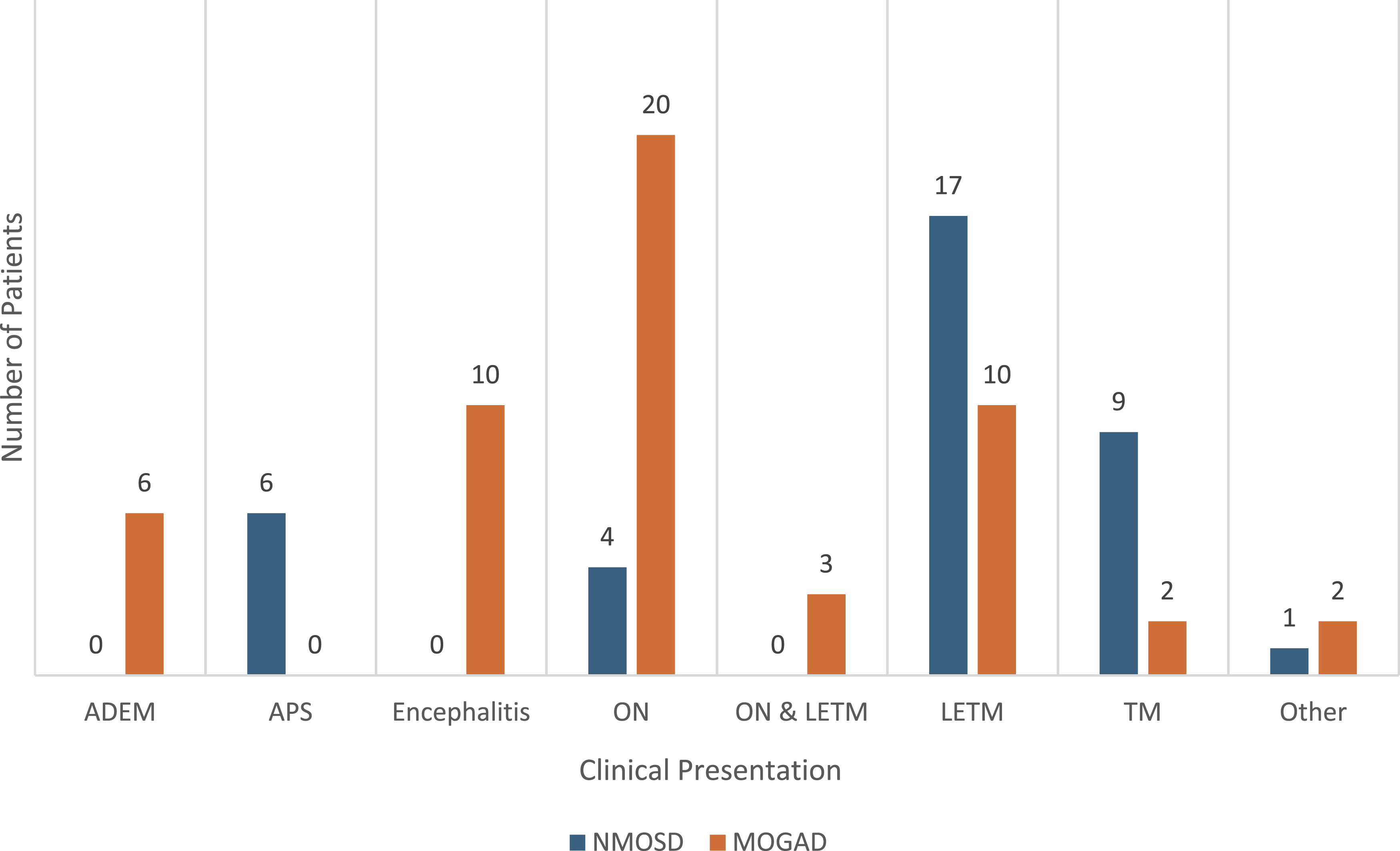
New-Onset MOGAD Post-COVID-19 Vaccine
After eliminating double seronegative and duplicate cases from numerous reviews, registries, observational studies, and case series/reports, 65 unique cases of new-onset seropositive MOGAD following COVID-19 vaccination were identified, with the highest number of reported cases from India. Fifty-seven percent of cases were male and 43% were female, with a mean age at presentation of 42 years, consistent with Francis et al (2023), who reported a median age of 40 years. Excluding the aggregate-only reported cases from Francis et al (2023), the most common first presenting symptom was isolated ON (n=20), followed by TM (n=12), brain/brainstem involvement, and three simultaneous ON and TM cases (Figure 1). Of the 12 aggregate-only cases reported by Francis et al (2023), 10 presented with TM and 2 with ON. All had positive MOG antibodies (S1). The case series (n=12) by Francis et al (2023) reported that the majority received their first COVID-19 vaccine, and two received their second vaccine. Collectively, approximately 71% of all cases (n=46) experienced neurological symptoms following their first COVID-19 vaccine. Including the two from Francis’ group, a total of fourteen cases presented after their second and another five after their third COVID-19 vaccine. Percentages are based on the number of cases with available dosing information. All cases reported vaccine types: 72% received a non-replicating viral vector vaccine, 22% a mRNA-based, and 6% an inactivated vaccine (Figure 2). Analysis of the 53 cases with complete data demonstrated a mean time between vaccination and symptom onset of 13 days (range of 2-42 days), with a median of 11 days. A prior UK case series reported a median onset time of 15 days (range: 6-41 days) 38 (Figure 3). All patients received IVMP and/or PLEX, except one case that required IVIG, and achieved complete or partial recovery. No deaths were reported.33,37,38,43-66
Discussion
The SARS-CoV-2 pandemic that started in December 2019 is the third in a recent series of outbreaks related to novel coronaviruses infecting humans. The first, in 2002 was caused by SARS-CoV-1, while the second was due to Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Neurological complications occurred with SARS-CoV-1 and MERS-CoV, and as anticipated, were also seen with COVID-19. 67 The literature is replete with descriptions of neurological complications occurring in the wake of infection or vaccination with SARS-CoV-2 and their impact in patients with demyelinating disorders.68,69 A large unknown at the inception of the pandemic was how patients with MS on a variety of immune-modulating therapies would respond to infection and immunization. Fortunately, the effects of infection and immunization on MS patients who contracted COVID-19 were not as dire as anticipated and have been the subject of a number of previous reviews.70-72
In this review, we assessed all of the available data on two other important CNS autoimmune disorders, NMOSD and MOGAD, to potentially identify trends and outcomes of COVID-19 infection and evidence of new-onset of these disorders associated with the infection or post-COVID-19 vaccination. Our review highlights several key observations of the impact of COVID-19 infection in patients with NMOSD and MOGAD, as well as the potential neuro-immunological complications of COVID-19 infection and vaccination. First, among patients with established NMOSD, those on immune-modulating therapies with a high EDSS and comorbid conditions appeared to be at greater risk of hospitalization and death with COVID-19 infection compared with patients with MOGAD. Among the 255 NMOSD cases, more than 50% were on rituximab, about 25% required hospitalizations or ICU management, and 19 deaths occurred, with 68.4% of deaths among the rituximab-treated. Among the 40 MOGAD cases, 15-44% were on rituximab. Of the 35 patients with available data, 20% were hospitalized, and no deaths were reported. Second, new-onset MOGAD cases (109 combined cases) nearly doubled those of NMOSD (60 combined cases) after COVID-19 infection and vaccination. Among these, 71% of those who developed MOGAD had received only their first vaccine, and 72% of these MOGAD cases received a non-replicating viral vector vaccine. Post-vaccinal NMOSD cases were predominately split between a non-replicating viral vector vaccine (38%) and a mRNA vaccine (38%). Third, unlike the female predominance seen in new-onset NMOSD cases after COVID-19 infection and vaccination, new-onset MOGAD cases were predominately male.4,6,7,9-12,29-66
Limitations of this review include variations in data collection and reporting methods of the studies reviewed, lack of long-term follow-up, and small sample sizes, which limit the interpretation and generalizability of our observations. Antibody testing methods and titers were variably reported across publications; although these data are summarized in Supplementary Table 1, this heterogeneity limits direct comparison across cases. In addition, some publications did not include analysis of their NMOSD and MOGAD data separately. Moreover, compared to NMOSD, there were far fewer cases of COVID-19 infection outcomes in MOGAD published at the time of this review.
A strength of this review is the inclusion of additional published case reports/series that were not included in prior systematic reviews due to the date of their publication. However, reported cases of new-onset NMOSD and MOGAD following COVID-19 infection or vaccination were limited to case reports and small case series. Since the total population at risk is unknown, the incidence and relative risk cannot be determined, and these findings should be interpreted with caution. While these cases highlight a potentially important clinical observation, they should not be interpreted as evidence of increased risk.
The impact of immune-modulating treatment on mortality following COVID-19 infection is worth mentioning. Of the 19 deaths among the 255 established NMOSD cases identified, 13 occurred in patients on rituximab treatment. All except one study reported rituximab as the most common treatment for NMOSD.5,56 Among the four US FDA-approved therapies for NMOSD, none had any mortality other than two patients who received inebilizumab due to COVID-19-related complications.2,4,23-28 This may be related to when they were approved by the FDA and their low utilization during the pandemic. B-cell depletion, while well tolerated and highly effective in controlling disease activity, was associated with more frequently reported COVID-19-related mortality; however, this observation may be influenced by confounding factors such as underlying disease severity, comorbidities, or treatment selection. Vaccination studies in MS patients on B-cell depleters have identified that humoral responses to the antigen are severely blunted, whereas CD4+ and CD8+ cell responses are not only good but exaggerated in subjects who receive vaccinations while on treatment.73,74 Impaired B-cell responses to SARS-CoV-2 following vaccination and infection have been reported in patients receiving B-cell depleting therapies. 75 This may contribute to the more frequently reported mortality among these patients; however, the exact mechanism remains uncertain and may be influenced by confounding factors. In selected cases of severe or prolonged COVID-19 infection, immune serum globulin may be considered.
Several studies have suggested molecular mimicry as a theory to explain new-onset NMOSD and MOGAD following COVID-19 infection and vaccination. Viral proteins of SARS-CoV-2 and human antigens can exhibit homology. There have also been reports of cross-reactivity between COVID-19 antibodies with 21 human tissue antigens, including antigens from the CNS-like optic nerve.65,76,77 On the other hand, a recent publication that evaluated the cross-reactivity between the SARS-CoV-2 spike and nucleocapsid proteins and MOG protein in 21 serum samples did not support a strong association between COVID-19 infection and MOGAD. 78 An alternative theory is that infection and/or immunization may induce CNS damage in some individuals due to an aberrant adaptive and innate immune response, particularly following repetitive vaccination with the same type of vaccine.76,79 Previous work by Wu has reported autoimmune CD4+ T-cells specific to MOG following COVID-19 infection in both of their MOGAD cases. 12 MOG antibodies have also been associated with ADEM following viral infections in younger cases. 80 However, some authors argue that this potentially autoimmune phenomenon is a temporal coincidence and not a causal association, given (at least in some cases) a relatively short interval from vaccination to the onset of disease.47,56
Conclusion
The findings from this review suggest that patients with NMOSD receiving immune-modulating therapies who develop COVID-19 infection may require close monitoring, particularly in the presence of comorbidities or advanced disease. Reported cases of new-onset NMOSD and MOGAD following COVID-19 infection and vaccination highlight the potential temporal association; however, these observations are based on limited data and should be interpreted with caution.
The underlying mechanisms remain incompletely understood and may involve multiple immunological pathways. In some cases, COVID-19 infection or vaccination may act as a potential trigger in individuals with pre-existing susceptibility, although this remains to be fully established. Additional mechanisms may include increased blood-brain barrier (BBB) permeability, molecular mimicry, bystander activation, and spreading of the epitope.7,38,56,76,77 Further research is needed to better characterize clinical outcomes and to clarify the relationship between COVID-19 infection, vaccination, and the development of NMOSD and MOGAD.
Supplemental Material
Supplemental Material - The Impact of COVID-19 Infection and Vaccination on Neuromyelitis Optica Spectrum Disorder and Myelin Oligodendrocyte Glycoprotein Antibody Disease: A narrative review
Supplemental Material for The Impact of COVID-19 Infection and Vaccination on Neuromyelitis Optica Spectrum Disorder and Myelin Oligodendrocyte Glycoprotein Antibody Disease: A narrative review by Jeffrey Hernandez, Silvia Delgado, Micheline McCarthy, Flavia Nelson, and Kottil Rammohan in Journal of Central Nervous System Disease.
Supplemental Material
Supplemental Material - The Impact of COVID-19 Infection and Vaccination on Neuromyelitis Optica Spectrum Disorder and Myelin Oligodendrocyte Glycoprotein Antibody Disease: A narrative review
Supplemental Material for The Impact of COVID-19 Infection and Vaccination on Neuromyelitis Optica Spectrum Disorder and Myelin Oligodendrocyte Glycoprotein Antibody Disease: A narrative review by Jeffrey Hernandez, Silvia Delgado, Micheline McCarthy, Flavia Nelson, and Kottil Rammohan in Journal of Central Nervous System Disease.
Footnotes
Acknowledgements
We would like to thank Dr. James Britton, PhD, Writing Studies Department, University of Miami, for his support in editing the manuscript. We would like to thank Thilani Samarakoon, PhD, of the Lois Calder Memorial Library at the University of Miami Miller School of Medicine, for consulting on data visualizations.
Author Contributions
Jeffrey Hernandez: Conceptualization, Data Curation, Methodology, Formal analysis, Investigation, Writing - original draft, review & editing, Visualization. Silvia Delgado: Analysis and interpretation, Writing - critical revision of the manuscript. Micheline McCarthy: Writing - review & editing. Flavia Nelson: Writing - review & editing. Kottil Rammohan: Conceptualization, Analysis and interpretation, Writing - critical revision of the manuscript, Supervision. All authors reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JH reports a relationship with UHealth, Sanofi, EMD Serono, TG Therapeutics, Novartis Pharmaceuticals, Amgen, Banner Life Sciences, Genentech, Can Do MS, and the Consortium of Multiple Sclerosis Centers that includes: consulting or advisory and/or speaking and lecture fees. SD has received research grants from Novartis and EMD-Serono. MM reports no conflicts of interest. FN reports a relationship with Novartis, Genentech, Sanofi, and EMD-Serono that includes: consulting or advisory and/or speaking and lecture fees. KR reports a relationship with EMD-Serono and Novartis that includes: consulting or advisory and/or speaking and lecture fees; and he has received research grants from Alexion, Novartis, Genentech, and Sanofi.
Data Availability Statement
The data supporting the findings are derived from publicly available sources and are cited in the manuscript. Additional data are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.