
Abstract

Introduction
Defects that involve the cosmetic subunits of the nose such as the nasal ala can be a reconstructive challenge especially when they cross multiple subunits and involve the alar groove. 1 Because the cosmetic subunits of the nose are critical facial landmarks and help to maintain a normal aesthetic appearance, preservation of the contours and topographic relationships of these subunits is imperative to achieve acceptable cosmetic outcomes. For example, blunting of the crescentic alar groove yields suboptimal results as it diminishes the natural demarcation between the nasal ala and the medial cheek and creates an unnatural appearance. Many current reconstructive options for larger nasal defects are multistaged repairs such as staged paranasal or melolabial flaps or the paramedian forehead flap that can place significant burden on the patient with regard to downtime, wound care, poorly hidden donor site scars, and transfer of hair-bearing skin.2-4 For certain patients, such as the very elderly, these multistaged repairs may not be well tolerated. There are limited single-staged repairs published in the literature that maintain functionality and acceptable cosmetic outcomes for nasal defects that involve multiple cosmetic subunits such as the single-stage melolabial transposition flap, although for larger defects that involve the nasal ala and extend into the nasal sidewall, blunting of the alar groove is likely. 5
We present a new option for certain large Mohs micrographic surgical defects that may involve such nasal cosmetic subunits as the nasal ala, alar groove, and nasal sidewall. This option is a single-staged double transposition pedicle flap that we have dubbed the “butterfly flap” because of the flap design. This reconstructive repair has been performed on 6 patients thus far and has evolved after each case with notable improvement in the final outcome. Our results have been shown to maintain functionality with acceptable cosmetic results.
Design and Execution
The butterfly flap (Figure 1) uses skin that is similar in texture and sebaceous character to the nasal subunits by using skin along the nasal sidewall superiorly and the melolabial fold inferiolaterally in its flap design. There is ample skin at these donor sites, making them ideal locations for tissue recruitment. For defects that involve the alar groove, this flap attempts to preserve the contour of this important facial landmark. For deeper defects and for defects near the alar rim, cartilage grafts may be required to ensure that the alar rim is not compromised and patency of the airway is maintained.
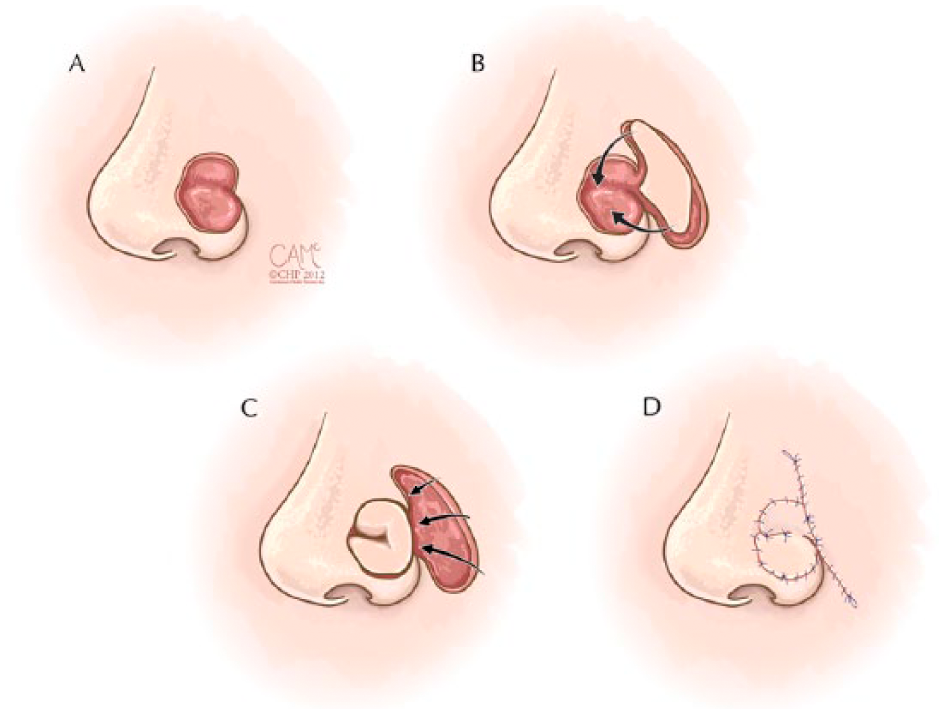
Drawing of the double transposition pedicle butterfly flap. (A) Surgical defect. (B) Flap design of 2 connected transposition flaps with an adequate pedicle. (C) Transposition of “wings” of butterfly into primary defect with creation of secondary defect. (D) Immediate postoperative sutured result.
The initial flap design of the first few cases involved 2 independent transposition flaps from the same donor sites as described above (Figures 2 and 3), 1 superiorly along the nasal sidewall and 1 inferiorly extending from the lateral nasal groove inferiorly to the melolabial fold. The first few cases proved to have good results; however, some blunting of the nasofacial sulcus was noted at follow-up visits. For this reason, the most recent patient’s flap was designed as a connected island pedicle flap with the superior aspect of the flap being transposed into the superior aspect of the surgical defect and the inferior aspect of the flap being transposed into the inferior aspect of the surgical defect, mimicking the outline of the wings of a butterfly. This approach helped to prevent blunting as the donor sites were sutured continuously and aided in maintaining the nasofacial sulcus superiorly and the melolabial fold inferiorly (Figure 4). The flaps are sutured to the skin that surrounds the defect as well as to each other centrally, as shown in all of the figures. This site where the 2 connected flaps meet each other can help re-create the concavity of the alar groove in defects that involve the nasal ala, alar groove, and nasal sidewall, as the inferior aspect of the flap can re-create the convex contour of the nasal ala while the superior aspect of the flap can fill the aspect of the defect that involves the nasal sidewall. A tacking suture at this central site may also assist in maintaining the concavity of the alar groove.
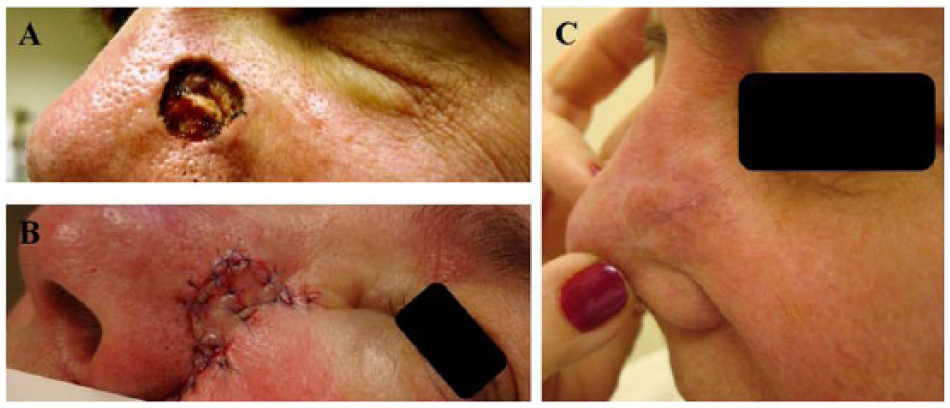
(A) Surgical defect. (B) Immediate postoperative sutured result. (C) Result 3 years later.
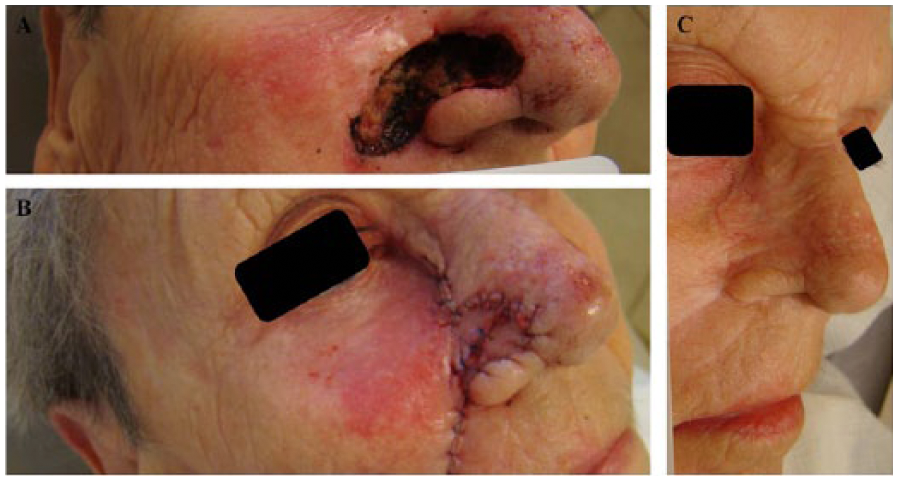
(A) Surgical defect. (B) Immediate postoperative sutured result. (C) Result 9 months later.
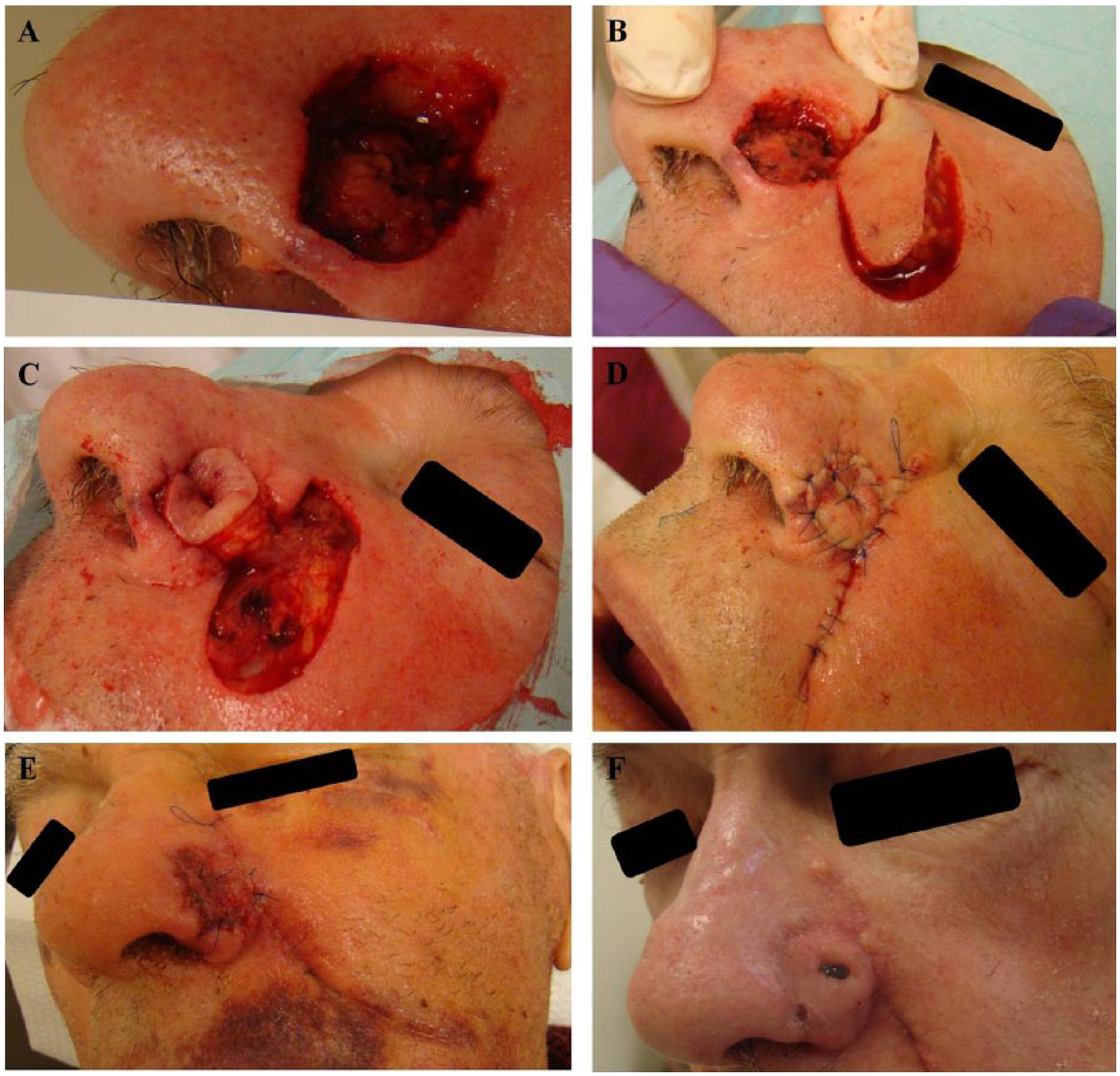
(A) Surgical defect. (B) Flap design of 2 connected transposition flaps with an adequate pedicle. (C) Transposition of “wings” of butterfly into primary defect with creation of secondary defect. (D) Immediate postoperative sutured result. (E) Postoperative day 7. (F) Postoperative day 26.
This double transposition pedicle butterfly flap is considered a random pattern flap that has a robust blood supply through perforators of the facial and angular arteries as long as an adequate pedicle is maintained to ensure the flap’s longevity. This flap design is an excellent single-stage option as the scars from both sites are well hidden at the nasofacial sulcus superiorly and at the melolabial fold inferiorly. It is important to note that if the flap is not sized appropriately, there is risk for pincushioning.
Conclusion
We report the successful reconstruction of defects that involve multiple nasal subunits with the Perez butterfly double transposition pedicle flap. For the appropriately selected patient, this single-stage repair is a new option that preserves the functionality and aesthetics of nasal cosmetic units. Its design saves patients from burdensome multistaged repairs, uses tissue that is similar in character to fill the defect, hides donor site scars well, maintains the contour of the nasal ala, and helps to preserve the cosmetic subunits of the nose.
Footnotes
Acknowledgements
The authors would like to acknowledge Courtney A. McKenna, medical illustrator, for her assistance in developing the drawings for Figure 1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.