
Abstract
Drug-induced acute generalized exanthematous pustulosis is a rare pustular skin reaction, most commonly triggered by antibiotics. Although its diagnosis is based primarily on the presence of specific clinical and histopathologic features, additional in vivo (patch testing) or in vitro testing may be required, especially in atypical cases, to more accurately determine the causative agent. The authors report a histologically confirmed case of acute generalized exanthematous pustulosis that was induced by amoxicillin/clavulanic acid, as documented by subsequent patch testing, and presented with generalized painful lymphadenopathy, mimicking an acute infectious process. This is a very rare and diagnostically challenging clinical presentation of acute generalized exanthematous pustulosis, which has been reported, to the best of our knowledge, only once previously.
Acute generalized exanthematous pustulosis (AGEP) is a rare cutaneous reaction, which is clinically characterized by acute widespread eruption of numerous small (<5 mm), nonfollicular, sterile pustules on an oedematous erythema; high fever (>38°C); neutrophilic leukocytosis; and spontaneous resolution of symptoms within less than 15 days. 1 Skin biopsy typically reveals spongiform subcorneal and/or intraepidermal pustules, in conjunction with marked oedema and eosinophilic infiltration of the papillary dermis, perivascular neutrophilic infiltrates, and focal necrosis of keratinocytes. 2 In the overwhelming majority (~90%) of cases, AGEP is triggered by drugs (most commonly antibiotics), while viral infections, spider bites, mercury exposure, chemotherapy, radiation, and psoralen plus ultraviolet A have also been described in association with this condition. 3
Lymph node enlargement is included among the potential clinical features of AGEP 3 ; however, to the best of our knowledge, there is only 1 previous report of AGEP associated with massive lymphadenopathy. 4 We report herein a case of AGEP that was induced by amoxicillin/clavulanic acid, as confirmed by subsequent patch testing, and presented with generalized painful lymphadenopathy. The relevant literature is also briefly discussed, with emphasis on the diagnostic criteria of this rare condition and the role of patch tests in the diagnostic workup of patients with suspected drug-induced AGEP.
Case Report
A 37-year-old woman was admitted to “Sotiria” General Hospital (Athens, Greece) with a 12-hour history of high-grade fever (up to 40°C) and a pruritic skin rash that had first appeared on the back of the knees and then spread rapidly to the trunk and arms. The patient had been under treatment with oral amoxicillin/clavulanic acid for periodontitis for the past 3 days. Her medical history was remarkable for a similar episode of amoxicillin-associated exanthema at the age of 16 years. Physical examination revealed multiple small (<5 mm in diameter), nonfollicular pustules on an erythematous base affecting the trunk and limbs; painful lymphadenopathy (in the posterior cervical, postauricular, suboccipital, axillary, and inguinal regions); and tachycardia. Laboratory tests (including complete blood count with differential, electrolytes, blood glucose, renal and liver function tests, erythrocyte sedimentation rate, C-reactive protein, clotting panel, perinuclear antineutrophil cytoplasmic antibodies, cytoplasmic antineutrophil cytoplasmic antibodies, antinuclear antibodies, and rheumatoid factor) were all within normal limits except for mild leukocytosis (white blood cell count, 11 800/mm3). The results of viral serologic testing for Epstein-Barr virus, human immunodeficiency virus, hepatitis B virus, hepatitis C virus, herpes simplex virus–1 and herpes simplex virus–2, cytomegalovirus, and syphilis (rapid plasma reagin) were all negative. Blood culture and bacterial cultures from representative pustules were negative as well. A skin biopsy was also obtained, and the results were consistent with AGEP.
The patient’s symptoms did not respond to initial treatment with oral methylprednisolone (0.5 mg · kg–1 · d–1) and cetirizine, and on the third day of admission, her condition worsened, with temporary hemodynamic instability (which promptly reverted with volume resuscitation), as well as development of facial oedema and palpable purpura on the extremities. Skin biopsy of one of the purpuric lesions was compatible with leukocytoclastic vasculitis. At the same time, treatment with intravenous prednisolone (40 mg, 3 times daily) was initiated, with gradual resolution of the eruption followed by postpustular desquamation. The patient was discharged afebrile and asymptomatic 6 days later. Patch testing with β-lactam antibiotics (cefuroxime, penicillin, amoxicillin, ampicillin, and amoxicillin/clavulanic acid, all diluted at 10% in petrolatum) was performed 2 months later. The results were strongly positive for ampicillin, amoxicillin, and amoxicillin/clavulanic acid, weakly positive for penicillin, and negative for cefuroxime and control (petrolatum) (Figure 1).
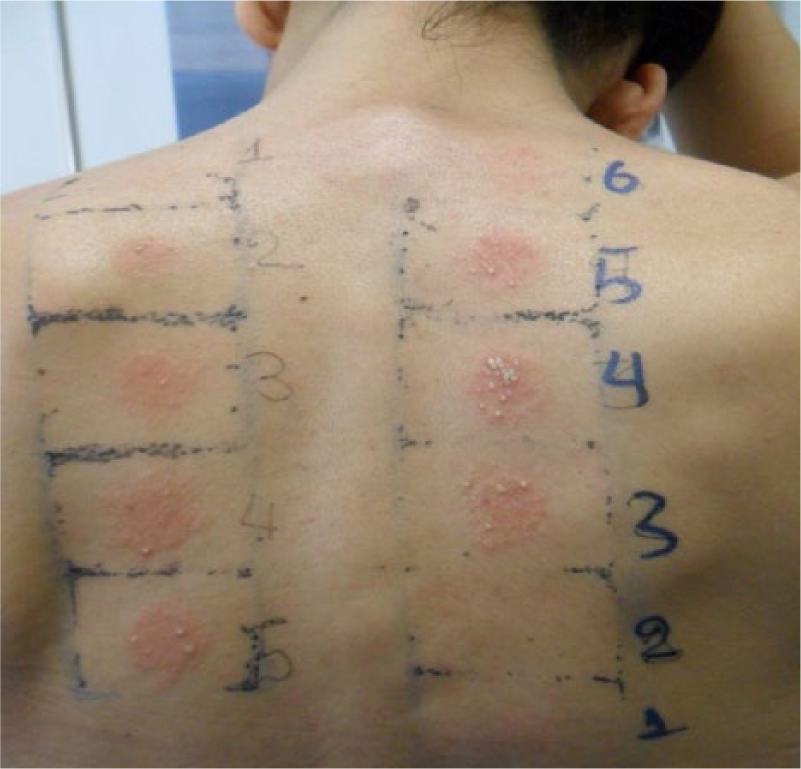
Results of patch testing showing: (a) strong positive, pustular reactions to ampicillin (number 4), amoxicillin (number 5), and amoxicillin/clavulanic acid (number 3); (b) a weak positive reaction to penicillin (number 1); and (c) negative reactions to cefuroxime (number 2) and control (petrolatum) (number 6).
Discussion
Drug-induced AGEP is a rare but well-described pustular skin reaction, with a characteristic clinical and histopathologic pattern. In previously sensitized patients, onset of symptoms is rapid, occurring within hours to 2 to 3 days after drug intake, while a more extended interval of 1 to 3 weeks may be encountered when a new drug is administered. 5 The eruption begins with a pruritic oedematous erythema, most commonly in the face or the intertriginous areas, before spreading to the trunk and extremities and is typically accompanied by high-grade fever and increased neutrophil count.3,6 Mucosal involvement may be found in a minority (~20%) of cases, while other atypical symptoms may include marked facial oedema, purpura, atypical target lesions resembling those seen in Steven-Johnson syndrome, blisters, and vesicles. 5
A detailed scoring system for validation of the diagnosis of AGEP was recently proposed by Sidoroff et al 5 on the basis of the results of a multinational epidemiologic study of severe cutaneous adverse reactions (the EuroSCAR project) and is increasingly applied worldwide. According to this scoring system, several key clinicopathologic features (with regard to morphology of the eruption, disease course, and skin biopsy findings) are evaluated, and cases are categorized as negative, possible, probable, or definite for AGEP, depending on the overall score. The total score in our case was 9 of 12, suggesting a definite diagnosis, while histopathology, which is widely recognized as the diagnostic gold standard, showed features consistent with AGEP.
A striking and atypical finding in our patient was the presence of generalized lymphadenopathy at disease onset, which gradually resolved, along with resolution of the remaining symptoms. This is a very rare manifestation of AGEP, which has been reported, to the best of our knowledge, only once previously, in a case of AGEP with a lymphoma-like presentation and a presumed viral etiology. 4 Our case suggests that painful widespread lymphadenopathy, closely mimicking an acute infectious process, although extremely rare, may be observed in drug-induced cases of AGEP as well. Differential diagnosis in these instances should be guided by the morphology and distribution of the eruption, the accompanying clinical signs and symptoms, a thorough evaluation of potential involvement of internal organs, the skin biopsy results, and the results of laboratory investigations, including serologic screening for probable infectious agents.
Although the diagnosis of drug-induced AGEP is usually based on its typical clinical presentation and histopathology, as discussed above, additional in vivo (patch tests) or in vitro testing (such as the lymphocyte transformation test, the macrophage migration inhibition factor test, and the mast cell degranulation test) may be required to safely confirm the causative agent.7,8 Despite the reportedly low sensitivity (~50%) of patch testing in AGEP,5,8 this diagnostic method remains a first-line tool in the evaluation of cutaneous adverse reactions, because of its excellent safety profile, high specificity, simplicity, low cost, and rapidity of results. Interestingly, strong, even pustular reactions on patch testing are more frequent in AGEP compared with other drug-induced skin reactions.5,7 In our patient, patch testing showed a strong pustular reaction to ampicillin, amoxicillin, and amoxicillin/clavulanic acid and a weak reaction to penicillin. Similarly to our findings, Bomarrito et al 9 previously reported a case of AGEP with multiple positivity to β-lactam patch testing and hypothesized that a T cell–mediated response to β-lactams common ring may be involved in the pathogenesis of this clinical pattern.
In conclusion, we report herein a rare case of drug-induced AGEP presenting with generalized painful lymphadeno-pathy. The diagnosis of this uncommon cutaneous reaction should be based on thorough clinical and laboratory investigations, especially in the presence of atypical clinical features, as in our reported case. Patch testing may play a decisive role in confirming the culprit drug and implementing the most appropriate avoidance strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.