
Abstract
Background:
Organ transplant recipients (OTRs) are at an increased risk of developing a de novo malignant neoplasm compared to the general population. The primary contributor to skin cancer in all patients is sun exposure.
Objective:
In this study, we aim to ascertain both OTR skin cancer awareness and photoprotection practices.
Methods:
A questionnaire-based study of Saskatchewan transplant recipients.
Results:
Nearly all respondents were aware that sun exposure is the best-known cause of skin cancer and that as an OTR, they are at increased risk of skin cancer (99.3% and 90.5%, respectively). Approximately half of respondents reported wearing a hat regularly, sun avoidance between 10
Conclusion:
Many OTRs are not engaging in photoprotection. Further intervention, which may include access to a dermatologist, is necessary to ensure ORTs do not experience undue morbidity and mortality secondary to skin cancer.
Background
Organ transplant recipients (OTRs) are at an increased risk of developing a de novo malignant neoplasm compared to the general population. 1 Skin neoplasms remain the most common cancer among OTRs, constituting nearly 40% of all posttransplant malignancies. 2 Approximately 50% of OTRs will develop at least 1 type of skin cancer. 3 In fact, OTRs have a 100-fold increased risk of developing a squamous cell carcinoma compared to the general population. 4 Skin cancer is an important cause of morbidity and mortality in OTRs, and while most skin cancers are not lethal in immunocompetent individuals, this is not the case for OTRs, who are chronically immunosuppressed.
The primary contributor to skin cancer in all patients is sun exposure, but recent research has suggested that the typical chronicity of UV-induced skin cancer is accelerated in transplant patients. 3 In this study, we aim to ascertain patient awareness of the risk of skin cancer and the need for both skin surveillance and sun avoidance in a population of solid organ transplant recipients.
Methods
All patients in the Saskatchewan transplant program who had a transplant from 1979 to 2011 were contacted to participate in this study. This study was approved by the University of Saskatchewan behavioural research ethics board.
An anonymous mail questionnaire was sent to all patients by the Saskatchewan transplant program along with a letter indicating that the research was being conducted by the division of dermatology. The study investigators developed the survey. The survey consisted of 14 questions and collected information regarding awareness of skin cancer risk, current sun-protective practices, history of skin cancer, and skin cancer surveillance and follow-up. The questions and response choices were developed in such a way that responses could be scored as a nominal outcome. See Figure 1 for an outline of the survey.
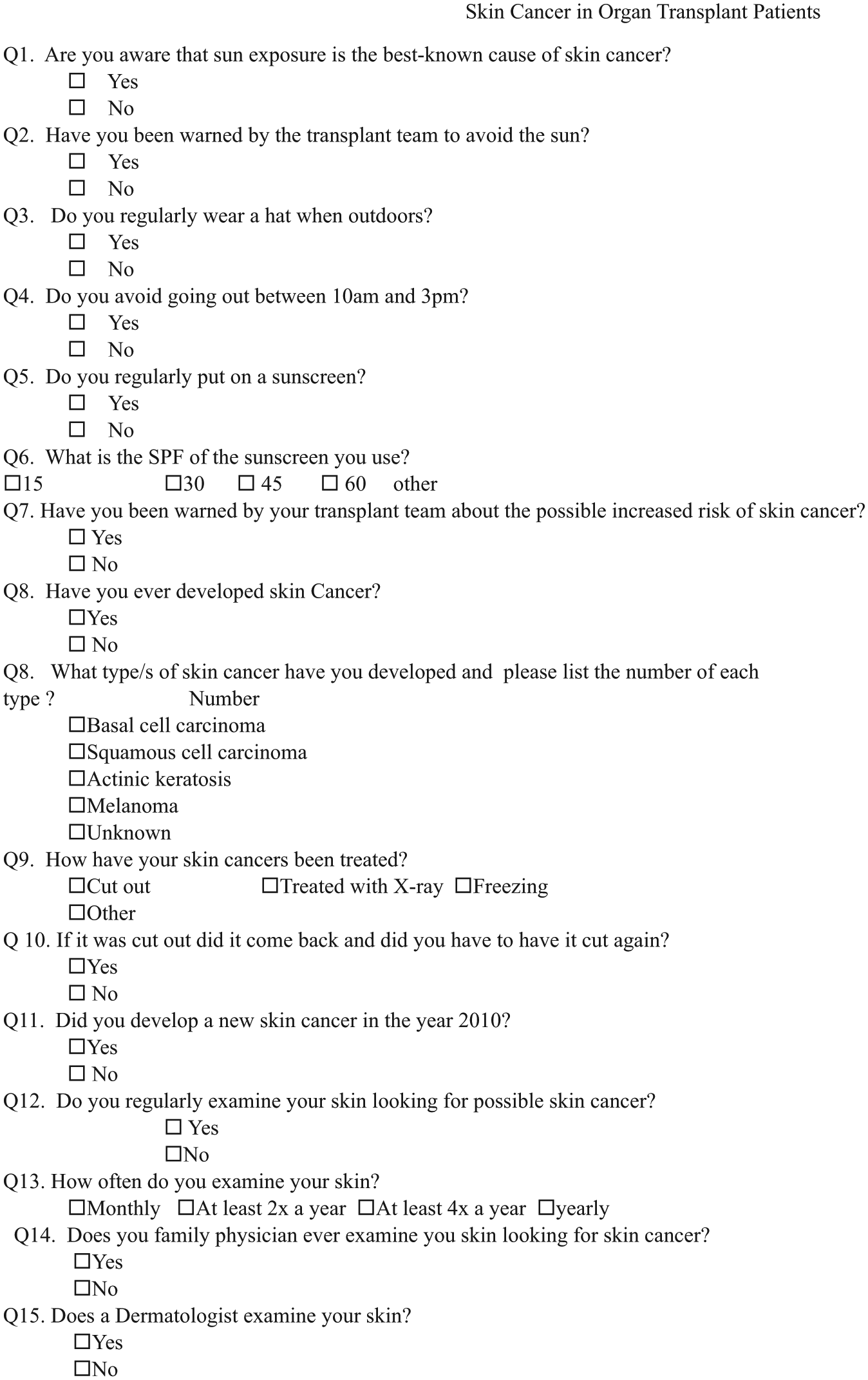
Outline of the survey.
Statistical Analysis
Analysis of survey responses was performed to calculate response frequency. Responses from patients with and without a self-reported history of skin cancer were compared to see whether this influenced their sun protection behaviour. Responses from patients who had ever had a skin exam performed by a dermatologist were compared with those who had never had a skin exam performed by a dermatologist. All data analyses were performed using SPSS computer software version 20 (SPSS, Inc, an IBM Company, Chicago, Illinois). For quantitative data, the difference in proportions was analysed with the Fisher exact test and the χ2 test for 2 × 2 contingency square when the number of subjects was <5 or >5, respectively. P < .05 was considered significant. We prepared histograms of total response by question using Microsoft Excel version 14.0 (Microsoft, Redmond, Washington).
Results
The response rate was 33.1% (149) for the 450 surveys distributed. Some surveys were incomplete; therefore, we performed our analysis based on the data available for each individual question.
Photoprotection, Skin Cancer Education, and Awareness
Overall, 148 respondents (99.3%) were aware that sun exposure is the best-known cause of skin cancer, and 133 respondents (90.5%) reported that their transplant team had warned them about the possible increased risk of skin cancer. Similarly, 138 respondents (94.5%) reported having been warned by the transplant team to avoid the sun.
Photoprotection Practices
Eighty respondents (53.7%) reported wearing a hat regularly when they are outdoors, and 48 respondents (33.1%) reported avoiding going out between 10
Skin Cancer History
Twenty-seven (18.4%) respondents reported a diagnosis of skin cancer. This included 7 cases of squamous cell carcinoma, 9 cases of basal cell carcinoma, 3 cases of actinic keratosis, 5 cases of melanoma, and 11 cases of an unknown skin cancer.
Of the 27 patients who reported having had a skin cancer, 23 (85.2%) reported having at least 1 cancer excised and 7 (30.4%) reported having a reexcision.
Of the patients diagnosed with skin cancer, 13.5 (50.0%) reported regular use of sunscreen compared to 56 (47.5%) patients who had not been diagnosed with skin cancer. The rates of hat use were not significantly different between patients with a history of skin cancer and those without (59.3 vs 53.3%, respectively). Similarly, there was no significant difference between patients with and without a skin cancer diagnosis with respect to avoiding the sun between 10
Skin Cancer Surveillance
In total, 114 respondents (79.2%) reported that they regularly examine their skin for skin cancer. Sixty-seven patients (65.7%) reported they self-examine monthly, 6 patients (5.9%) reported they self-examine at least 4 times a year, 23 patients (22.5%) reported they self-examine at least twice a year, and 6 patients (5.9%) reported they self-examine annually.
Only 38 respondents (25.8%) reported that their family physician had examined them for skin cancers, and 26 respondents (17.7%) reported that a dermatologist examines their skin. Of the respondents who reported that their family physician examined them for skin cancer, 7 (18.4%) also saw a dermatologist. The rate of regular sunscreen use was higher among those who had been examined by a dermatologist compared to those who had not (72.0% vs 42.0%, P = .006). There was no significant difference in hat use or avoidance of sun between 10
Discussion
This cross-sectional survey-based study of OTRs’ photoprotective practices and levels of skin cancer awareness demonstrated that most (90.5%) respondents were aware of their increased risk of skin cancer and the role that sun exposure plays in increasing that risk (99.3%). Similarly, most of the respondents reported that they had been told to avoid the sun by their transplant team. Previous studies have shown varied results with respect to patient advice, with 40% to 96% of responders reporting receiving photoprotection advice.4-6 Similar ranges in response rates have been reported with respect to OTR knowledge regarding the connection between skin cancer and sunlight and the increased risk of skin cancer among OTRs.4,6-8
Although respondents were aware of their increased cancer risk and the role of chronic sun exposure, only approximately half of respondents practiced regular photoprotection (hat use, midday sun avoidance, and regular sunscreen). Our findings are similar to others reported in the literature. A 2004 study of sun protection attitudes and behaviour in OTRs by Robinson and Rigel 9 found that 35% of OTRs used sunscreen. Another study of liver transplant patients found that 66% of surveyed patients reported using sunscreen, while only 31.8% reported using sunscreen with an SPF >30. 7 Our study found that nearly all patients who wore sunscreen regularly used an SPF of 30 or greater.
Several theories have been suggested regarding the discrepancy in transplant patient knowledge of increased risk for skin cancer and behaviour. A study of renal transplant recipients found that patients did not perceive the threat of skin cancer as an important health problem. Therefore, they did not give a high priority to sun protection, even though they were aware of their increased risk of developing skin cancer. This study also found that patients, particularly male patients, had negative individual attitudes towards the use of sunscreens. 10
The cost of sunscreen has also been suggested as a barrier to its use.10-12 Lautenschlager et al 11 estimated that the annual cost of sunscreen for an OTR to adhere to the recommendations for the quantity and frequency of application ranges from US$245.30 to US$292.30 per year. In fact, some authors believe that OTRs should receive broad-spectrum sunscreen as treatment provided by health care systems in order to improve compliance. 12
This study examined whether either a history of skin cancer or contact with a dermatologist affects a patient’s photoprotection behaviours. We found no significant increase in any measured photoprotection behaviours among those OTRs with a history of skin cancer. Conversely, we did find that OTRs who had visited a dermatologist were more likely to report regular sunscreen use than those who had not visited a dermatologist. These results are supported by Ismail et al, 4 who found that the use of photoprotective measures was significantly higher among OTRs who had attended a specialist dermatology clinic. They concluded that the delivery of education messages regarding skin cancer may be improved if it is provided in a specialist dermatological setting. Additionally, guidelines from the Kidney Disease: Improving Global Outcomes Transplant Work Group recommend that adult OTRs should have an annual skin and lip exam performed by a qualified health professional with experience in diagnosing skin cancer. 13 Unfortunately, only 17.7% of respondents in this study reported that a dermatologist examines their skin.
According to surveillance data collected by the Saskatchewan Cancer Agency, the incidence of skin cancer in the province from 1998 to 2007 was approximately 2.6%. 14 The incidence of skin cancer among OTRs in this study was 18.4%. Among kidney and heart transplant recipients, the incidence of nonmelanoma skin cancer and melanoma has been reported to be 65 to 250 and 3 to 4 times higher than the general population, respectively. 15 The rate of skin cancer among OTRs appears to vary by organ type. A Swedish population-based study found that among liver transplant recipients, the rate of all skin cancers was only 16 times higher than the general population. 16
Our study had a number of limitations, including its cross-sectional survey-based nature. One of the major limitations of this study design is recall bias. In particular, the skin cancer history data (positive skin cancer history, number of skin cancers, skin cancer type and treatment) are potentially subject to this form of bias. Recall bias may, at least in part, explain why the rates of skin cancer reported in this study group were not as high as those reported in the literature. The inclusion of solid organ transplant recipients from the province of Saskatchewan only in this study makes the generalisation of the results to all transplant recipients questionable because of the differences in resources, particularly dermatologic care, across provinces.
Conclusion
OTRs in the province of Saskatchewan are aware of the association between UV exposure and skin cancer, and they are being informed by the transplant program that they are at increased risk of skin cancer. However, this knowledge is not reliably translating into action, with nearly half of OTRs surveyed reporting that they did not participate in photoprotective practices. Contact with a dermatologist does appear to increase OTR participation in photoprotective practices and so may represent an area of future intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.