
Abstract
Oral glucocorticoids are commonly used across every field of medicine; however, discontinuing them in patients can be challenging. The risk of acute adrenal crises secondary to glucocorticoid withdrawal can be fatal and arises from chronic suppression of the adrenal glands. Identifying risk factors for adrenal suppression in dermatological patients, such as doses greater than 5 to 7.5 mg of prednisone equivalent, duration of glucocorticoid use greater than 3 weeks, certain medications, and comorbidities, can help risk-stratify patients. The use of adrenal gland testing such as basal cortisol levels and adrenocorticotropic hormone stimulation tests can confirm adrenal suppression in patients. This review article provides an approach that dermatologists can use to minimise the risk of adrenal insufficiency in patients discontinuing glucocorticoids and when it may be appropriate to use adrenal gland testing.
Use of Oral Glucocorticoids in Dermatology
The use of oral glucocorticoids as anti-inflammatory agents is highly prevalent in the field of dermatology. Treatment for various dermatitides, vasculitides, bullous diseases, sarcoidosis, and other cutaneous diseases relies on glucocorticoid use to diminish symptoms. Short-term use of glucocorticoids is generally associated with milder and less common side effects compared to long-term use. 1 However, it is important to understand the side effects associated with both short-term use and long-term use of oral glucocorticoids and counsel patients accordingly (Table 1). 2
Short-Term and Long-Term Side Effects of Oral Glucocorticoids. a
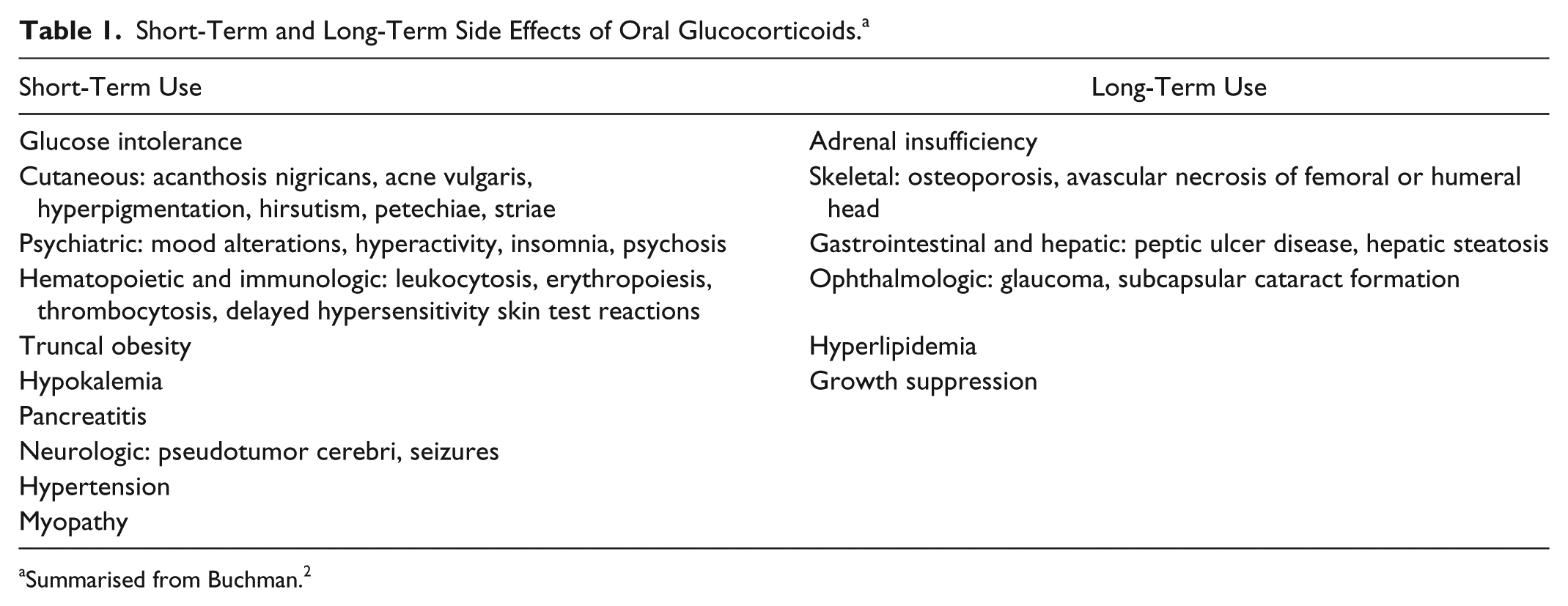
Summarised from Buchman. 2
Adrenal Insufficiency
A particularly life-threatening complication of glucocorticoid use is adrenal insufficiency. The hypothalamic-pituitary-adrenal (HPA) axis (Figure 1) plays a role in helping the human body respond and adapt to physiologic stresses. The use of glucocorticoids can suppress this axis and prevent appropriate cortisol production. The clinical symptoms of adrenal insufficiency tend to be nonspecific and include fatigue, anorexia, gastrointestinal discomfort, myalgia, dizziness, and fever. 3 Furthermore, severe exogenous oral and inhaled glucocorticoid withdrawal-induced adrenal crises have led to a number of fatal adrenal crises, some without any identifiable triggers, as shown by Dinsen et al. 4 Although less common, adrenal suppression has additionally been reported in intra-articular 5 and topical 6 glucocorticoid use.
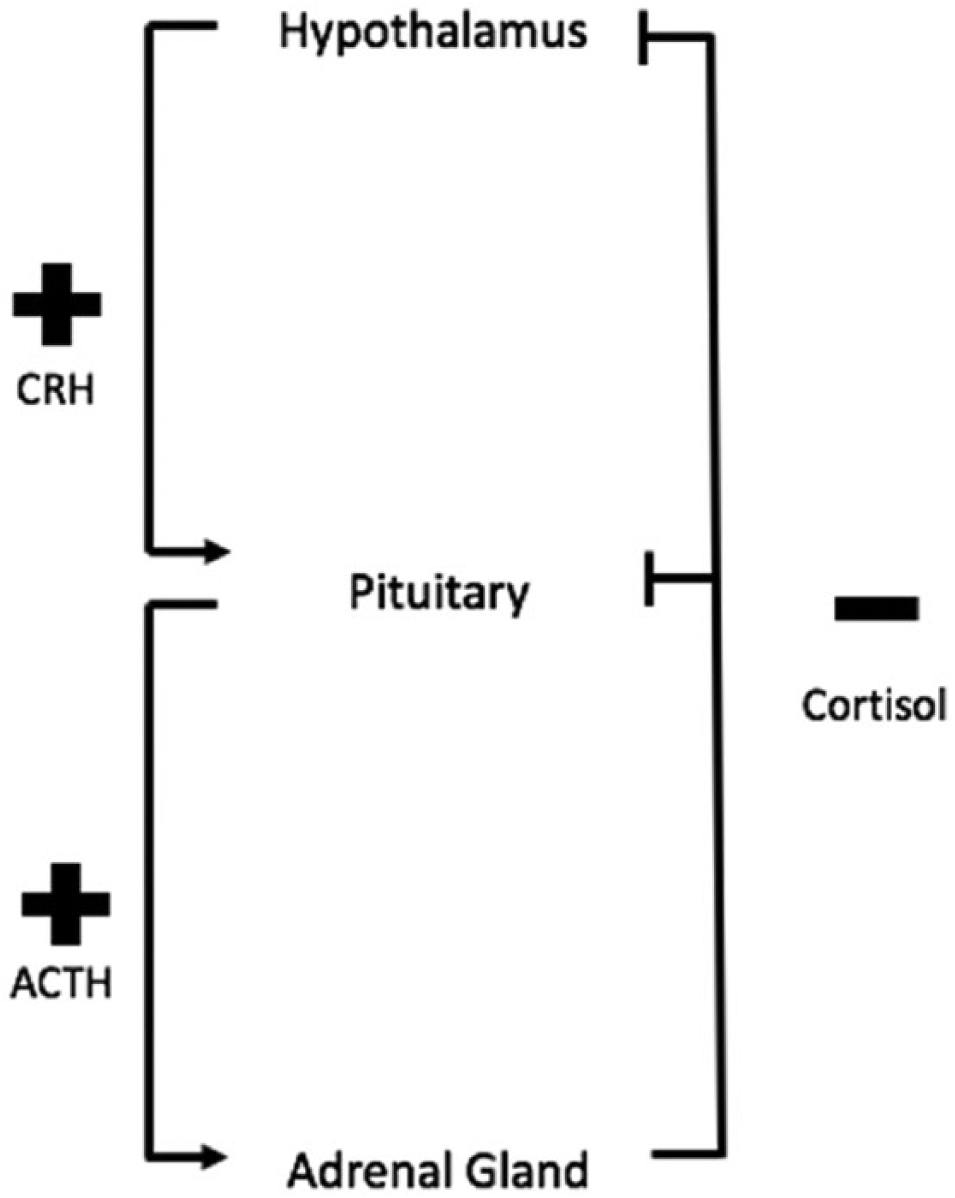
The hypothalamic-pituitary-adrenal axis. The hypothalamus secretes cortisol-releasing hormone (CRH), which stimulates the pituitary to secrete adrenocorticotropic hormone (ACTH). This will stimulate cortisol production from the adrenal gland, which has an inhibitory effect on the pituitary and hypothalamus.
Steroid Withdrawal Syndrome
Although documented cases of adrenal insufficiency leading to adrenal crises are uncommon, cases of steroid withdrawal syndrome (SWS) are much more likely to be seen in clinical practice. Patients with SWS exhibit clinical findings of fatigue, mood changes, flu-like symptoms, and nausea similar to patients with adrenal insufficiency but, unlike patients with adrenal crises, do not exhibit profound hypoglycemia and hypotension. Patients with SWS also do not exhibit changes in serum cortisol. The need for appropriate tapering of glucocorticoids is crucial for prevention of both adrenal insufficiency and SWS. 7
Subclinical Adrenal Insufficiency
Adrenal insufficiency in long-term use of oral glucocorticoids can easily go unrecognised. Patients who are symptomatic may only present with nonspecific symptoms, thus making adrenal insufficiency difficult to diagnose. Furthermore, many patients do not present with any symptoms. A 2015 meta-analysis looking at studies that tested patients for adrenal insufficiency after glucocorticoid use found only 10 patients reporting symptoms of adrenal insufficiency out of 521. Yet when the serum cortisol level of the same patient pool was tested, 98 were defined as adrenal insufficient. 8 The meta-analysis also found that the percentage of adrenal insufficiency in patients after oral corticosteroids was 48.7%, although a number of limitations due to heterogeneity and bias in studies used were reported. 8 Therefore, even when patients are asymptomatic, they may be at risk for subclinical adrenal insufficiency, which could put them at risk for adrenal crises if they are faced with a large physiological stressor. Clinical symptoms do not reliably represent the amount of adrenal suppression in clinical practice, and the use of adrenal testing, discussed below, can be helpful in identifying subclinical adrenal insufficiency.
Risk Factors for Adrenal Insufficiency When Discontinuing Glucocorticoids
Variability in both patient susceptibility to adrenal suppression and rate of adrenal function recovery makes it difficult to anticipate which patients are likely to have glucocorticoid withdrawal-induced adrenal insufficiency. 9 However, a number of factors can be used to help identify high-risk patients.
Glucocorticoid Potency
The potency of an oral glucocorticoid directly affects the amount of adrenal suppression that occurs. Oral glucocorticoids differ based on their relative glucocorticoid potency (Table 2). 10 For example, 5 mg prednisone has approximately the same glucocorticoid potency as 20 mg cortisol.
Relative Glucocorticoid Potency of Commonly Used Glucocorticoids. a
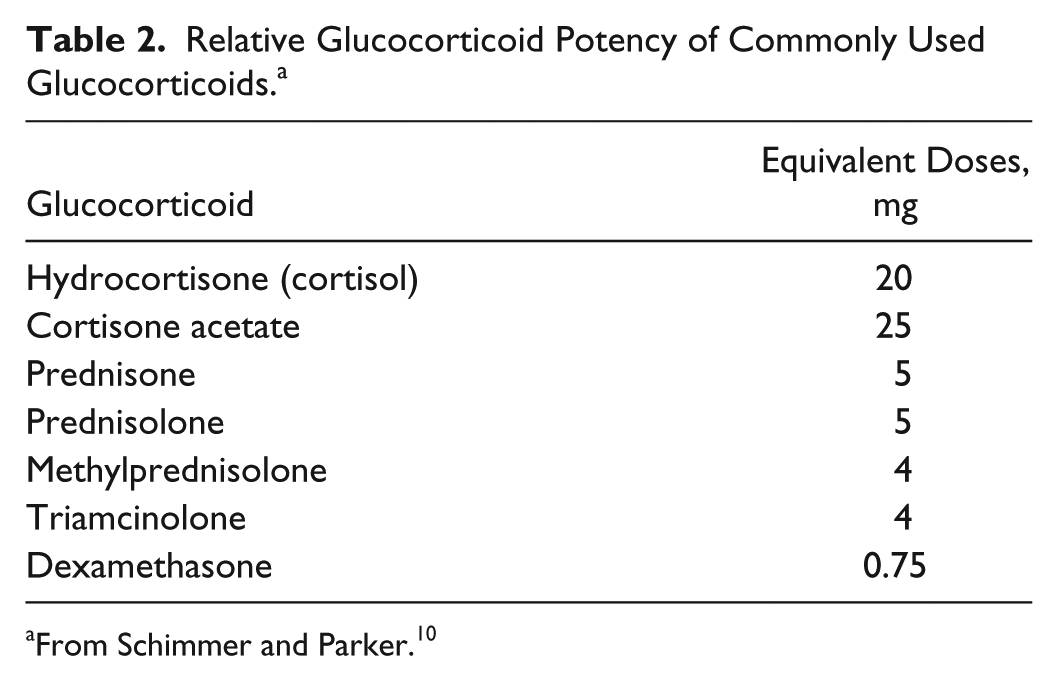
From Schimmer and Parker. 10
Currently, there is no defined lower limit dose where zero risk of adrenal insufficiency exists. The physiologic production of cortisol has been measured at approximately 10 mg/d in healthy volunteers, equating to approximately 2.5 mg/d of prednisone. 11 Adjusting for bioavailability and patient variation, the physiologic dose of oral prednisone is generally agreed to be around 5 to 7.5 mg/d.7,12,13 Patients on glucocorticoids at subphysiologic doses of prednisone do not appear to be at risk for symptomatic adrenal suppression 14 and are therefore deemed low risk. Doses of <5 mg/d of prednisone equivalent are still associated with a risk of blunted serum cortisol production after cortisol-releasing hormone (CRH) stimulation tests. 15
Duration of Glucocorticoid Therapy
Adrenal suppression occurs quite quickly with glucocorticoid use. Patients on supraphysiologic doses of prednisone for 5 days are frequently stopped abruptly without symptomatic adrenal insufficiency. 16 However, a 2011 study found that patients using glucocorticoids for only 1 week were at risk for subclinical adrenal insufficiency as shown through plasma cortisol levels. 15 A group of patients taking oral glucocorticoids for longer than 1 week were assessed for adrenal suppression by measuring their plasma cortisol response to CRH. Patients with normal responses were significantly more likely to have had a shorter course of glucocorticoids than patients with blunted responses. 15 Although longer duration of glucocorticoid use may be associated with a higher risk of adrenal suppression, most literature states glucocorticoid use up to 3 weeks is unlikely to cause significant adrenal suppression and thus these patients are considered low risk.7,17
Medications
A number of medications can alter the serum levels of corticosteroids and thus the potential for adrenal insufficiency (Table 3). Corticosteroids can also alter serum levels of other medications, which may increase potential toxicity. These key medication interactions include increasing serum levels of immunosuppressive drugs such as cyclosporine while decreasing serum levels of anti-inflammatory drugs such as salicylates and antituberculous therapies such as isoniazid. 7 In addition, medications may also independently carry a risk of adrenal suppression, and extra caution must be taken when prescribing them to patients on glucocorticoid therapy. Medications in this category include anticoagulants (heparin, warfarin), tyrosine kinase inhibitors (sunitinib), trilostane, phenobarbital, phenytoin, rifampin, troglitazone, mifepristone, chlorpromazine, imipramine, etomidate, and antifungals (ketoconazole, fluconazole). 18 Identifying medications that have been associated with adrenal insufficiency may help risk-stratify patients when discontinuing glucocorticoids to prevent adrenal insufficiency.
Medications That Affect Corticosteroid Potency and Thus Risk of Adrenal Suppression. a
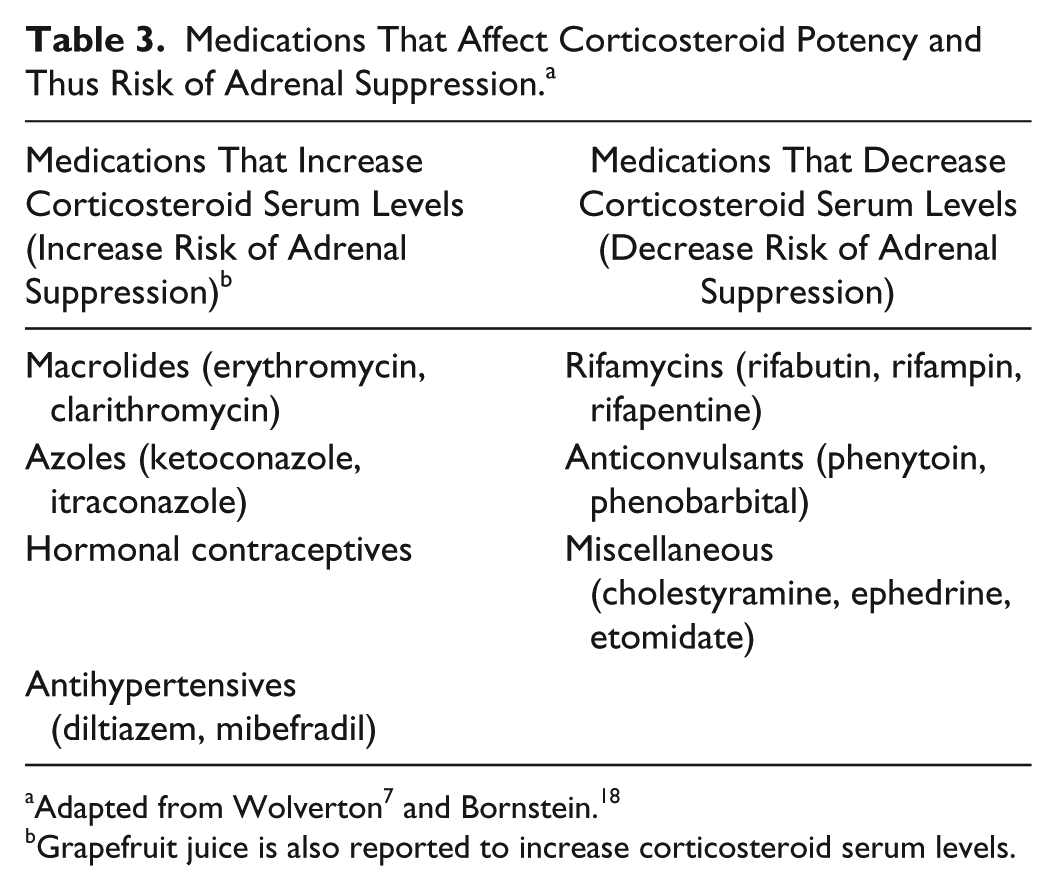
Grapefruit juice is also reported to increase corticosteroid serum levels.
Illness
Illnesses such as Waterhouse-Friderichsen syndrome (most commonly associated with meningococcal infections), 19 congenital abnormalities, 20 and infiltrative diseases including sarcoidosis, 21 amyloidosis, 22 and hemochromatosis 23 may present with primary adrenal insufficiency and thus make a patient at higher risk for more severe adrenal suppression when glucocorticoids are added. In addition, any severe illness or infection can cause adrenal crisis in patients on glucocorticoids due to the increased demand on the adrenal glands. 24
Confirming Adrenal Suppression
Dermatologists should consider ruling out adrenal suppression in their patients on chronic glucocorticoid therapy just prior to tapering below physiologic corticosteroid doses. 25 Many dermatologists opt to forgo confirmation tests and instead rely on patient symptoms of either a flare of their dermatological disease or of adrenal suppression. However, due to the risk of subclinical adrenal suppression, if relying on patient symptoms rather than confirmation testing, it is important to understand that the adrenal glands may be suppressed. Clinically, this may mean that patients with unconfirmed adrenal suppression could require stress dosing, discussed below, during times of illness or surgeries soon after stopping glucocorticoids. To confirm adrenal sufficiency in this population group, particularly patients with other risk factors for adrenal suppression, basal serum cortisol levels and adrenocorticotropic hormone (ACTH) stimulation testing can be used.
Measuring serum or salivary cortisol prior to 8
The standard high-dose ACTH stimulation test involves the use of 250 µg ACTH followed by measurement of serum cortisol 30 or 60 minutes after administration to assess adrenal suppression. Serum cortisol levels of greater than 500 nmol/L or 550 nmol/L have been used to confirm adrenal sufficiency with excellent specificity, although the sensitivity of this test is inadequate to rule out adrenal suppression. 28
The use of a low-dose 1-µg ACTH stimulation test was thought to provide a more physiological plasma concentration of ACTH and thus theoretically be more accurate in diagnosing adrenal insufficiency. Although supported in earlier studies,29,30 both 1-µg and 250-µg ACTH stimulation tests have since been shown to have similar diagnostic accuracy in ruling in secondary adrenal insufficiency. 28 Some clinicians may still prefer to use the 1-µg ACTH stimulation test after long-term glucocorticoid use due to the idea that adrenal glands with moderate atrophy may not respond adequately to 1 µg ACTH but will still respond well to 250 µg ACTH.
Other tests of the HPA axis exist, such as insulin hypoglycemia, metyrapone, and corticotropin-releasing factor; however, these tests are cumbersome and would generally be performed in consultation with an endocrinologist. 7
An Approach to Discontinuing Glucocorticoids
An approach to deciding on whether to discontinue corticoids abruptly or by weaning off slowly is described in Figure 2.
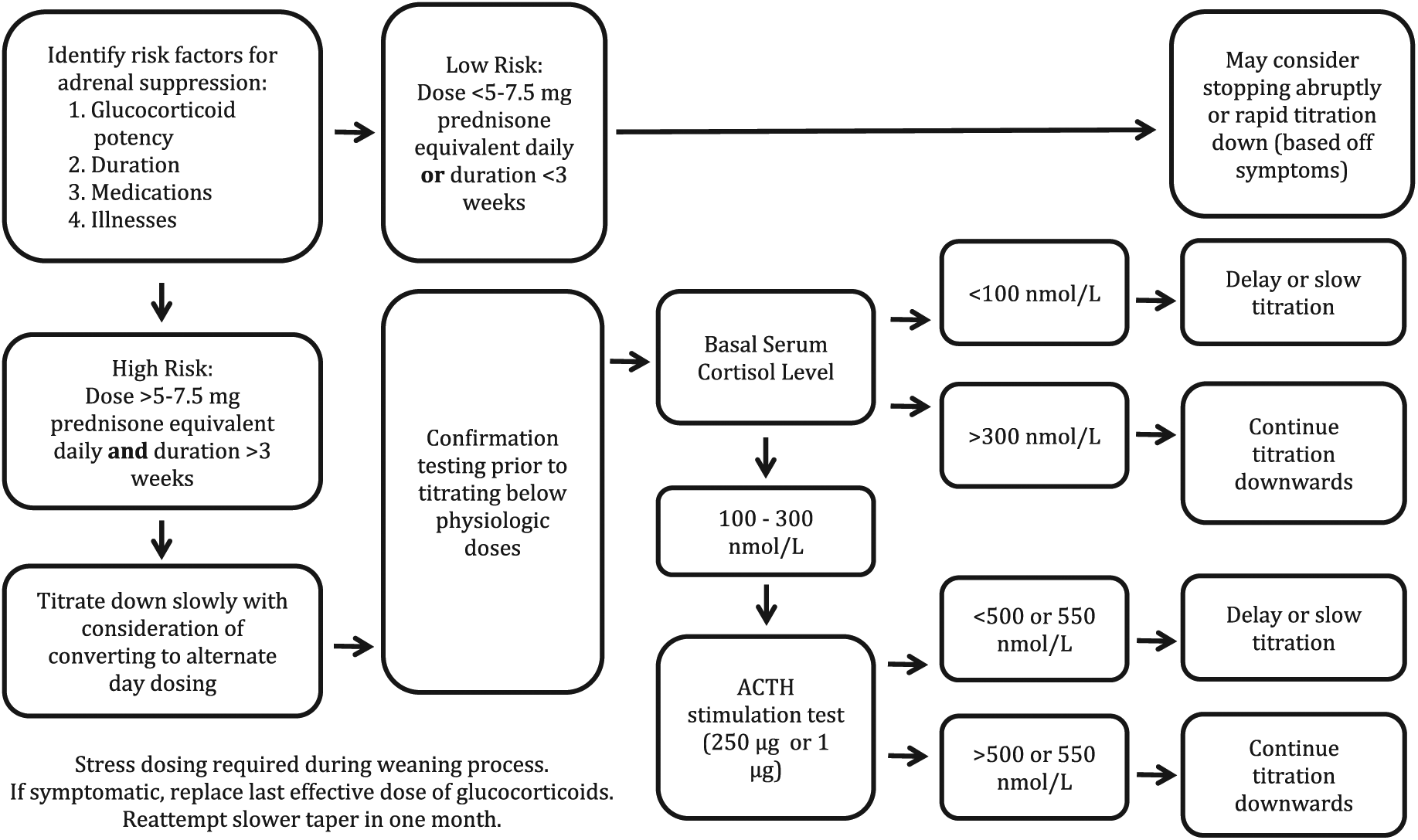
Approach to discontinuing glucocorticoids. ACTH, adrenocorticotropic hormone.
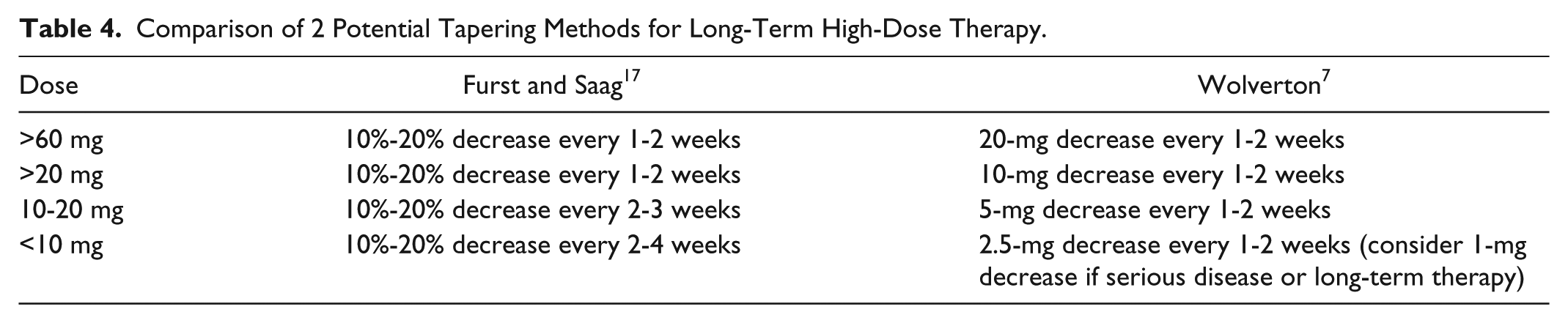
As Figure 2 shows, there are many situations where it is advisable to slowly wean or taper patients off glucocorticoids. Different tapering methods have been published in literature (Table 4); however, there is no consensus on the optimal way in tapering glucocorticoids. A 2013 systematic review of glucocorticoid tapering methods in rheumatoid arthritis looked at 6 randomised controlled trials, each with different tapering methods. 31 Methods varied and either decreased glucocorticoids by a set consistent amount over a set duration or decreased glucocorticoids by a percentage of overall dose over a set duration. Overall, the percentage of patients able to taper successfully was lower in patients with longer duration of disease. 31
Comparison of 2 Potential Tapering Methods for Long-Term High-Dose Therapy.
A general principle in discontinuing glucocorticoids is to titrate down slowly and not by large amounts. A 2016 study looked at 124 patients with pemphigus vulgaris on glucocorticoids who successfully titrated down their dosage of glucocorticoids while remaining symptom free. 32 After an initial tapering period, patients would reduce their glucocorticoid dose on average by 50% every year to an end point of 10 mg/d prednisone equivalent or less within 3 to 6 years. Using this slow tapering method, approximately 84% of patients experienced no flares of their disease during the course of titration. 32 The use of slow tapering of glucocorticoids may be helpful in preventing disease flares in dermatology patients. To help facilitate tapering of glucocorticoids without disease flares, dermatologists should use steroid-sparing oral medications and/or nonsystemic glucocorticoids such as topical formulations whenever possible.
Conversion to Alternate-Day Dosing
The main reason supporting conversion of patients to alternate-day dosing is the idea that alternate-day dosing causes less HPA axis suppression due to the glucocorticoid anti-inflammatory effect lasting longer than its suppression on the adrenal glands. Clinicians should consider converting patients on long-term glucocorticoids once disease control is largely attained on daily dosing and the use of intermediate-duration corticosteroids such as prednisone is being used. 7
Furst and Saag 17 recommend a conversion to an alternate-day regimen by decreasing the alternate-day dose first by 5 mg prednisone equivalent every 1 to 2 weeks until 10 mg prednisone equivalent and then decreasing by 2.5 mg prednisone equivalent every 1 to 2 weeks until the alternate-day dosing reaches 0 mg. The remaining drug is reduced in the same manner at that time. However, Wolverton 7 states that this method has the lowest chance of successful conversion to alternate-day therapy. This author instead proposes 2 other options for transitioning a patient to alternate-day therapy. The first option consists of multiplying the first day by 2 (or 2.5 for serious disease) while stopping the second day dose immediately. The second option consists of increasing the first day by a gradual amount while decreasing the second day by a similar gradual amount (consider 5-mg prednisone equivalent increments each day) until the second day dose is 0 mg. 7
If patients start having symptoms of their dermatologic disease during the tapering process, they should be restarted at the last effective dose when the dermatologic disease was well controlled. Dermatologists should then wait for the disease status to be well controlled again prior to tapering and should consider tapering more slowly than previously.
If at any time a patient shows signs and symptoms of adrenal insufficiency, replacement of the last effective dose of glucocorticoids when the patient was asymptomatic is recommended. 33 Glucocorticoid tapering may be reattempted after 1 month. The use of basal serum cortisol levels and the ACTH stimulation test could be considered to confirm adrenal sufficiency prior to reattempting the tapering process but is not commonly done in clinical practice and unlikely to alter management. It is crucial to advise patients about stress dosing glucocorticoids during this time and while they are titrating down their doses. 33
Stress Dosing
A common practice of giving patients on glucocorticoids an increased dosage of glucocorticoids during times of severe illness, commonly referred to as “stress dosing,” is done to prevent these adrenal crises. Different stress dosing protocols have been suggested for patients, including ones based on severity of illness. 34 For mild illnesses such as viral illnesses, urinary tract infections, cellulitis, or moderate illnesses such as gastroenteritis, pneumonia, or pyelonephritis, a simple “3 × 3 rule” has been proposed suggesting that patients on long-term glucocorticoids should triple their dosage for 3 days during illness. Severe infections, such as ones that require hospital admission like pancreatitis and myocardial infarctions, can require intravenous hydrocortisone from 75 to 200 mg/d depending on infection severity. 34 Stress dosing is also used perioperatively based on the required surgery’s severity. 34 In dermatology, skin biopsies under local anesthetic are classified as minimal surgical stress procedures, and patients should take their usual glucocorticoid dose without increasing. 34 It is important to discuss with patients the need for stress dosing during times of physiological stress. In addition, consider advising patients on long-term glucocorticoids to carry a Medic Alert product or a wallet card that identifies them as being on glucocorticoids.
Conclusions
Glucocorticoids are used commonly in dermatology to help alleviate disease symptoms, but their use creates a risk of side effects such as adrenal suppression. Acute adrenal crises secondary to glucocorticoid withdrawal are a potentially fatal complication but can be avoided with proper identification of risk factors and confirmation of adrenal suppression through various laboratory tests. We have presented in Figure 2 an approach for dermatologists to decide how to taper patients off glucocorticoids in a way that reduces the risk of adrenal insufficiency. Further research is required looking at optimal methods in weaning off glucocorticoids; however, general principles dictate slowly decreasing glucocorticoids over a long period of time with careful monitoring for symptoms of adrenal insufficiency.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.