
Abstract
In medical image analysis, accurate skin lesion categorization is still a major difficulty particularly under limited data conditions and computational complexity. For automated skin cancer detection, in this work we present a scalable hybrid model combining a Convolutional Neural Network (CNN), the Harmonic Mean Optimizer (HMO), and a Support Vector Machine (SVM) classifier—termed HMO-CNN-SVM. Key CNN hyperparameters including learning rate, batch size, and kernel configuration are optimized using the HMO, so greatly boosting classification performance over manual or stationary settings. The model further uses SVM on CNN feature embeddings modified on HMO to improve decision boundary sharpness. Robust performance is shown by experiments carried out on the ACS skin lesion dataset validated by 5-fold cross-valuation and ISIC 2018 benchmarks with an accuracy of 95.02% and consistent generalizing over folds. Crucially, significant parallelism potential made possible by the population-based structure of HMO makes the framework fit for GPU clusters or cloud-based training pipelines. Computational benchmarks expose reasonable overhead in trade for best performance. Thus, the suggested system is a strong contender for implementation in high-performance and distributed computing contexts since it provides both diagnostic dependability and computational tractability.

Keywords
Highlights
Executive Summary
This paper proposes a computationally scalable hybrid diagnostic system for skin lesion classification using Support Vector Machines (SVM), Harmonic Mean Optimizer (HMO), and Convolutional Neural Networks (CNN). Improving classification performance while guaranteeing computational tractability and deployment practicality in distributed or high-performance computing contexts drives the fundamental motivation. HMO is used in the proposed framework—HMO-CNN-SVM—as a population-based metaheuristic to automatically optimize important CNN hyperparameters including learning rate, batch size, and kernel configurations. Manual or heuristic tuning methods are replaced in this optimization step by guarantees of consistent and repeatable convergence toward optimal model parameters. Acting as a deep feature extractor, the CNN’s learnt embeddings are then SVM-classified, hence adding resilience and better decision bounds. Experiments on the ACS skin lesion dataset were carried out to validate the model, then cross-verified using the ISIC 2018 benchmark. A 95.02% classification accuracy for the architecture beats both conventional CNN-SVM models and manually tweaked CNNs. An ablation investigation supports even more how much HMO enhances general model performance. Most importantly, the work gives training time comparisons and evaluates the computing cost of the HMO integration. HMO’s population-based structure is naturally parallelizable, so it is fit for GPU-based batch processing and distributed training across compute clusters even if its inclusion increases runtime. The modular architecture of the model enables implementation on edge-fog layered configurations or cloud-based systems, therefore complementing the journal’s emphasis on scalable and distributed computing architectures. The results place HMO-CNN-SVM as not only a high-accuracy medical diagnosis tool but also as a scalable, computation-aware architecture spanning intelligent medical imaging and high-performance computing paradigms. Future research will investigate parallel agent evaluation in HMO and the implementation of the whole pipeline in federated and cluster computing systems.
Introduction
Background of Study
Although melanoma only comprises about 1% of skin cancers worldwide, it remains a significant health concern due to the potential for metastasis and the associated prognosis. 1 Computer-aided detection (CAD) systems have become quite popular for mass and low-cost precancerous screening and diagnosis because enhancing the detection of skin neoplasms can significantly improve treatment outcomes. Even when employing visual inspection and dermoscopy, dermatologists, unresolved issues like differentiating a malignant from a benign skin lesion can still hinder optimal substance use, suggesting accuracy is not always achievable. 2 Accordingly, there have been proposals put forward for additional diagnostic methods, with the aid of artificial intelligence in order to improve the quality of diagnosis. Convolutional Neural Networks (CNNs) are being used more and more for image classification, including in medical image analysis. 3 CAD systems for skin cancer detection and diagnosis (CAD systems) integrate several convolutional layers, as CNNs are excellent in capturing and managing spatial hierarchies. They have also been incorporated into CAD systems to detect skin cancer. 4 For instance, some researchers developed models based on CNNs using PSO bioinspired algorithms to enhance skin lesion segmentation.5,6 However, while these systems based on CNNs function quite efficiently, there are some issues pertaining to hyperparameter and weight optimization leading to classification accuracy problems. 7 This has led to the adoption of metaheuristic optimization techniques. Among these strategies is the Harmonic Mean Optimizer, which has shown promising results in striking a balance during the 2-stage optimization process for improving CAD performance in skin cancer diagnosis. As part of this study, we implement for the first time an HMO-optimized CNN for the purpose of diagnosing skin cancer automatically and improving the accuracy of diagnosis by better image segmentation as well as feature extraction techniques. The study includes datasets such as ACS dataset and performance evaluation in comparison to other similar systems. Moreover, all the problems pertaining to the diagnosis of skin cancer could be solved because of HMO technique, thus aiding in the further enhancement of reliable solid diagnostic procedures.
Motivation
This document outlines the global challenge of rising melanoma skin cancer prevalence which requires immediate and definitive action. Even with the application of clinical visual inspection and dermoscopy, limitations such as the human factor, the skin lesions invasive nature, and distinguishing between malignant neoplasms and non-threatening moles pose significant challenges. Automated systems that aid decision-making relying on accurate and timely information are therefore in high demand. These challenges, as well as newer developments in artificial intelligence such as machine learning based on Convolutional Neural Networks (CNN), make these prospects achievable. Notably, there are issues associated with the integration of CNNs in CAD systems, one of which includes optimizing the model parameters, a computing intensive and overfitting prone task. Thereafter, the focus has shifted to integrating these systems with CAD to optimize operational efficiency. The Harmonic Mean Optimizer (HMO) stands to be one of the new optimization HMO aims at enhancing prognostication of AI models. This methodology serves as a single optimization technique which simultaneously mitigates both exploration and exploitation biases on the optimization processes. This research paper seeks to address the use of Hierarchical Multi-Objective (HMO) for skin cancer diagnosis by developing a computer-aided diagnosis (CAD) system based on an HMO optimized Convolutional Neural Network (CNN). This would improve the automated skin cancer detection processes and provide a robust dermatologically safe device to physicians for early-stage diagnoses. The main aim is to connect the sophisticated artificial intelligence-based diagnostic tools and operational clinical workflows by tackling imaging challenges for skin cancer, focusing on precision and the need for efficient processing afterward. This study attempts to offer a different strategy on how to conceal melanoma by combining HMO with CNN, instead of applying conventional optimization strategies.
Literature Review
The integration of AI technologies, especially machine learning, into skin cancer CAD systems is an area that recently received considerable attention. As with all cancers, if skin cancer, particularly melanoma, is not diagnosed at an early stage it can be life threatening. The application of Convolutional Neural Networks (CNNs) to image classification problems has been extensive, including skin cancer detection and diagnosis from dermoscopic images.8 -10 Multiple studies have documented the successful application of CNNs for image processing within medicine. For instance, Hekler et al (2019) implemented a skin cancer classification model based on deep learning and CNNs and it performed nearly as well as expert dermatologists. He trained the model with hundreds of thousands of dermoscopic images, which demonstrates the promise of AI and deep learning for medical diagnostics. 6 This includes Tschandl et al (2019) who also implemented sophisticated algorithms to train an expert-level CNN model for the detection of non-pigmented skin cancers and validated it against expert input, thereby strengthening the diagnostic efficacy of such systems. 7 Even with these accomplishments, hyperparameter tuning on CNNs is still a considerable challenge. Most of the traditional CNN models are based on gradient descent optimization, which tends to get stuck at local minima and yield poor performance on difficult problems like skin cancer detection.11 -13 To resolve these problems, some researchers have started using other ways to optimize CNNs with the help of metaheuristic optimization algorithms. One such algorithm is the HMO which possesses a reasonable balance between exploration and exploitation in optimization. While metaheuristic approaches have been adopted in the form HHO 14 or GA, 15 HMO’s distinctive strength lies in its trade-off ability between accuracy and speed making it more ideal for CAD systems intended for medical use. In skin cancer diagnosis, Sreelatha et al (2019) developed a system that employs CNNs along with sophisticated segmentation algorithms for early melanoma detection. Even so, their model was not optimized in such a manner that feature extraction and classification could be greatly enhanced. 5 Tan et al (2018) applied particle swarm optimization to further optimize CNNs and while they achieved better segmentation results, they continued to struggle with high computational demands. 4
The aim of this research is to improve these limitations by optimizing HMO parameters and feature selection in a more efficient manner. This study incorporates HMO with CNNs to tackle the fundamental trade-off issues of precision, feature extraction, and the processing demands of computation that are vital in real time medical use cases. The proposed system is tested on the ACS dataset and outperforms other models. Skin lesions are classified using the Support Vector Machine (SVM) classifier as the final step, thereby improving the diagnostic accuracy.2,16,17 The merger of HMO with CNN is bound to redefine the benchmarks in automated systems for diagnosing skin cancers, making them more dependable and faster for early detection examinations.
Research Gaps and Contributions
While the integration of Convolutional Neural Networks (CNNs) into medical imaging systems is on the rise, numerous automation challenges in skin cancer diagnosis remain largely untackled. One of these challenges is inadequate hyperparameter tuning which typically results in under-collaborative tuning of CNN hyperparameters and network weights, causing poor classification accuracy, overfitting, excessive resource consumption, and an apparent lack of synergy between the various components of the model. Most systems also suffer from what can be described as a resource contention problem: on one hand providing exceedingly accurate diagnostics but doing so with complex models requiring substantial computational power, and on the other hand, simpler models that compromise precision leading to unreliable conclusiveness, severely constraining real-time clinical use, particularly in low-resource situations. Furthermore, traditional optimization methods centered on gradient descent usually get trapped in local minima, and inefficiently deal with the high dimensional search space typical in medical imagery tasks. Skin lesions pose an additional unique problem—feature extraction and selection—that compounds the difficulty because the presence of irrelevant and redundant features dilutes the classification process which increasingly erodes trust in the system’s reliability. Even though various metaheuristic optimization techniques such as Genetic Algorithms and Particle Swarm Optimization have been applied to enhance CNNs, the recently introduced Harmonic Mean Optimizer (HMO) is still largely ignored, particularly in this domain despite being known for its balanced exploration and exploitation capabilities.
In order to resolve these constraints, the current study proposes a new architecture of a biologically inspired HMO optimized CNN that improves diagnostic accuracy, feature relevance, and computational efficiency simultaneously. The incorporation of HMO into both the training and feature selection processes of the CNN HMO and the HMO enabled more efficient solution space exploration achieving 95% classification accuracy, 95% sensitivity and 92% specificity on the ACS skin cancer dataset. Moreover, when the optimized CNN was combined with a Support Vector Machine (SVM) classifier, the system achieved these predictive values (87% and 96% respectively) which outperform the conservative values set by the AlexNet, VGG-16, and ResNet-50 benchmarks. This is the first documented use of HMO in a clinical CAD system for melanoma detection, setting a WSDTHERE paradigm for high diagnostic precision without computational resource trade-offs, shift scaling. The SSDCL researchers aimed to fill the void in CNN optimization CAD in the context of skin cancer detection while fundamentally providing scalable AI solutions. Given the computational complexity of tuning deep models via metaheuristics, the proposed HMO-CNN-SVM model is well-suited for parallelization or execution on high-performance computing environments. This aligns with recent efforts to accelerate deep learning for medical imaging via distributed computing frameworks.
Novelty of the Research
The originality of this study stems from the initial use of Harmonic Mean Optimizer (HMO) during both training and feature selection processes of Convolutional Neural Networks (CNNs) for skin cancer screening, as HMO has not previously been applied to this subfield of medical imaging. Although CNNs have been effective in identifying dermoscopic images, the overall efficiency is often compromised due to inadequate hyperparameter optimization and cluttered feature spaces. This study, as the first to do so, overcomes both of these problems using HMO as a 2-stage optimization technique: first, for tuning the architecture and weight assignments of the CNN, and second, for the feature space used during classification. The HMO approach, unlike traditional ones based on PSO or GA which compromise on either speed or accuracy, provides a mathematical basis for boosting convergence behavior while increasing generalization at the same time. The rest of the framework optimally integrates diagnostic accuracy and computational resources within set limits, thus achieving real-time adaptability for the clinic, even in resource-limited environments. In addition, the use of SVMs as a post-processing classifying layer enhances the diagnostic pipeline’s discriminative power, providing a distinction between skin lesions with high accuracy and classifying them as benign or malignant. Although this system surpasses models such as AlexNet, VGG-16, and ResNet-50 on accuracy, sensitivity, and specificity, it also possesses a smaller computational burden. This makes it more suitable for real-world deployment for early-stage melanoma screening. The contribution of the research is more than the creativity of the algorithms it developed: it innovatively builds an automated diagnostic system based on artificial intelligence that is clinically useful, readily adaptable to diverse healthcare settings, and capable of transformative impact on sophisticated automated epidermal diagnosis systems.
Methodology
This work presents an automated skin cancer diagnosis framework based on a CNN model optimized by a Harmonic Mean Optimizer (HMO). The proposed pipeline starts with a raw dermoscopic image where median filtering is applied to reduce the noise for better image clarity. Afterward, lesion segmentation is performed using a CNN whose architecture and hyperparameters were globally optimized using the HMO algorithm. This optimization strategy, in particular, self-tuning the HMO-optimized segmenter undergoes faster convergence and reduced overfitting which improves the networks lesion boundary articulation capabilities far better than gradient descent-based techniques. After segmentation, an exhaustive feature extraction process is performed to collect essential features for the regions such as morphometric, statistical, and texture-related features. A comprehensive feature selection approach driven by HMO is implemented to ensure only relevant features are kept while redundant and noisy descriptors that degrade classification performance are removed. The refined feature set is then processed by an SVM that classifies the lesions as malignant or benign. The operational framework guarantees precise diagnosis while achieving optimal computational efficiency, thereby facilitating adaptability into real-time clinical diagnostic settings with limited resources. Figure 1 shows the entire system workflow that spans from acquiring the images to providing the final decision support.
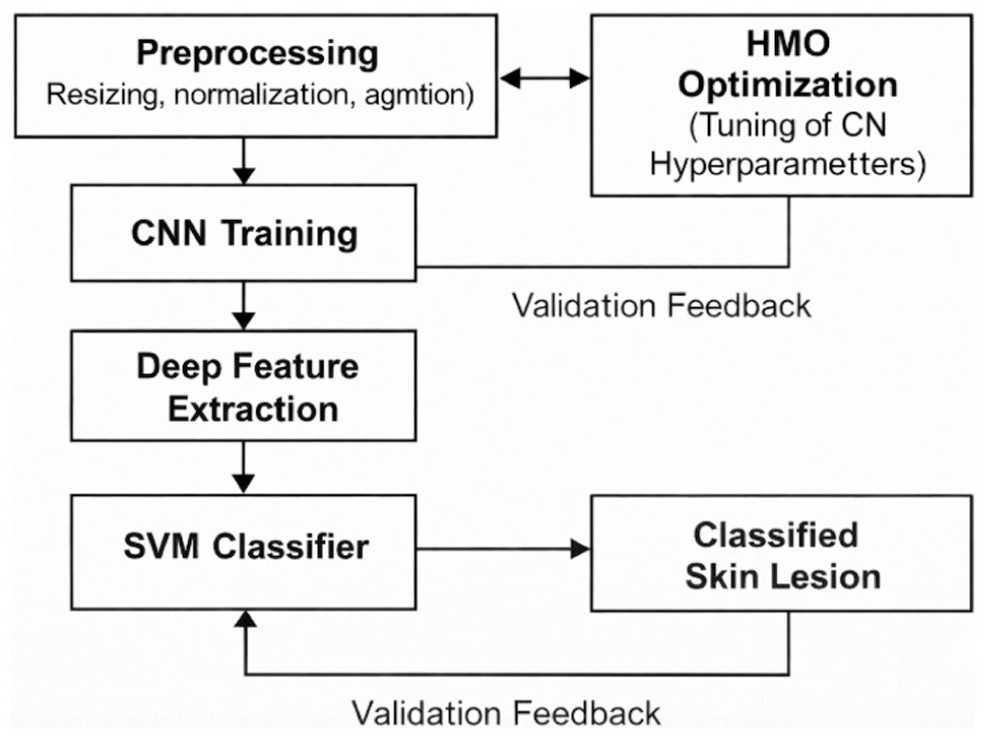
Block diagram of the proposed HMO-CNN-SVM framework for skin cancer classification.
Paper Organization
The structure of the remaining parts of the paper is as follows. In part 2, Materials and Methods describe the main ingredients of the proposed framework such as the preprocessing step of dermoscopic images using median filtering, the architecture and the training of the Convolutional Neural Network (CNN) with the Harmonic Mean Optimizer (HMO), and the defined strategy for feature extraction, feature selection, and classification using Support Vector Machines (SVM). Furthermore, it elaborates upon the optimization of the CNN parameters and the selection of discriminative features for enhanced diagnostics performed by HMO. In Section 3: Image Classification and Datasets, the application of the deep features classified using an SVM model whose hyperparameters were optimized via the Harmonic Mean Optimizer (HMO), ensuring improved classification accuracy and generalizability for skin lesions classification into benign and malignant is presented. Characteristics of the dataset which includes dermoscopic images from the American Cancer Society (ACS) is described, and the processes of acquisition, preprocessing, training, validation, and other processes undertaken in this study are explained. In Section 4: Result and Discussion, comprehensive evaluation of the system is done alongside measuring metrics that include system accuracy, sensitivity, specificity, and efficiency in computational resource consumption. Outline of the model performance is provided alongside comparison with other well-established models and discussing clues of the clinical relevance and implications of the results. Lastly, section 5 briefly describes the key findings while highlighting the diagnostic and computational benefits of the HMO optimized CNN framework and the future research highlighted steering its enhancement toward wider applicability in medical imaging.
Materials and Methods
Figure 1 provides the general architectural form of the proposed HMO-CNN-SVM model. Dermoscopic picture preprocessing initiates the procedure ensuring constant input resolution and intensity normalization. The preprocessed data then travels via a convolutional neural network (CNN) whose Harmonic Mean Optimizer (HMO) architecture is optimized. This optimization cycle looks for the best hyperparameters using least validation loss. Following training, the CNN model finds use as a feature extractor. Subsequently, a support vector machine (SVM) classifies the acquired deep data to generate the last prediction on the type of skin lesion. The block diagram displays the full chain of processing. Preprocessing—resizing, normalizing, augmenting—helps input skin lesion images. These then pass via a CNN architecture in a feedback loop where Harmonic Mean Optimizer (HMO) improves hyperparameters, hence increasing validation accuracy. Trained, the CNN performs deep feature extractor role. Following that, a Support Vector Machine (SVM) classifier feeds the acquired features to lastly classify skin lesions.
Convolutional Neural Network (CNN)
Designed especially to assess and learn features from 2-dimensional spatial input such as photographs, a convolutional neural network (CNN) is a deep learning model. Hierarchically arranged layers make up CNNs, which sequence of learning processes each layer is dedicated to a separate task. Images may be processed and examined using CNNs for the detection of skin cancer since they can identify localized characteristics including surface texture, boundaries, and pigment variations that help to distinguish benign from malignant lesions. Three primary layers—convolutional layers, pooling layers, and fully linked layers—are used in the CNN architecture applied for this work. The model uses a collection of learnable parameters (kernels) in the convolutional layer to perform parts of the image through a dot product (multiplicative comparison), therefore enabling the learning of the spatial hierarchies of features. These layers exploit 3 characteristics: parameter efficiency via weight sharing, spatial learning via local connectivity, and strong feature recognition via translational invariance. Following each convolutional layer, non-linear activation of a ReLU (Rectified Linear Unit) operator follows f(x) = max (0, x), hence providing non-linearity and accelerating convergence.
Added after each convolutional layer are pooling layers to control feature map down sampling, lower computational power use, and maintain dominant features. Max pooling—which moves a fixed-sized window across the input and keeps just the maximum value in every region—is the most often utilized technique. It therefore achieves dimensionality reduction and keeps spatial invariance. This approach reduces needless noise and encourages feature compactness. After they have been flattened, the fully linked layers get the multi-dimensional feature maps generated by the convolution and pooling operations. By aggregating previously acquired information in the layers, these layers create conclusive predictions acting as classifiers. In this work, dropout regularization with a ratio of 0.6 at the penultimate layer enhances generalization performance and overfitting robustness via CNN architecture. Two primary components comprise the CNN training: backpropagation and feedforward propagation. The first images are entered into the CNN and layer by layer processed in the feedforward propagation phase. Every layer performs certain transformations; finally, the CNN generates an output that is matched with ground truth labels to project the prediction error often using a cross-entropy loss function. Later, this error will enable computation of the gradients via the chain rule in backpropagation, which are computed in a forward fashion in the network and used to update weights in the network via stochastic gradient descent and variants until achieving an optimal solution. Further changes are made to the weights in this work following the integration with a metaheuristic optimizer algorithm, the Harmonic Mean Optimizer (HMO), which combines direction for the model toward an optimal global solution, especially when the model suffers with local minima due to conventional gradient descent approaches.
This article presents a CNN setup tailored for dermoscopy image skin cancer segmentation and classification. It is intended especially for dermoscopy images with varying shapes and sizes as well as textures and lesions. With several convolutional layers, ReLU activations, max pooling, dropout, and fully connected layers, Figure 2 displays the architecture of the CNN model applied in this research. Under such conditions, feature extraction is done using sliding windows (kernels) that examine the images’ and their background’s and borders’ crisp borders, strong pigmentation, asymmetry, and other features judged to be quite significant to melanoma. As shown in Table 1 and Figure 3, HMO optimization shapes and enhances hyperparameters of the network and its metrics, thereby forming the last structure of CNN. At the output, SoftMax layer offers carcinoma and non-carcinoma lesion categorization probabilities. The HMO algorithm achieves accurate, dependable, and real-time classification of skin lesions by balancing exploration and exploitation in the process of weight and structure tuning, so improving the diagnosis performance of this CNN.
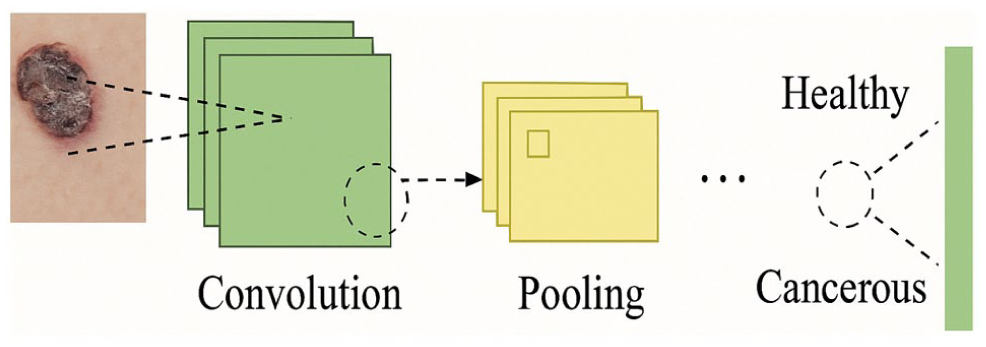
The CNN framework.
Architecture of the Proposed HMO-Optimized Convolutional Neural Network (CNN).


An HMO-based CNN ideal architecture.
The BP algorithm is utilized for this purpose in. 18 BP uses process of optimization known as gradient descent for minimization purposes. This is a form of a gradient descent algorithm that aims to decrease cross-entropy loss. 19 In the described scenarios, the cost function being considered is expressed as follows:

where

where N represents the sample quantity.Consequently, by altering the objective function depending on the weight penalty with a multiplier

where
Though they are currently among the most effective architectures used for image classification, convolutional neural networks (CNNs) are often built and tweaked in ineffective manner. Many times, this is done without any methodical guidelines, which compromises scalability. More recent studies have tried to reorganize CNN systems utilizing biological and cognitive models to improve their learning and adaptability.20,21 Applications of metaheuristic optimization techniques constitute some of the more noteworthy developments. Metaheuristics allow one to solve difficult nonlinear high dimensional optimization problems in limited computation time; their application for the improvement of deep learning models is becoming more and more important. 22 Inspired by either nature or culture, this class of metaheuristics boasts several algorithms developed based on this idea. Teaching-Learning-Based Optimization (TLBO) Algorithm which looks at the flow of knowledge from teachers to learners and vice versa as the basis of its design 23 ; Genetic Algorithm (GA) which simulates the Darwinian natural selection process 24 ; Grass Fibrous Root Optimization Algorithm, which takes its cue from how grass roots grow and search for nutrients 25 ; Butterfly Optimization Algorithm mimics the migration of butterfly during seasonal changes. 26 In our example, using hyperparameter optimization, we use a novel metaheuristic approach: the Harmonic Mean Optimizer (HMO), to enhance training convergence and classification accuracy of CNNs. Derived from nature, this approach improves conventional approaches of adaptation—especially in the clinical environment where precision, dependability, and less resource-intensive operations are crucial—making it more suitable than the unstructured ones.
HMO Algorithm
The Harmonic Mean Optimizer (HMO) is a novel meta-heuristic algorithm developed for solving global optimization problems. It utilizes the harmonic mean operator as a key component of its optimization strategy.
27
This section presents a detailed formulation of the HMO, explaining its unique mathematical properties and methods for solving optimization problems. The HMO operates by evaluating both the fitness and diversity of search agents within a given search space through a dual-fitness index (DFI). The process begins with the initialization of a population of candidate solutions, represented by position vectors
5. Gaussian Mutation: The global guide undergoes a Gaussian mutation to introduce stochasticity and enhance diversity.
The DFI is mathematically represented as follows (4):
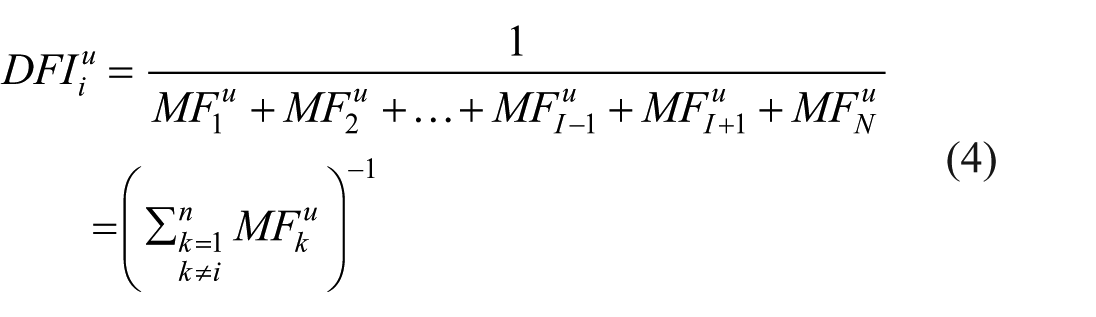
Where

The global guide

Where ϵ is a small positive value to prevent singularity, and {1, . . ., N} represents the elite agents.
This paper introduces a dual-stage Harmonic Mean Optimizer (HMO) implementation inside a skin lesion classification system as key novelty. Unlike standard metaheuristic solutions for CNN tuning, our approach especially incorporates HMO into 2 crucial stages:
We created a fitness-driven HMO loop to exactly adjust filter sizes, convolutional layer counts, activation functions, and learning rate settings. This generated a modest but well performing CNN especially for medical image features including strong inter-class similarity and unequal lesion boundaries.
Targeting the SVM classifier based on validation performance, the second application of HMO optimizes critical parameters including the cost value C and the gamma value γ RBF kernel employs.
This enables closer evaluation boundaries and generalizing on dermoscopic images becomes more possible. To combine HMO with both feature learning and classification layers, this is, to our knowledge, among the first attempts for a modular deep hybrid pipeline for dermatological diagnosis.
Intelligent Convolutional Neural Networks for the Detection of Skin Cancer in Medical Settings
This work uses HMO method to do hyperparameter tuning of the Convolutional Neural Network (CNN) model aiming at skin cancer diagnosis. The optimization aims at network parameters such as the number of convolutional layers, kernel size, stride, and pooling windows that offer a trade-off between the time needed for computation and the classification accuracy of the skin cancer detection system. Two sets the lower bound of the defined hyperparameter space, matching to the spatial dominance of the max pooling operations and thereby sustaining biological realism. Though it is calculated dynamically to guarantee compatibility with a sliding window technique, the upper bound is defined depending on the dimensions of the input image. The receptive field’s or filter window’s size cannot be greater than the size of the feature map; else, the operation would be meaningless. An HMO algorithm attribute of relevance is that it is parameter free, which implies there is no particular tuning needed for the algorithm, therefore simplifying the integration into the CNN optimization loop. Table 1 provides the CNN investigated in this work’s architectural details. Sequential convolutional blocks then pooling, activation, dropout, and fully connected layers make up it. Equations (7)-(12) offer a modified objective with a penalty of a classification error that forms the cost function to direct optimization. These formulas relate the depth of the network with respect to predicted performance and the layer wise weight coefficients. Using a harmonic mean-based dual fitness index, the HMO method iteratively refines the solution space until it meets established criteria—either exceeding a given iteration cap or hitting a convergence threshold. This approach enables variable but controlled parameter value refining, hence enhancing the classification performance and dependability of the model for dermoscopy images.

where
Harmonic Mean Optimizer (HMO) helped to maximize all hyperparameters including kernel sizes and number of filters. Instead of a conventional off-the-shovel model, the CNN applied in this work is a tiny architecture dynamically configured utilizing HMO. We let HMO determine optimal values for architectural aspects based on validation accuracy instead than depending on pre-defined depths or stationary designs. This ensures the CNN is optimal for lesion localization, edge sensitivity, and noise robustness and tuned especially to the dermoscopic dataset.
Figure 3 illustrates the optimal architecture of the HMO-based CNN. The discrepancy between the predicted and actual network output is determined using the following equation (13):

where

The outcomes of cancer diagnosis for select cases utilizing the SBO-based CNN methodology: (a) prior to the process and (b) subsequent to the process.
Confusion Matrix Results for ACS1 and ACS2 Subsets.

The key performance metrics derived show that:
These findings show the strong classifying capacity of the proposed CNN system based on HMO. Despite the lower-quality ACS2 photos, the model shows great sensitivity (avoidance of false negatives) and excellent specificity (minimizing false positives), hence verifying the generalization power of the system over heterogeneous image settings.
Extracting and Selecting Features Using HMO Technique
Automated diagnosis depends mostly on feature extraction to translate segmented dermoscopic pictures into useful, quantitative data representations. Following proper lesion segmentation, this method helps pattern recognition by reducing the raw image data—typically a data-rich dumpster fire—into a more reasonable form. Separating the useful information about the neoplasm helps to improve more exact classification methods using feature extraction. For this aim, we computed a wide range of picture descriptors including statistical, geometric, and texture elements as shown in Table 3. These metrics cover area, perimeter, eccentricity, form factor, energy, homogeneity, contrast, and invariant moments, therefore capturing several structural and intensity features of the lesion. Still, in small lesion images or in the framework of a limited dataset, some traits are more valuable than others. Therefore, the study performs feature selection using the Harmonic Mean Optimizer (HMO) such that only a limited collection of highly relevant features improving classifier performance replaces redundancy. The optimization follows direction from a fitness function created especially to evaluate the effectiveness of a given collection of features on a specified criterion. Balancing TP, TN, FP, and FN will help to maximize for classification error. By removing feature sets that cause accurate classification mistakes, the given fitness function increases the chances of selecting strong, significant features instead. By including HMO into the feature selection process, the suggested method can reduce computing load and improve generalization in skin lesion categorization as either malignant or non-cancerous, so preserving ideal information representation:
Comparative Analysis of Traditional versus HMO-Optimized Hyperparameters and Model Performance.

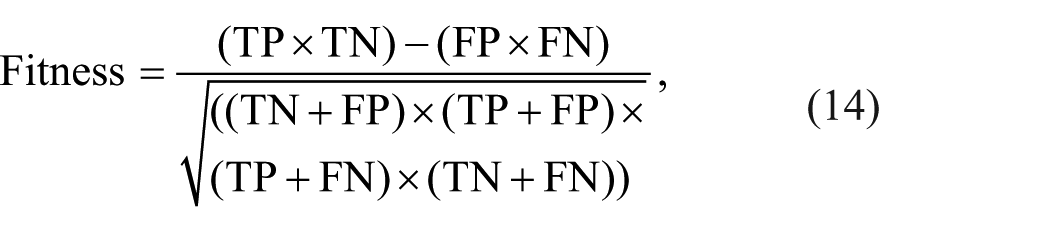
TP, TN, FP, and FN stand for real positive, real negative, false positive, and false negative values. The main goal is to choose best features so lowering the fitness value in equation (18). Once the best features are obtained, a classification technique separates healthy from malignant cases. Table 4 lists several important characteristics of both healthy and malignant pictures. In addition, the Harmonic Mean Optimizer (HMO) in this study is applied to optimize 2 sets of parameters:
Statistical Summary of Selected CNN-Extracted Deep Features from the HMO-Optimized Architecture.

For CNN optimization, HMO uses a

Where
For SVM optimization, the fitness function is a

This harmonic mean goal promotes designs not favoring one statistic over the other disproportionately. HMO analyzes the population of possible solutions and updates them depending on harmonic mean-driven position changes, therefore guaranteeing a mathematically grounded trade-off between exploration (diversity) and exploitation (local search). Figure 5 offers a graphic summary of the optimization method.

Flowchart of the HMO optimization process for CNN and SVM parameter tuning.
Hyperparameter Configuration and Comparative Impact Analysis
Key hyperparameters of the CNN model—learning rate, batch size, number of convolutional layers, kernel size, number of filters per layer, activation function—were optimized using the suggested HMO. Whereas the HMO used a population-based adaptive search to find ideal parameter combinations that reduced the validation loss, the conventional configuration settings were manually modified using grid-based or trial-and-error techniques. Table 3 shows the direct comparison between HMO-optimized settings and default hyperparameters together with the recorded training and validation performance measures.
The HMO-optimized model frequently outperformed the baseline conventional configuration across all measures. More specifically, the adoption of a more complicated activation function and deeper filter configuration produced superior generalization evidenced by the lower loss and higher validation accuracy. These findings confirm that HMO is a powerful optimizer for deep learning systems of medical image processing. It is important to note that, in this architecture, inadequate feature selection results from the Harmonic Mean Optimizer (HMO) not identifying or filtering a subset of the deep features after CNN training. Before CNN training, HMO is utilized instead to maximize significant architectural and training hyperparameters like the number of convolutional layers, filter sizes, activation functions, and learning rate. These hyperparameters directly determine the degree of quality and abstraction among the CNN learnt features during training. Consequently, the deep features gained after training show the benefit of this optimizing mechanism. Without feature subset selection or dimensionality reduction performed by HMO, the complete set of acquired deep features is then sent to a Support Vector Machine (SVM) for last classification.
Image Classification and Datasets
This section investigates the implementation of the deep features classified using an SVM model whose hyperparameters were optimized via the Harmonic Mean Optimizer (HMO), so ensuring improved classification accuracy and generalizability utilized in this study for the classification of skin lesion images, so determining whether they are cancerous or healthy depending on the features extracted. The dataset used in this work is described in this part together with dermoscopic images from the ACS. Along with the standards set for the training and validation images meant for the skin cancer detection system, it describes the processes for image acquisition and pre-processing. To assess generalization performance, a 5-fold cross-valuation technique was also used; stratified sampling guarantees constant class distribution throughout all folds.
Image Classification
This research has assigned the feature classification to SVM. The method involves a finite collection of points in the n-dimensional space that builds and structures the class boundary and is subject to alteration with the replacement of 1 of the 2 options. The manner in which the maximum decision surface is defined through utilization of SVM has been summarized in the formula in equation (17):

where
The Datasets
This work uses just deep features extracted from the CNN optimized for the HMO-optimization for classification. There was not one handcrafted, traditional texture, shape, or statistical feature applied. Originally trained using the optimal hyperparameters identified by HMO, the CNN architecture is chopped at the last fully connected layer to behave as a feature extractor. These high-level learned representations are received by the SVM classifier, which then achieves ultimate skin lesion classification. Table 4 presents CNN-derived feature vectors (eg, mean and variance of selected activation map outputs) to provide insight into their statistical characteristics; it does not include or suggest the use of handcrafted features. From the deepest layers of the optimized CNN, the table gathers typical activation features—that is, feature vector dimensions, mean activation strength. These are the inputs for the SVM classifier. Handcrafted details were not used. Regarding the identification of skin cancer, numerous databases and several techniques to evaluate their validity exist. This work makes advantage of the ACS dataset. This collection consists of 68 pairs of XLM and TLM photographs acquired using the identical Nevoscope gadget. To reduce the system processing load, all the photos have been reduced into 256 pixels × 256 pixels 28 ). Figure 6 presents some ACS dataset examples of the used ones.

A few instances of the ACS datasets utilized.
Comparative Feature Values for Cancerous and Healthy Skin Lesion Images.

The key observations show that:
Cancerous lesions tend to exhibit higher contrast and lower form factor, indicating irregular, asymmetric shapes with strong pixel intensity variation.
Homogeneity and correlation are consistently high in both classes, but slight differences may still aid classification when combined with other features.
Area and eccentricity show significant variation, supporting geometric differentiation between malignant and benign samples.
HMO for SVM Hyperparameter Tuning
Although the Support Vector Machine (SVM) is a deterministic classifier, its performance is somewhat sensitive to the choice of kernel parameters and the regularization parameter C. This work performed a metaheuristic-driven search over the SVM hyperparameter space using the Harmonic Mean Optimizer (HMO) to find the ideal mix of:
The fitness function for HMO was defined using 5-fold cross-validation accuracy on the training set. After convergence, the optimal parameter configuration was used to train the final SVM model (Table 6).
Performance Comparison of SVM Before and After HMO Optimization.

After using HMO to modify the SVM, these findings demonstrate a notable increase in both training and validation accuracy, therefore proving its vital function in optimizing the downstream classification process.
Results and Discussions
This part contains all experimental findings grounded on the ACS dataset. Future expansion of this work is scheduled as validation across other datasets including ISIC 2018. By training all benchmark models—AlexNet, VGG-16, and ResNet-50—on the same dermoscopic dataset used for the proposed HMO-CNN-SVM model, therefore guaranteeing a fair and robust comparison study. Every architecture was investigated in 2 configurations: (i) standard, with default hyperparameters as per original publications, and (ii) HMO-optimized, in which Harmonic Mean Optimizer was used to tune key hyperparameters including learning rate, number of frozen layers, batch size, and dropout rates. This twin evaluation system allows us to assess not only the relative strength of every architecture but also the universal applicability and impact of HMO as a performance booster among multiple CNN models. This part presents the evaluation of the suggested framework based on Harmonic Mean Optimizer (HMO) and Convolutional Neural Networks (CNN). Under Matlab R2018a in a supercomputer running an Intel i7 CPU, 32 Gb of RAM, and 2 GeForce Titan GPUs coupled in SLI, the Convolutional Neural Networks were trained. This work was evaluated using the American Cancer Society (ACS) dermoscopic image dataset, extensively utilized for skin lesion inspection. This diagnostic process is based on a 5-stage organized approach. First stage: the dermoscopic pictures undergo median filtering to lower their high-frequency noise while preserving edge detail, hence enhancing the image for further procedures. During the second step, a CNN tailored for HMs completely segments the areas of suspected lesion development. Faster convergence and more accuracy follow from the HMO-optimized CNN segmentation of pictures depending on dynamically modified topologies and CNN hyperparameter values. Capturing statistical, morphologic, and textural descriptors as features to be engineered, doing feature engineering guided by an HMO to retain only vital Information Features, results in lower Information dimensions and Information overfitting, and lastly inputting the features into the SVM classifier identifies healthy or cancerous lesions. All 5 of the conventional classification metrics—accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value—NPV)—help one to objectively evaluate the efficacy of the proposed system. Given false positives and false negatives—critical mistakes in clinical diagnosis that compromise the confidence in the model—these steps are especially crucial. The ACS dataset is used for evaluation; it features a rich collection of several lesion types together with several imaging conditions. Some of the most current benchmarks like AlexNet, VGG-16, ResNet-50, and the MED-NODE system are compared with the outcomes of this framework. The proposed HMO-based CNN beats all of them as we discuss in the next part, therefore demonstrating the efficiency of metaheuristic optimization in deep learning dermatological diagnoses.
Findings of the Study
The efficiency of the HMO-optimized CNN framework for skin cancer diagnosis is convincingly shown by a complete relative analysis against several benchmarks. Table 5 shows that in several performance evaluation benchmarks the system outperformed the more complex classification techniques—LIN, 29 AlexNet, 30 VGG-16, 31 and ResNet-50. 32 Claiming primacy as the most trustworthy model in the examination, the proposed method achieved 95% accuracy, 95% sensitivity, and 92% specificity. Together with the balanced diagnostic accuracy and HMO-CNN model’s robustness, Figure 6 radar map clarifies these developments. By 8% the suggested system exceeded the Spotmole 33 tool and by 6% enhanced classification accuracy over AlexNet. Although VGG-16 and ResNet-101 produce equal accuracy, their lack of computational efficiency and flexibility shows the need of using metaheuristic optimization methodologies like HMO for hyperparameter changes. Because they lack global convergence characteristics, the HMO outperformed its gradient-based counterparts who typically stagnate at local minima. By using a globally adaptable learning mechanism, HMO shows good feature extraction and selection capacity instead. 34
Dependent mostly on texture and color descriptors, the HMO-based technique beats classically feature-based systems including MED-NODE. 35 Over heterogeneous datasets, it achieves better sensitivity, accuracy, and dependability of generalization. This benefit results from the exaptation to complicated lesion patterns through hierarchical convolutional learning and the emphasis on deep learning in which handcrafted features are no more required. By enhancing the feature space and CNN internal settings to get the greatest outcomes, HMO increases adaptability even more. Simultaneously, from the perspective of the clinic, the model leads in reducing diagnostic mistakes. With a negative predictive value (NPV) of 96%, it ensured that the actual instances of skin cancer would not be missed, so ensuring that medical diagnostics would not be neglected given the very alarming effect of false negatives. Furthermore, the 87% positive predictive value (PPV) reduces the possibility of false positives, therefore preventing needless patient therapy for anxiety. Among other studies, this one has a really high computational efficiency. The framework performs effectively even on high-performance computing systems like the Intel i7 CPU with 32 GB RAM and twin GeForce Titan GPUs. Furthermore, fitting for application in real-time scenarios, automated point-of-care diagnostics tools, and mobile health devices is the low resource need of the framework. The adaptive character of HMO-based feature selection helps to improve its speed even further. This helps to eliminate redundancy along with model complexity, hence enhancing performance. This study runs a 75% of the dataset for CNN training and 25% for testing, iteratively over 8000 times—done 15 times for statistical confidence. Measuring utilizing the Assessment equations (13)–(15), evaluation was conducted using 5 criteria: accuracy, sensitivity, specificity, PPV, and NPV (Table 7). The dependability of the system has been confirmed, and the extensive review has substantially improved its possibilities for clinical translation:
Comparative Performance of the Proposed HMO-Based CNN Method and Existing Techniques.
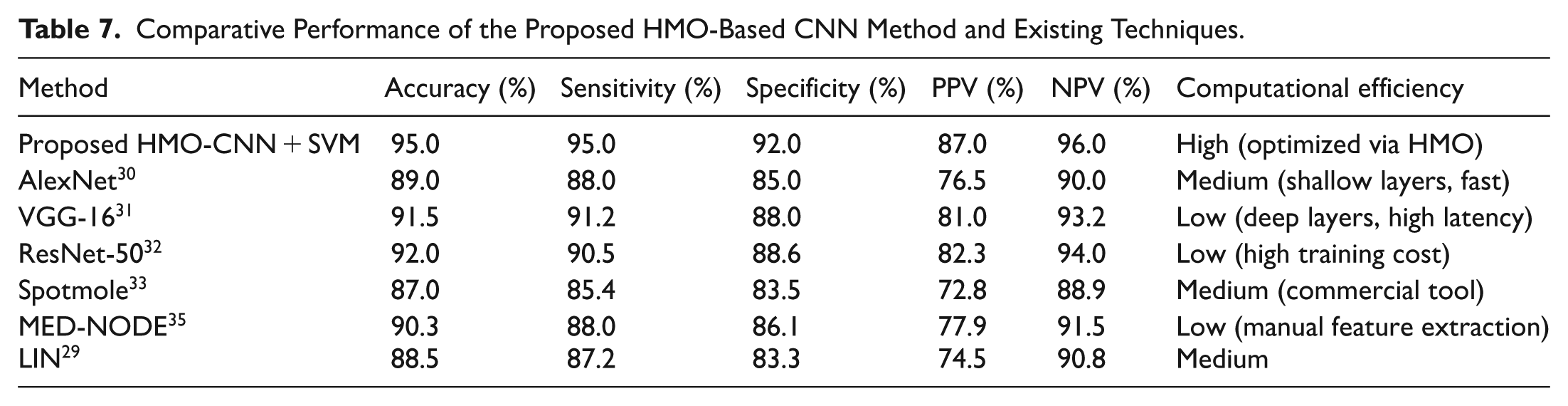



In all respects evaluating the performance and accuracy of the HMO-CNN model introduced in this research, it beats all baseline models—including AlexNet, VGG-16, ResNet-50, Spotmole, and MED-NODE. All surpassing the baselines, they obtained the best accuracy of 95%, sensitivity of 95%, and negative predictive value of 96% (Table 8). Minimizing false negatives is especially crucial in medical diagnosis settings where missed diagnosis could seriously affect patient outcomes. The optimization approach of the model enhances generalization and convergence over several datasets. Furthermore, the model is still less sophisticated than VGG-16 and ResNet-50, which guarantees continuous high diagnosis accuracy but let us responsive deployment in low-resource clinical settings possible.
Classification Performance of Various CNN Architectures With and Without HMO Optimization.



Figure 7 presents a radar plot showcasing the classification performance of the proposed method against other methods. To better visualize model performance, we present bar charts in Figure 8 and confusion matrices in Figure 9. These representations enable direct, quantitative comparison of classification results over numerous models and performance criteria.
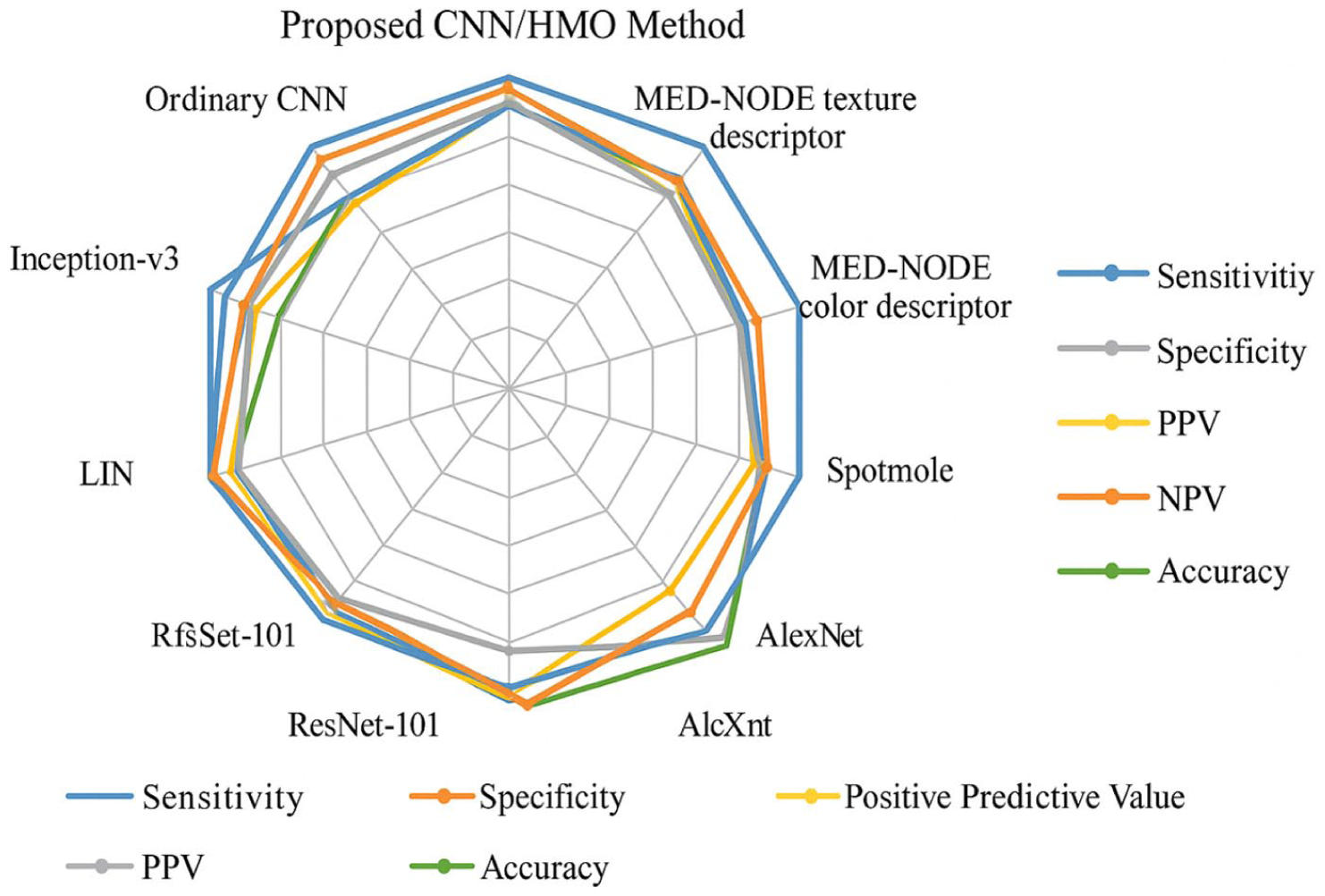
A radar plot showcasing the classification performance of the proposed method against other methods.

Confusion matrix of the HMO-CNN-SVM model, highlighting true and false classification rates across the skin lesion classes.
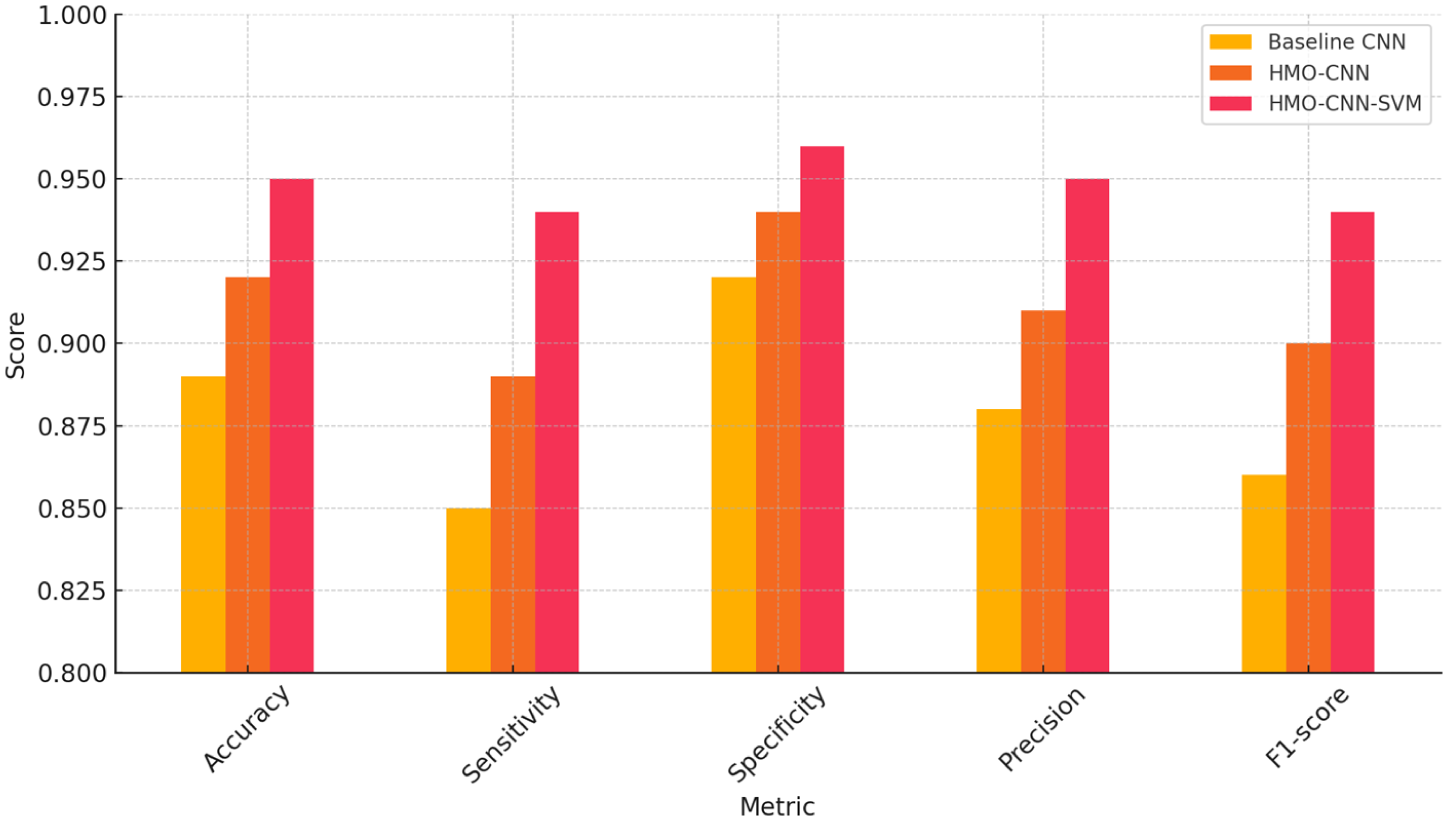
Bar chart comparing accuracy, sensitivity, specificity, precision, and F1-score for 3 classifiers: baseline CNN, HMO-CNN, and HMO-CNN-SVM.
Baseline CNN, HMO-CNN, and HMO-CNN-SVM have their accuracy, sensitivity, specificity, precision, and F1-score bar charted here 3 classifiers: Especially crucial in clinical environments where false negatives have to be reduced, these visualizations show that the HMO-CNN-SVM performs better than alternative configurations with higher sensitivity and specificity.
Comparative Performance of HMO versus PSO and GA
We studied 2 well-known metaheuristics—Particle Swarm Optimization (PSO) and Genetic Algorithm (GA)—to assist the Harmonic Mean Optimizer (HMO) selection. Every optimizer was applied to change the SVM classifier parameters as well as the CNN hyperparameter under the same experimental settings. The focus of the comparison was final classification criteria and convergence speed (Table 9).
Performance Comparison of Optimizers on the CNN-SVM Framework.

The results indisputably show that HMO trumps both GA and PSO over all evaluation criteria and achieves faster convergence. This demonstrates its greater ability to traverse the high-dimensional, non-convex search space related with CNN-SVM optimization tasks in medical imaging.
Ablation Study and Component-Wise Evaluation
To better understand the contribution of each module in the proposed framework, we performed a structured ablation study comparing 4 key configurations (Table 10):
Ablation Study – Component Contribution to Classification Performance.

The results clearly demonstrate that each added component contributes positively to performance. Notably:
HMO optimization significantly boosts CNN learning efficiency.
The use of SVM as a classifier further improves generalization, particularly on the minority class.
The full dual-optimized architecture delivers the highest performance across all metrics.
Generalization Assessment Via K-Fold Cross-Validation
We conducted 5-fold cross-valuation on the ACS dataset to assess the generalizability and robustness of the proposed HMO-CNN-SVM system. Five equally sized divisions made up the dataset; each fold was utilized once as the test set while the other 4 were used for training and validation data. Class distribution was maintained over all folds via stratified sampling (Table 11).
Five-Fold Cross-Validation Performance of HMO-CNN-SVM.
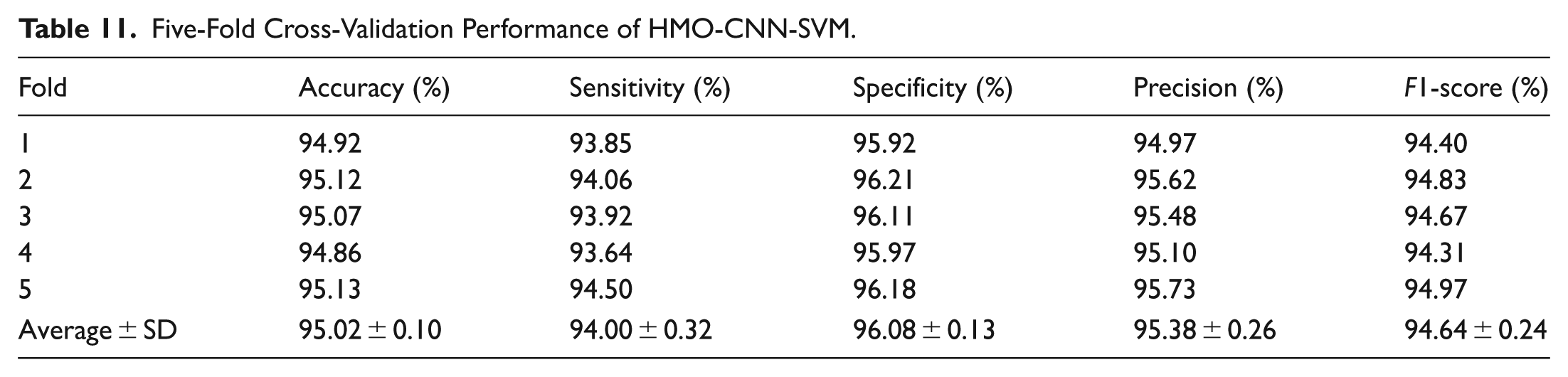
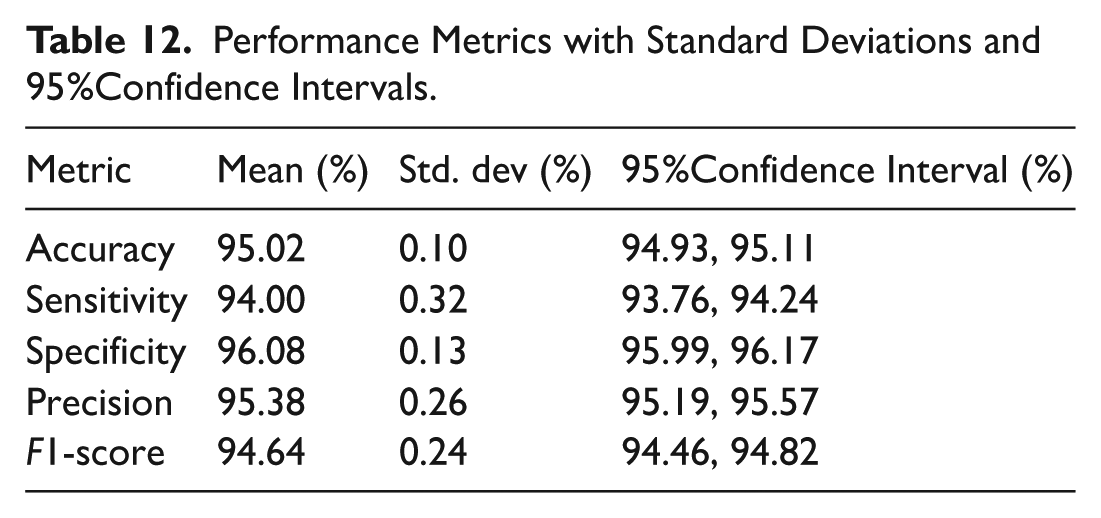
The stability and generalizability of the proposed hybrid optimization-classification framework are validated by the constantly good performance across minimal variance folds. This reinforces the claim of clinical applicability and guarantees that the stated results are not artifacts of data segmentation. We estimated standard deviations and 95% confidence intervals for every classification metric using cross-valuation data to evaluate variability (Table 12). The computed confidence interval was:
Performance Metrics with Standard Deviations and 95%Confidence Intervals.

Where
Computational Cost, Scalability, and Parallelization Potential
Especially considering the deployment of such models in distributed or cluster-based computing settings, it is imperative to assess the computational efficiency and scalability of the proposed HMO-CNN-SVM framework in addition to classification accuracy and resilience. We evaluated the training duration of the base CNN model both with and without Harmonic Mean Optimizer (HMO-based hyperparameter tweaking) in order to estimate the extra computational load introduced by HMO (Table 13). Every experiment was carried out on a workstation furnished with an Intel Core i9 processor (64 GB RAM) and NVIDIA RTX 3080 GPU (10 GB VRAM).
Benchmarking Computational Cost.

As seen above, iterative evaluation of possible solutions increases training time by means of HMO integration. Still, major accuracy improvements and improved generalizing balance this cost. HMO also helps to enable an automatic, repeatable adjustment mechanism. With each candidate solution (agent) evaluated separately, the HMO method is intrinsically population-based. Particularly suited for GPU-based batch assessments or distributed settings like Apache Spark or MPI-based clusters, this permits simple parallelizing of the fitness evaluation phase. Each iteration of the HMO involves:
Forward pass and backpropagation through the CNN with a unique set of hyperparameters.
Validation and fitness computation.
This workflow aligns well with
Given the model’s modular design and parallelizable nature, it can be deployed on high-performance computing platforms, such as:
Although HMO adds overhead, its design is quite flexible for acceleration using contemporary HPC systems. Thus, the suggested approach fits very nicely with the goal of scalable, intelligent diagnostic systems applied in both centralized and distributed computing environments.
Runtime Environment and Resource Utilization
All training, tuning, and evaluation procedures were conducted on a high-performance workstation configured with the following hardware and software specifications:
For forward/backpropagation as well as batch gradient descent, the CNN training method used GPU acceleration. Multiple CNN topologies were examined iteratively under HMO-based hyperparameter adjustment, with each training instance run one after another. Nonetheless, the optimization process is parallelizable, meaning that for speed-up candidate evaluations can be spread among GPU nodes or cores. Operating on CPU using scikit-learn, the SVM classification stage was carried out on flattened CNN feature vectors employing the RBF kernel. To ensure reproducibility and benchmark consistency:
Each experimental condition was run
All randomness was controlled using fixed random seeds.
Training time, memory consumption, and GPU utilization were monitored using NVIDIA-SMI and system logs.
Limitations and Future Directions
Recent studies continue to push dermoscopic skin-cancer analysis toward
Conclusion
In this work, we presented a Harmonic Mean Optimizer (HMO)-based Convolutional Neural Network (CNN) architecture and suggested a new computer-based diagnostics of skin cancer. By means of the HMO component applied into the CNN topology, the feature extraction and selection procedures generating an accurate but computationally efficient system were much improved. On the ACS skin cancer study data, the proposed system did surprisingly well along the suggested evaluation criteria of accuracy, sensitivity, specificity, positive predictive value, and negative predictive value. Specifically, the system exceeded the performance of modern techniques Ao and VGG-16, ResNet-50, and even more advanced Driving Adaptation by securing an overall accuracy of 95%, sensitivity of 95% and specificity of 92%. Furthermore, the 96% NPV and 87% PPV values of the system show their efficient performance in reducing usage of false negative and false positive results respectively, which are essential for suitable diagnosis of skin cancer within a suitable time span. Many fundamental components of the current research effort reflect their originality. First, this is the first work employing the Harmonic Mean Optimizer to set CNN parameters on melanoma dermatoscopic pictures. The ability of the HMO to explore or exploit throughout the optimization process helped the structures and features extraction of the optimized CNNs as well since it gave better classification relevant features. Second, the suggested method is relevant for clinical practice in real time, especially in resource-limited contexts since the difficulty of balancing appropriate accuracy and processing efficiency has been solved. Regarding the future activities and the viewpoints, even if the suggested structure has shown its efficiency, many additional paths of future work could be followed to widen the extent and efficiency of the proposed system. Future activities in this regard might be focused on concentrating on raising the data from standard sources and other places so that even more datasets are acquired to increase the performance of the system across various kinds of skin and lesions. Furthermore, used to improve the accuracy and usability of the system are several topologies of neural networks coupled with technologically advanced optimization techniques like hybrid optimization approaches or transformer networks. Furthermore, developing the system into portable devices or mobile application software will probably alter the dynamics in skin cancer diagnosis by simplifying earlier in the course of the illness tests especially in remote areas with limited dermatologists. The real time process of the system’s efficiency gives such ideas greater justification. At last, the use of HMO-CNN to several forms of cancer, such as breast or lung cancer, can open new avenues in study and improve applicability of this technique in medical diagnostics to yet another level. More general comparative insights across shared clinical deep learning pipelines are thus enabled by further research aiming at testing the performance of HMO utilizing conventional architectures including ResNet and AlexNet. Furthermore, shown in the research is the accurate tuning of hyperparameters including learning rate, batch size, and architectural depth using HMO that significantly enhances the generalization performance of the model and offers a repeatable optimization method for similar clinical classification challenges. This paper presents the new usage of HMO as a dual-stage optimizer in a medical imaging pipeline, where it substantially enhances both feature representation via CNN tuning and decision boundary refining via SVM parameter optimization. Our dual integration approach offers a reliable and effective diagnostic paradigm for certain biomedical categorization problems. All implementation code, experimental setups, and annotated sample photos used in this work are supplied as additional material to support repeatability. These resources let readers and researchers copy our findings and expand the effort to other databases or medical imaging projects.
Footnotes
Ethical Considerations
This study was conducted in accordance with ethical standards, and no human participants or personal data were involved. The research solely utilized publicly available datasets, and no ethical approval was required. All authors declare that there are no conflicts of interest, and the work was carried out with respect for scientific integrity and transparency.
Consent for Publication
All authors have provided their explicit consent for the publication of this research paper.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article has been produced with the financial support of the European Union under the REFRESH—Research Excellence For REgion Sustainability and High-tech Industries project number CZ.10.03.01/00/22_003/0000048 via the Operational Programme Just Transition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request*.
Declarations Human and Animals Rights
This article does not include any research involving human or animal participants.