
Abstract
Objectives
Artificial intelligence (AI)-driven automated crown design is rapidly transforming digital restorative dentistry by enabling anatomically precise and functionally integrated crowns. This systematic review and meta-analysis critically evaluate whether AI-assisted crown design systems, including machine learning (ML), deep learning (DL), generative adversarial networks (GANs), and diffusion models, produce restorations with comparable or superior morphological accuracy, occlusal integration, internal fit, and workflow efficiency relative to computer-aided design (CAD) or technician-driven workflows.
Methods
A comprehensive search of MEDLINE (PubMed), Scopus, Web of Science, Embase, and Cochrane Library was conducted for studies published through 17 March 2026. Eligible studies included in vitro, in silico, and clinical investigations comparing AI-based crown design systems with conventional workflows. Primary outcomes were morphological accuracy root-mean-square (RMS) deviation, cusp morphology, volumetric/linear deviation, occlusal contact fidelity, and internal fit; secondary outcomes included marginal adaptation and restoration design time. Risk of bias was assessed using validated tools, and meta-analyses were conducted using random-effects models with standardized mean differences (SMDs).
Results
Seventeen studies met the inclusion criteria, of which 13 were included in the quantitative synthesis. AI-based systems achieved clinically acceptable morphological accuracy, internal fit, and occlusal contact reproduction (RMS deviation: SMD = −0.15, 95% CI −1.04 to 0.74). Workflow efficiency improved significantly, with reductions in design time of 25-50% and enhanced precision in chamfer and marginal gaps (p < 0.001). DL and GAN-based platforms consistently produced crowns within clinically acceptable deviation ranges (<100–200 μm). Integration of patient-specific occlusal and mandibular dynamics further enhanced functional occlusal prediction. Expert technician refinement remained beneficial in anatomically complex cases.
Conclusions
AI-assisted crown design demonstrates promising potential for providing reproducible, morphologically accurate, and functionally integrated restorations while potentially enhancing workflow efficiency. This review underscores the potential of AI systems to standardize restorative outcomes and reduce operator dependency, while combined human-AI workflows may enhance performance in complex cases. However, the current evidence is derived predominantly from in vitro and computational studies, with limited prospective clinical validation, limited integration of patient-specific dynamic occlusal data, and insufficient long-term follow-up evidence. Therefore, the findings should be interpreted cautiously and not considered definitive evidence of clinical superiority over conventional workflows. Standardized clinical protocols and prospective trials are required to confirm long-term efficacy.
Keywords
1. Introduction
The precise reconstruction of dental crown morphology remains a fundamental challenge in restorative dentistry. Clinically successful restorations must not only replicate the intricate anatomical features of natural teeth but also maintain accurate occlusal relationships with adjacent and opposing dentition, while accommodating patient-specific mandibular movements and functional occlusal pathways. Inaccurate replication of these features can lead to premature contacts, uneven load distribution, increased biomechanical stress, restoration fracture, temporomandibular dysfunction, and patient discomfort. 1
Digital dentistry has revolutionized restorative workflows by integrating intraoral scanning, computer-aided design (CAD), and computer-aided manufacturing (CAM) technologies into end-to-end protocols. These digital systems enable highly accurate three-dimensional representations of prepared abutments and support precise model fabrication, substantially reducing turnaround time, operator dependency, and human error compared with conventional analog techniques. 2 However, despite these advances, conventional CAD-based crown design remains limited by reliance on library-based morphology, average anatomical parameters, and manual refinement, which may not fully reflect individualized functional occlusion or patient-specific dynamics. Consequently, variability in clinical outcomes persists, and design workflows may remain time-consuming. 3
Artificial intelligence (AI) offers transformative potential in this domain. Machine learning (ML) and deep learning (DL) algorithms can analyze large datasets of dental morphology to identify complex anatomical patterns and functional relationships, generating highly detailed restorative designs directly from digital scans. Advanced DL architectures, including generative adversarial networks (GANs) and diffusion-based models, are increasingly applied to predict occlusal surfaces, cusp geometry, and tooth morphology with high anatomical fidelity, while minimizing operator dependency. 4 Contemporary AI-assisted crown design platforms, such as Dentbird Crown (Imagoworks Inc., Seoul, Republic of Korea), AutoMate (3Shape A/S, Copenhagen, Denmark), PrintIn DentDesign (PrintIn, Taoyuan, Taiwan), and CEREC Biogeneric (Dentsply Sirona, Charlotte, USA), automate restoration morphology generation to standardize design quality, reduce workflow time, and minimize variability.3,5,6
Recent innovations extend AI applications beyond static morphology, incorporating patient-specific occlusal and mandibular dynamics derived from jaw-tracking devices, digital occlusal analysis, or motion-capture-based kinematics. These systems aim to optimize functional occlusal contacts and reduce post-placement chairside adjustments, potentially improving clinical efficiency and patient outcomes, where personalized parameters influence the prosthetic design achieving unique restorations to each patient’s specific mandibular movements.7,8 Nevertheless, limitations remain in reproducing nuanced functional wear facets, cusp-groove morphology, and consistent performance in anatomically complex cases. Moreover, the current literature is fragmented, with heterogeneous datasets, diverse algorithmic architectures, and inconsistent evaluation protocols, complicating direct comparisons between AI-based and conventional workflows.2,9
Therefore, this systematic review and meta-analysis critically evaluates the performance of AI-based automated crown design systems relative to conventional CAD and technician-driven workflows. The analysis focuses on morphological accuracy, occlusal integration, internal fit, and workflow efficiency, with particular attention to the added value of integrating patient-specific functional dynamics. The null hypothesis is that no statistically significant differences exist between AI-generated and conventional CAD or technician-driven crown design workflows in terms of morphological accuracy (e.g., RMS deviation, volumetric and linear discrepancies, cusp morphology), occlusal contact fidelity, internal fit, marginal adaptation, occlusal morphology, chamfer/finish line precision, and workflow efficiency (design time).
2. Materials and Methods
2.1 Study Design
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. 10 The protocol was prospectively registered in the Open Science Framework (OSF; 10.17605/OSF.IO/YG6D2). The research question was formulated using the PICO framework, in which the population comprised digital datasets of teeth requiring crown restoration, including clinical cases, typodont models, and digital dental casts representing both anterior and posterior dentition. The intervention included AI-based automated crown design systems, encompassing ML, DL, GANs, diffusion-based architectures, and hybrid or knowledge-based approaches, with particular emphasis on systems integrating patient-specific occlusal or mandibular dynamic data. The comparator consisted of conventional crown design workflows, including technician-driven design, manual CAD modeling, library-based CAD/CAM morphology, and virtual articulator-based simulations. The primary outcomes were defined as morphological accuracy, measured by root-mean-square (RMS) surface deviation, occlusal contact accuracy, cusp-groove morphology, and internal fit. Secondary outcomes included marginal adaptation, restoration design time, and functional occlusal performance.
The focused research question was whether AI-based automated or generative crown design systems, particularly those incorporating patient-specific occlusal dynamics, produce restorations with comparable or superior morphological accuracy, functional integration, and workflow efficiency relative to conventional CAD or technician-driven workflows.
2.2 Search Strategy
Search Strategy (PubMed Example)
2.3 Study Selection
Two independent reviewers (A.A.H. and M.N) screened all retrieved titles and abstracts. Studies were considered eligible if they met the following criteria: (1) in vitro, in silico, or clinical investigations evaluating AI-based dental crown design systems; (2) compared AI-generated crowns with conventional CAD workflows or technician-driven designs; (3) reported quantitative morphological, occlusal, or functional outcomes, such as RMS deviation, occlusal contact accuracy, cusp morphology, or internal fit; and (4) assessed outcomes related to crown morphology, occlusal integration, marginal adaptation, or restoration design efficiency. Exclusion criteria included non-English publications, review articles, case reports, animal studies, and conference abstracts without full data; studies lacking comparator groups; studies that did not report quantitative evaluation metrics; and investigations focusing solely on virtual articulator parameters without AI-based crown design generation. Full-text articles of potentially relevant studies were retrieved and independently assessed by the same reviewers. Discrepancies between reviewers were resolved through discussion, and, when necessary, consultation with a third reviewer was undertaken to reach consensus.
2.4 Data Extraction
Data were independently extracted using a standardized data collection form. Extracted information included the author and publication year, AI system or software evaluated (ML, DL, GAN, diffusion, hybrid), and study design, including dataset type and sample size. Detailed information regarding dataset characteristics and experimental setup was recorded, including tooth type, arch location, and whether the data were derived from in vitro models, digital casts, or clinical intraoral scans. The type of occlusal integration was documented, distinguishing between static occlusion (e.g., intercuspal position) and dynamic occlusal simulation (e.g., mandibular movement or articulator-based analysis). Comparator workflows were also extracted, including technician-designed crowns, conventional CAD systems, or natural tooth references where applicable. Outcome measures were comprehensively collected and categorized into morphological, functional, and mechanical parameters. These included RMS surface deviation, volumetric and linear discrepancies, cusp angles, occlusal contact points and contact area, internal fit, marginal gap, finish line deviation, and occlusal or proximal contact accuracy. Where reported, advanced geometric parameters such as Hausdorff distance and Intersection-over-Union (IoU) were also recorded. Functional and mechanical outcomes, including fracture resistance, stress distribution, and fatigue performance, were extracted when available. In addition, details of validation methodologies were documented, including three-dimensional superimposition techniques, finite element analysis, mechanical testing, blinded assessment, and statistical analysis approaches. The principal findings and conclusions of each study were also recorded to facilitate qualitative synthesis and comparison across studies.
2.5 Quality Assessment
The risk of bias in the included studies was evaluated using a study-design–adapted framework to ensure methodological appropriateness across heterogeneous experimental and computational designs. For in vitro experimental studies, the Quality Assessment Tool for in vitro studies (ROBDEMat tool) 11 was applied, which assesses four domains: D1 – planning and allocation; D2 – sample/specimen preparation; D3 – outcome assessment; and D4 – data analysis and reporting. Domain D1 includes three criteria: the use of appropriate control or reference groups, randomization of samples, and justification of sample size. Domains D2, D3, and D4 each comprise two criteria: D2 evaluates the standardization of experimental methods and conditions; D3 assesses study reproducibility and the implementation of operator blinding; and D4 examines the appropriateness of statistical analyses and transparency of outcome reporting. Each criterion was rated as “sufficiently reported,” “insufficiently reported,” “not reported,” or “not applicable.” In addition, for non-randomized clinical studies, risk of bias was additionally interpreted using ROBINS-I principles, 12 focusing on confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, outcome measurement, and selective reporting. For diagnostic or measurement-accuracy–oriented studies, risk of bias was evaluated in line with Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) domains, 13 including patient selection, index test, reference standard, and flow and timing, with explicit consideration of applicability concerns. Quality assessment was independently performed by two reviewers, and any disagreements were resolved through discussion or, if necessary, consultation with a third reviewer until consensus was achieved. Studies were categorized as having low, moderate, or high risk of bias based on the overall reporting across domains. A study was considered at low risk of bias when most criteria were sufficiently reported without critical limitations, at moderate risk when one or more domains were insufficiently reported without major methodological flaws, and at high risk when multiple key domains were inadequately reported or not reported, potentially compromising the validity of the findings.
2.6 Data Synthesis and Statistical Analysis
Quantitative synthesis and meta-analyses were performed using Review Manager Software (version 5.4, The Cochrane Collaboration, Copenhagen, Denmark). A random-effects model was applied to account for inter-study variability. Pooled effect sizes were calculated as standardized mean differences (SMDs) for continuous outcomes, comparing AI-generated restorations with conventional CAD or technician-driven designs across relevant metrics, including morphological deviation (RMS), occlusal contact accuracy, internal fit, and cusp–groove morphology. Subgroup analyses were performed according to AI architecture (e.g., knowledge-based, deep learning, GAN, hybrid), occlusal integration type (static vs dynamic), and restoration location (anterior vs posterior teeth). Statistical significance was defined as p < 0.05. Heterogeneity among studies was assessed using the Cochran Q test and quantified with the I2 statistic to determine the degree of inconsistency across results. Quantitative pooling was performed only for outcomes meeting the following prespecified criteria: (1) reported in at least three included studies; (2) defined using comparable measurement methods and units across studies; (3) consistent effect direction interpretable as favorable vs unfavorable; and (4) extractable means and standard deviations (or data permitting calculation thereof). Outcomes that did not satisfy these criteria were synthesized narratively.
3. Results
3.1. Search Strategy
A systematic and comprehensive search was conducted across multiple electronic databases, initially yielding 689 records. After removal of duplicates, 532 unique publications were retained for preliminary screening. Titles and abstracts were then evaluated, resulting in the exclusion of 456 studies that did not meet the predefined inclusion criteria, such as non-AI workflows, non-occlusal crown focus, or insufficient methodological detail. Full-text assessment was performed on the remaining 76 articles. Of these, 59 studies were excluded due to reasons including lack of quantitative outcome reporting, ineligible AI methodology, or insufficient occlusal evaluation: CAD/CAM or 3D printed restorations without AI modality (n=23), inaccessible full texts (n=15), AI descriptive studies (n=4), studies implementing virtual articulators (n=5), studies using intraoral scanners without AI modality (n=4), out of study inclusion criteria (n=8). Ultimately, 17 studies were included in the qualitative synthesis. Among these, 4 studies were excluded from quantitative comparison due to heterogeneity in performance metrics, leaving 13 studies for further comparative analysis. A detailed overview of the study selection process is provided in the PRISMA flowchart (Figure 1). PRISMA flowchart summarizing the study selection process
3.2. Main Findings
Summary of AI-Assisted Occlusal Crown Design Studies: Systems, Methodologies, and Key Findings
Abbreviations: AI, Artificial Intelligence; AA, Automated Algorithm; AD, Automated Design; BI, Built-In Knowledge-Based AI; CAD, Computer-Aided Design; CE, Clinician Expert; CN, Clinician Novice; DL, Deep Learning; DM, Dental Technician–Optimized Model; FDI, Fédération Dentaire Internationale clinical quality score; GAN, Generative Adversarial Network; ICP, Intercuspal Position; IoU, Intersection over Union; NC, Conventional CAD; PMMA, Polymethyl Methacrylate; RMS, Root-Mean-Square; SD, Standard Deviation; TD, Technician-Designed; 3D, Three-Dimensional.
Occlusal integration strategies varied across studies, from static inter-occlusal contact assessments and virtual articulator simulations to dynamic occlusion modeling and triple-scan techniques.6,8,15,16 Functional performance metrics included RMS deviations, cusp angle analysis, occlusal contact points and areas, occlusal morphology, finish line deviation, marginal gaps, and stress distribution under simulated loading conditions.14,15,19,22,24 Workflow efficiency, measured as design time reduction, and clinical quality scores (e.g., Fédération Dentaire Internationale FDI) were also frequently reported.7,19,21 Overall, AI-generated crowns demonstrated high reproducibility and clinically acceptable fit, particularly in internal adaptation and occlusal contact alignment.6,18,19,23Knowledge-based AI systems often required manual refinement by technicians to achieve morphological conformity comparable to human-designed crowns, whereas DL and GAN-based models exhibited improved baseline morphology and faster design workflows.4,16,19 Certain studies reported subtle deviations in cusp angles, occlusal wear facets, or proximal contacts, highlighting that AI remains an adjunct rather than a replacement for skilled operator refinement.9,14,16,19
Several investigations demonstrated enhanced efficiency, with AI workflows reducing design time by approximately 25-50% compared with conventional methods, without compromising clinically relevant outcomes.19,21 Biomechanical and functional simulations suggested that AI-designed crowns maintained adequate stress distribution and fatigue resistance, although minor differences were observed depending on the algorithm type and the extent of technician optimization.15,22
Despite promising results, substantial heterogeneity in AI architectures, training datasets, occlusal integration protocols, evaluation metrics, and study designs limited the feasibility of quantitative meta-analysis. Narrative synthesis indicates that no single AI system universally outperforms conventional CAD workflows, but AI can reliably provide baseline designs with high reproducibility, reduced workflow time, and acceptable occlusal and marginal fit. Optimal outcomes typically involve combined AI-assisted design with targeted human refinement, particularly for complex occlusal geometries, aesthetic anterior teeth, or patient-specific functional requirements.8,16,19,23
3.3. Quality Assessment and Risk of Bias
Risk of Bias Assessment of Included in vitro Studies Using the ROBDEMat Tool. R – Sufficiently Reported/Adequate; NR – Not Reported; IR – Insufficiently Reported; and NA – Not Applicable

The non-randomized clinical study by Win et al., 6 assessed using ROBINS-I, demonstrated an overall low risk of bias across all domains. The within-subject design effectively controlled for confounding by allowing direct comparison under identical clinical conditions, with robust participant selection, intervention classification, outcome assessment, and reporting, and no evidence of missing data, protocol deviations, or selective reporting. Two studies (Chau et al. 17 ; Zhao et al. 24 ) were evaluated using QUADAS-2 due to their diagnostic and measurement-accuracy focus. Chau et al. 17 showed low risk of bias in the index test, reference standard, and flow/timing domains, but moderate risk in patient selection and applicability due to restrictive inclusion criteria and simulated conditions limiting clinical generalizability. In contrast, Zhao et al. 24 demonstrated consistently low risk of bias across all QUADAS-2 domains, supported by strong dataset design, independent validation, blinded assessment, and appropriate reference standards.
3.4. Meta-Analysis
A meta-analysis was conducted for outcomes meeting the prespecified suitability criteria. Accordingly, quantitative pooling was performed for RMS deviation, cusp angles, occlusal contact points, profile discrepancy, internal fit, chamfer distance, marginal gap, design time, and occlusal morphology. Outcomes with insufficient data or excessive methodological heterogeneity, including fracture resistance, stress distribution, FDI clinical quality scores, Hausdorff distance, and IoU, were synthesized narratively (Section 3.2 and Table 2) (Figures 2-10). Forest plot comparing AI-based and control systems for overall accuracy (RMS deviation) Forest plot comparing AI-based and control systems for cusp angle reproduction Forest plot comparing AI-based and control systems for occlusal contact points Forest plot comparing AI-based and control systems for profile discrepancy Forest plot comparing AI-based and control systems for internal fit Forest plot comparing AI-based and control systems for chamfer distance Forest plot comparing AI-based and control systems for marginal gap Forest plot comparing AI-based and control systems for design time Forest plot comparing AI-based and control systems for occlusal morphology

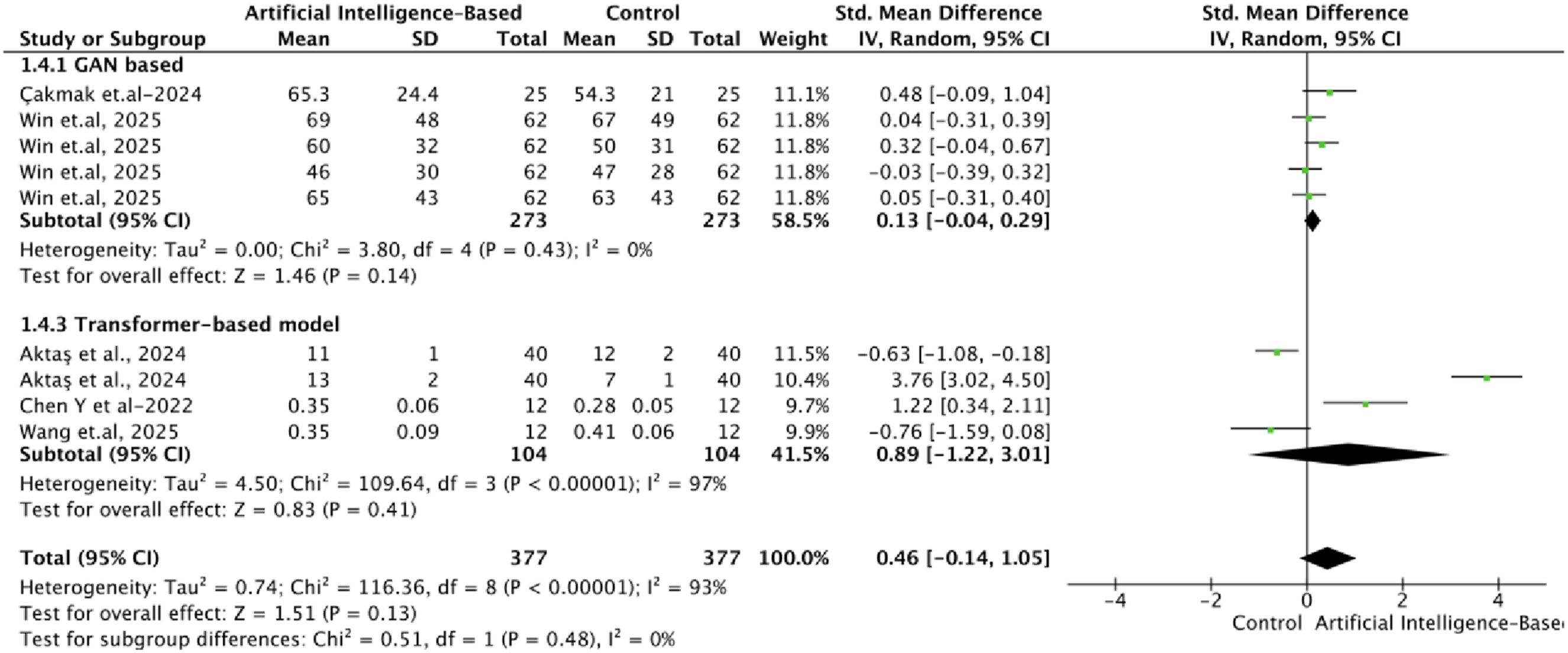


3.4.1. Geometric and Morphological Accuracy Outcomes
For overall accuracy (RMS deviation) (Figure 2), no statistically significant difference was observed between AI-based systems and control workflows. The pooled analysis demonstrated a negligible effect size (SMD = −0.15; 95% CI, −1.04 to 0.74; p = 0.74), indicating comparable overall geometric trueness between approaches. None of the subgroup’s comparisons revealed statistically significant differences (p ≥ 0.06). Similarly, the analysis of cusp angles (Figure 3) showed no statistically significant difference between groups (SMD = −0.24; 95% CI, −0.88 to 0.40; p = 0.45). Again, the subgroups analyses did not show any statistically significant differences (p ≥ 0.11).
For occlusal contact points (Figure 4), the pooled estimate also demonstrated no statistically significant difference (SMD = −0.43; 95% CI, −0.95 to 0.10; p = 0.11). However, when analyzing the subgroup of GAN based architecture, there was statistically significant differences, favoring the control group (p < 0.01). In the analysis of profile discrepancy (Figure 5), no statistically significant difference was identified between groups (p = 0.13); also, the subgroups analyses did not show statistically significant differences (p ≥ 0.14), suggesting comparable contour fidelity and morphological agreement. Similarly, internal fit (Figure 6) showed no statistically significant difference (p = 0.35), indicating equivalent internal adaptation and seating accuracy of restorations between AI-based and conventional approaches.
3.4.2. Marginal Accuracy and Efficiency Outcomes
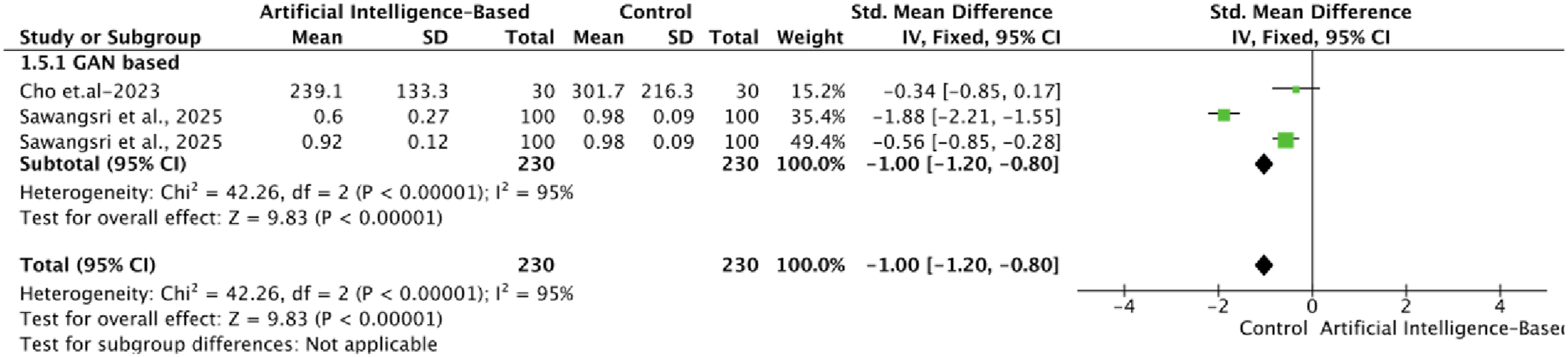
In contrast, statistically significant differences were observed for several clinically critical parameters. For chamfer distance (Figure 7), a highly significant difference was found, favoring AI-based systems (SMD = −1.00; 95% CI, −1.20 to −0.80; p < 0.00001). Despite substantial heterogeneity (Chi2= 42.26, df = 2, p < 0.00001; I2= 95%), the direction of effect was consistent across studies, indicating improved precision in finish line delineation.
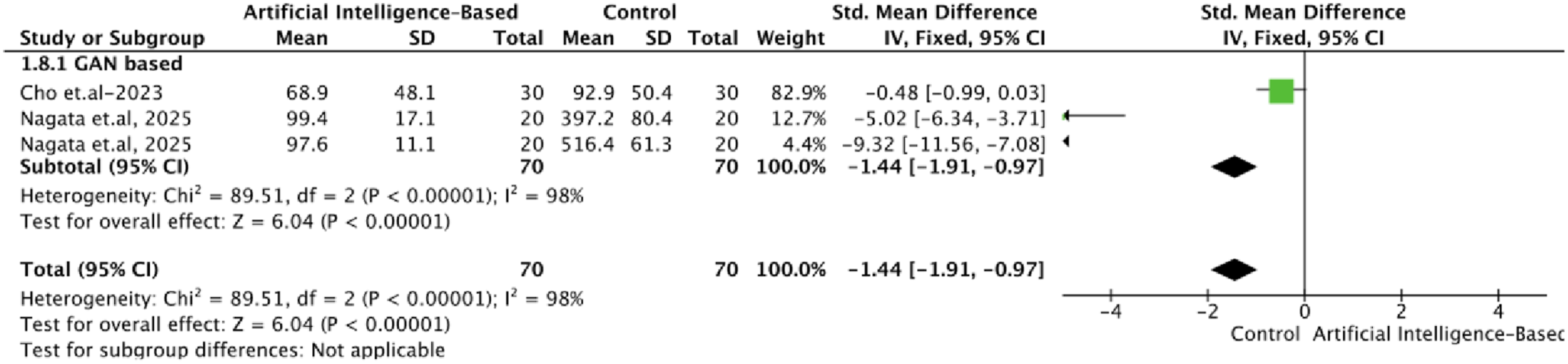
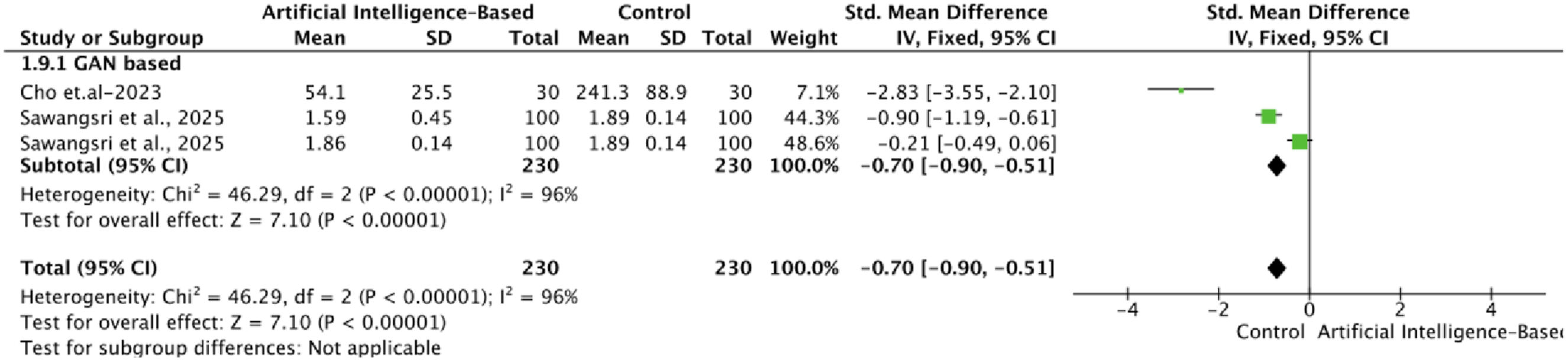
Similarly, the analysis of marginal gap (Figure 8) revealed a statistically significant difference (SMD = 0.44; 95% CI, 0.17 to 0.71; p = 0.001). For design time (Figure 9), a highly significant difference was observed (p < 0.001), indicating a clear advantage of AI-based systems in reducing workflow time and improving efficiency. This finding reflects the impact of automation and reduced operator dependency in AI-driven crown design.
Finally, occlusal morphology (Figure 10) demonstrated a statistically significant difference (p < 0.001), suggesting enhanced anatomical reconstruction and surface detailing in AI-generated designs compared to conventional methods.
Overall, the meta-analysis indicates that AI-based automated crown design systems achieve equivalent performance to conventional digital workflows in terms of geometric accuracy, occlusal contact relationships, and internal fit. However, significant advantages were identified in parameters directly related to clinical precision and workflow efficiency, particularly chamfer definition, marginal accuracy, design time, and occlusal morphology. Despite these promising findings, the consistently high heterogeneity observed across several outcomes highlights the influence of methodological variability, differences in AI algorithms, and inconsistencies in evaluation protocols. Therefore, while AI-based systems demonstrate clear potential to enhance digital prosthodontic workflows, further standardized and high-quality studies are required to confirm their clinical superiority and reproducibility.
4. Discussion
The present systematic review and meta-analysis provides a comprehensive and critical synthesis of the current evidence regarding AI-assisted crown design systems and their performance relative to conventional CAD-based and technician-driven workflows. The findings indicate that contemporary AI-driven systems are capable of producing restorations with clinically acceptable morphological accuracy, occlusal integration, and internal adaptation, while simultaneously offering substantial improvements in workflow efficiency and reproducibility. Based on the pooled quantitative analysis, the null hypothesis was partially rejected, as no statistically significant differences were observed for several primary outcomes, including overall morphological accuracy, occlusal contact relationships, and internal fit, whereas statistically significant improvements were identified in specific parameters, particularly marginal precision, chamfer definition, occlusal morphology, and restoration design time in favor of AI-based systems. However, important limitations persist, particularly in anatomically complex scenarios and in the accurate prediction of functional occlusal dynamics, supporting the current paradigm that AI serves as an adjunctive tool rather than a replacement for clinical expertise.
4.1. Morphological Accuracy and Anatomical Reproduction
The quantitative synthesis demonstrated no statistically significant differences between AI-generated and conventionally designed crowns in terms of overall geometric accuracy, as assessed by RMS deviation, or in cusp morphology. These results suggest that AI systems have achieved a level of global morphological fidelity comparable to established workflows. According to the studies, deviations for AI-generated crowns consistently fell within clinically acceptable thresholds, typically below 100–200 μm, indicating reliable geometric reproduction.1,6 In this context, morphological deviation was interpreted as clinically acceptable when RMS error remained within approximately ≤100–200 μm, reflecting established CAD/CAM restorative accuracy ranges reported in prosthodontic literature for indirect restorations. Importantly, this geometric agreement was paralleled by evidence of functional adequacy, as multiple investigations reported that AI-generated restorations maintained occlusal and biomechanical relevance alongside morphological accuracy.1,5,15,18 Advanced DL and GAN architectures demonstrated the ability to reproduce occlusal contact patterns, cusp inclinations, and tooth-axis alignment within clinically acceptable limits, as confirmed through digital articulation and three-dimensional superimposition analyses.1,15,25 Even in studies reporting minor deviations in cusp morphology or occlusal surface detail, these discrepancies remained within acceptable clinical thresholds and did not significantly compromise functional outcomes, reinforcing the reliability of AI-assisted crown design.3,5,18
Notably, systems such as Dentbird Crown (Imagoworks Inc., Seoul, Republic of Korea), 3Shape Automate (3Shape Fullcontour, Copenhagen, Denmark), and ToothGAN (Hong Kong, PR China) exhibited high reproducibility and close approximation to natural tooth morphology and technician-designed references across repeated designs.5,15 This consistency highlights a key advantage of AI-driven workflows, namely reduced operator dependency and enhanced standardization. Nevertheless, this reproducibility may come at the expense of reduced sensitivity to patient-specific occlusal dynamics, particularly in reproducing individualized anterior guidance and functional contact patterns. 26 Despite comparable global accuracy, several studies identified localized discrepancies in anatomically complex regions, including cusp tips, occlusal grooves, palatal surfaces, and anterior guidance contours.3,25,27 Reports of increased cusp angulation and incomplete reproduction of functional wear facets suggest that fine morphological detailing remains influenced by algorithmic constraints and the representativeness of training datasets.25,27 These findings indicate that while AI systems are effective in generating accurate baseline morphology, targeted clinician-driven refinement remains essential in esthetically demanding cases and complex occlusal scenarios.
4.2. Marginal Precision and Internal Adaptation
The evaluation of internal fit demonstrated no significant differences between AI-generated and conventionally designed crowns, confirming that AI systems can reliably reproduce internal geometries and seating accuracy. Clinically acceptable internal gaps and marginal discrepancies were consistently reported across different AI platforms. 6 Internal adaptation was interpreted as clinically acceptable when internal gap values remained within approximately ≤100–150 μm, consistent with widely reported tolerances for fixed prosthodontic restorations and CAD/CAM-fabricated crowns. The high reproducibility observed in internal adaptation likely reflects the capacity of machine learning algorithms to consistently identify preparation boundaries and replicate internal contours once adequately trained. 23 This predictability is further enhanced by automated digital workflows and AI-assisted evaluation methods, which provide more standardized and reproducible measurements compared with conventional manual techniques. 28
Importantly, the meta-analysis identified statistically significant improvements in marginal precision and chamfer definition favoring AI-based systems. Marginal adaptation was considered clinically acceptable when marginal gap values remained ≤120 μm, aligning with classical prosthodontic evidence linking marginal discrepancies below this threshold with improved long-term restoration survival and reduced microleakage risk. This finding suggests that AI algorithms may offer enhanced performance in finish line delineation due to reduced operator dependency and improved consistency in detecting preparation margins, owing to their ability to learn boundary conditions from large datasets. 1 Given that marginal integrity is a critical determinant of restoration longevity, this represents a meaningful clinical advantage. However, localized discrepancies have been reported, particularly in lingual or anatomically complex regions, especially when preparation geometries deviate from patterns represented in the training data. 6 These observations highlight the continued influence of input data quality and preparation standardization on AI performance and reinforce the need for clinician oversight.
4.3. Occlusal Function and Functional Integration
Regarding occlusal integration, the meta-analysis demonstrated no statistically significant differences in occlusal contact points or overall occlusal morphology between AI-based and conventional workflows, indicating that AI systems can reliably reproduce clinically acceptable static occlusal relationships. Occlusal outcomes were considered clinically acceptable when contact discrepancies did not lead to functional interference, loss of intercuspation stability, or requirement for major occlusal adjustment during simulated or clinical validation, corresponding to minimal deviation in digitally mapped contact distribution. Multiple studies have reported comparable occlusal contact distribution, contact intensity, and intercuspal alignment between AI-generated and technician-designed crowns.5,18 Furthermore, biomechanical simulations indicate that AI-generated restorations exhibit stress distribution patterns and fatigue resistance closely resembling those of natural dentition, supporting their functional adequacy under simulated loading conditions. 15 However, a critical technical limitation of current AI-based crown design systems is their predominant reliance on static three-dimensional geometric inputs derived from intraoral scans or digital dental casts. These datasets capture spatial morphology but lack temporal information required to model functional mandibular movements.29-31 As a result, most existing AI architectures are inherently optimized for static occlusion reconstruction rather than dynamic occlusal prediction. Accurate simulation of functional occlusion requires integration of kinematic and temporally resolved data, such as jaw-tracking systems, motion-capture recordings, or digitally simulated articulator pathways. 32 However, such multimodal datasets remain sparsely incorporated into current AI training pipelines, limiting the ability of models to predict excursion movements, adaptive contact patterns, and functional wear behavior under physiological loading conditions. This represents a fundamental bottleneck in the translation of AI-driven crown design from static morphological reconstruction toward fully functional occlusal modeling. 33
Performance variability becomes more pronounced in complex occlusal scenarios. Reduced accuracy in both occlusal and interproximal contacts has been reported in cases involving irregular occlusal schemes or altered anatomical relationships. 6 Interestingly, the subgroup analysis demonstrated significantly inferior occlusal contact point reproduction in GAN-based architectures compared with control workflows. This finding may be explained by the intrinsic objective of GAN models, which primarily emphasizes generation of morphologically realistic and visually coherent occlusal anatomy rather than explicit optimization of precise functional contact localization. Although GANs excel in reconstructing global surface morphology through adversarial learning, small deviations in cusp inclination, fossae depth, or marginal ridge contour may substantially alter occlusal contact distribution despite overall acceptable geometric similarity. In addition, GAN training commonly relies on static dataset-driven pattern learning without direct integration of biomechanical constraints, articulator dynamics, or real-time occlusal force mapping, thereby limiting functional precision. By contrast, conventional CAD workflows and technician-refined designs frequently incorporate rule-based occlusal adjustment protocols, virtual articulator simulations, and clinician-guided refinements specifically targeting stable intercuspation and contact optimization. Furthermore, adversarial training instability, mode collapse, and dependence on homogeneous training datasets may contribute to variability in GAN-generated contact accuracy, particularly in anatomically complex posterior occlusion. Consequently, despite demonstrating promising anatomical realism and efficient morphology generation, current GAN-based systems may remain less reliable for highly precise occlusal contact reproduction without integration of patient-specific dynamic functional data and subsequent clinician refinement. Emerging evidence suggests that incorporation of virtual articulators, jaw-tracking systems, and dynamic occlusion modeling into AI training frameworks may enhance functional alignment and improve prediction of mandibular movement pathways and adaptive occlusal behavior.34-36
4.4. Workflow Efficiency and Standardization
One of the most clinically impactful findings of this review is the substantial reduction in design time associated with AI-assisted workflows. Traditional CAD-based design requires multiple iterative steps, including occlusal adjustment, proximal contact refinement, and contour optimization. In contrast, AI algorithms can generate complete crown morphology within seconds by leveraging learned patterns from large datasets. Across the included studies, AI systems reduced design time by approximately 30–50% compared with conventional methods.19,21 However, an important methodological consideration is that “design time” was not consistently distinguished from “total workflow time,” particularly in relation to post-processing refinement. In several studies, reported efficiency metrics reflected only the initial AI-generated design phase, without accounting for additional manual adjustments performed by clinicians or dental technicians in cases involving complex occlusal anatomy or interproximal contacts. 3 This introduces a potential overestimation of net workflow efficiency. Accordingly, workflow efficiency should be interpreted as a composite construct comprising: (i) automated design generation time; and (ii) human refinement or correction time. While AI systems clearly reduce the initial design burden, the extent of efficiency gain in real clinical workflows is partially dependent on case complexity and the need for operator intervention. Nevertheless, these efficiency gains were observed irrespective of operator experience, suggesting that AI may contribute to standardizing design quality and minimizing variability associated with user skill. From a clinical and laboratory perspective, this has significant implications for chairside CAD/CAM workflows and high-throughput production environments. Nevertheless, efficiency should not be conflated with clinical completeness, as most studies emphasize that AI-generated designs still require clinician verification and occasional refinement prior to fabrication.8,19,22,23
4.5. Clinical Translation and AI Architecture Considerations
Variations in performance across studies can be partially attributed to differences in AI architecture. Early systems based on rule-based or statistical approaches were inherently limited in capturing complex three-dimensional morphological relationships. In contrast, modern data-driven frameworks, including convolutional neural networks, generative adversarial networks, and emerging transformer-based models, are capable of learning intricate spatial relationships between prepared teeth, adjacent dentition, and opposing occlusion.25,35 A study incorporating a two-stage deep learning framework established that AI models can generate occlusal crown structures through spatial learning relationships between tooth position, size, and surrounding anatomy, allowing precise reconstruction of crown surface morphology. 37 These architectures enable more anatomically realistic and functionally coherent crown designs by leveraging large-scale datasets. 5 Generative models, in particular, have demonstrated the ability to reconstruct missing dental structures with high anatomical fidelity, consistency, and realistic anatomic characteristics, encompassing occlusal surface details and functional morphology, representing a significant advancement over traditional CAD algorithms.34,38 However, despite these technological improvements, current AI systems remain dependent on the quality, diversity, and representativeness of training datasets, which may limit performance in atypical or complex clinical scenarios.
From a clinical perspective, the evidence strongly supports a hybrid human–AI workflow model. AI systems provide rapid, standardized baseline designs with high reproducibility, while clinician and technician expertise remains essential for refining esthetic details, optimizing occlusal relationships, and adapting restorations to patient-specific anatomical and functional conditions. Several studies demonstrated that clinician or technician refinement of AI-generated designs leads to improved morphological and functional outcomes, particularly in complex cases.3,8,19,22,23 This reinforces the concept that AI enhances clinical workflows rather than replacing professional judgment.
4.6. Limitations and Future Research Directions
Despite the promising findings, several limitations must be acknowledged. Substantial heterogeneity was observed across studies in terms of AI architectures, dataset characteristics, occlusal integration protocols, and outcome assessment methods, which may influence the robustness and generalizability of the meta-analytic findings. Additionally, the predominance of in vitro studies and limited clinical datasets restricts the ability to extrapolate results to long-term clinical performance. Moreover, most occlusal evaluation methodologies relied on static digital or laboratory-based assessments, including virtual articulators and three-dimensional superimposition analyses, which may not accurately reproduce real-time intraoral functional dynamics such as mandibular movement patterns and physiologic occlusal force distribution. 28 Most investigations focused primarily on geometric and mechanical parameters, with limited evaluation of clinically relevant outcomes such as restoration survival, wear behavior, biological complications, and patient-reported outcomes. Variability in measurement methodologies, including differences in RMS thresholds, occlusal contact assessment techniques, and marginal evaluation protocols, further complicates direct comparisons across studies. Moreover, potential sources of bias, including incomplete reporting of randomization, operator blinding, and dataset selection, were identified in several studies, highlighting the need for more rigorous methodological standards.
An additional methodological consideration is the presence of potential language bias. Although the literature search was performed without language restrictions at the level of database querying, inclusion in the qualitative and quantitative synthesis was restricted to English-language full-text publications due to feasibility constraints related to standardized data extraction and risk-of-bias assessment. In addition, an important but underreported limitation is the potential influence of training dataset composition on AI model performance. Most included studies relied on in vitro typodont models, single-center datasets, or standardized digital libraries, which may not adequately capture real-world clinical variability, including inter-individual differences in occlusal wear patterns, ethnic dental morphology, restorative history, and functional occlusal dynamics. This introduces a risk of model overfitting to homogeneous or laboratory-controlled datasets, whereby AI systems may learn dataset-specific morphological patterns rather than broadly generalizable anatomical representations. Consequently, reported “clinically acceptable accuracy” in controlled experimental settings should be interpreted cautiously, as it may reflect dataset-constrained validity rather than confirmed real-world clinical generalizability. Furthermore, external validation using independent and demographically diverse datasets was rarely reported, limiting confidence in cross-population applicability and robustness of currently available AI-driven restorative design systems.
These concerns are further compounded by substantial methodological and clinical heterogeneity across the included studies, which complicates the interpretation and synthesis of pooled outcomes. Although standardized mean difference (SMD) was employed to harmonize effect sizes measured on different scales, SMD does not resolve differences in tooth type (anterior vs posterior), restoration location (premolar vs molar), sample source (typodont, extracted teeth, or intraoral scans), comparator workflows (technician-designed, conventional CAD, or natural tooth references), or measurement methodologies (three-dimensional superimposition, micro-CT, silicone replica technique, or direct measurement). The substantial heterogeneity observed in several global pooled analyses (I2 exceeding 75% for chamfer distance, design time, and occlusal morphology) reflects these underlying differences. Subgroup analysis by AI architecture reduced but did not fully eliminate this heterogeneity, as residual variability persisted due to differences in training datasets, evaluation protocols, and outcome definitions. These findings underscore the urgent need for field-wide standardization of outcome metrics, measurement protocols, and reporting guidelines for AI-based dental restoration studies. Future research should adopt consensus-based core outcome sets to facilitate meaningful meta-analytic synthesis and direct comparisons across studies.
Future research should focus on the development of standardized evaluation protocols and the conduct of multicenter, prospective clinical trials with long-term follow-up. The integration of patient-specific functional data, including dynamic occlusal analysis and mandibular movement tracking, represents a critical area for advancement. Incorporating real-time functional simulation into AI training frameworks may enhance predictive accuracy and clinical applicability. Furthermore, continued validation of emerging AI architectures is necessary to determine their relative advantages and limitations in comparison with current systems.
5. Conclusions
AI-based automated crown design systems demonstrate clinically acceptable morphological accuracy, occlusal integration, and internal fit comparable to conventional workflows, with potential improvements in efficiency, reproducibility, and marginal precision. However, these findings should be interpreted as directional trends across heterogeneous experimental and early clinical studies rather than definitive evidence of superiority, given the substantial variability in study designs, AI architectures, and evaluation methodologies, as reflected in high heterogeneity across multiple pooled analyses. These systems do not yet consistently surpass expert human performance in complex anatomical and functional scenarios, particularly those involving dynamic occlusion and individualized patient factors. At present, the most effective clinical paradigm is a collaborative workflow in which AI-generated designs are critically assessed and refined by clinicians or dental technicians to ensure optimal individualized outcomes. Ongoing advances in generative AI, including GANs, diffusion models, and transformer-based architectures, are expected to further enhance performance and adaptability. Nevertheless, the establishment of standardized evaluation protocols and the generation of high-quality prospective clinical evidence remain essential to fully validate and integrate these systems into routine restorative practice.
Supplemental Material
Supplemental Material - Accuracy and Functional Performance of Artificial Intelligence-Based Automated Crown Design Systems: A Systematic Review and Meta-Analysis
Supplemental Material for Accuracy and Functional Performance of Artificial Intelligence-Based Automated Crown Design Systems: A Systematic Review and Meta-Analysis by Ahmed A. Holiel, Mounir M. Al Nakouzi, Carlos Enrique Cuevas-Suárez, Abigailt Flores-Ledesma, Sofia Drouri, Rim Bourgi in Biomedical Engineering and Computational Biology
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.