
Abstract
Ulcerated infantile hemangiomas may present a therapeutic challenge, especially if there is concurrent hemorrhage or infection. The aim of this study was to systematically review the published evidence on the treatment of ulcerated hemangiomas, focusing on wound healing as the outcome of interest. We searched MEDLINE, Embase, SCOPUS, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Web of Science from inception to July 2016. Seventy-seven studies met our inclusion criteria. One study was a randomized controlled trial, 30 were observational studies, and 46 were case reports or case series. There is significant heterogeneity among the methods used. We reviewed 1239 patients in total. Of the 197 treated with oral propranolol, 191 (97.0%) achieved complete ulcer healing. Thirty-one patients failed corticosteroid therapy (oral, intralesional, or topical) and were subsequently successfully treated with other therapies. Surgical resections were typically performed for larger hemangiomas and those causing complications. None of the therapies discussed appear to offer significant advantages over others. Therefore, treatment decisions should be individualized based on location of disease, extent, symptoms, feasibility, cost, and parental preference.
Infantile hemangiomas (IHs) are the most common vascular tumours of childhood, with an incidence of 3% to 10% in all infants. 1 IHs are more commonly seen in females and in preterm infants. They typically exhibit a phase of rapid proliferation shortly after birth, followed by a phase of spontaneous involution that takes years to be completed. Most uncomplicated IHs do not require active intervention. However, ulceration is the most common complication seen in IHs, occurring in up to 15% of IHs.1,2 Ulceration is almost always an indication for intervention, as it can cause significant pain and increases risk of infection and scarring. 2
IHs can be described as superficial, deep, or mixed (having both superficial and deep components). Superficial and mixed hemangiomas are more likely to ulcerate, whereas deep hemangiomas rarely do. 3 Larger lesions and lesions located in areas frequently exposed to friction, such as the lip, neck, and perianal regions, are more prone to ulceration.4,5 IHs tend to ulcerate during the proliferative phase, and early white discoloration of a lesion is predictive of ulceration. 6
Ulcerated IHs may present a clinical challenge, causing functional limitations (eg, lip hemangiomas cause feeding difficulties), unrecognized infection, or poorly controlled pain. Ulcerated IHs in the perineum are particularly difficult to treat because of repeated contact with urine and stool. Currently, there are multiple options for treatment, which can be broadly categorized into wound care or conservative management, medical therapy, laser therapy, and surgery. The purpose of this study was to systematically review the published evidence on the treatment of ulcerated IHs, focusing on wound healing as the outcome of interest.
Patients and Methods
Search Strategy
Comprehensive literature searches were conducted from inception to July 2016 using each database platform’s command language and appropriate search fields, in the MEDLINE, Embase, SCOPUS, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Web of Science databases (Appendix S1). MeSH terms, EMTREE terms, and text words were used for the search concepts of ulcerated hemangiomas, wound care, surgical procedures, and drug interventions. No limits were applied. Because we reviewed all therapeutic interventions that have been used, a broad search strategy was necessary.
Inclusion and Exclusion Criteria
Only ulcerated IHs were included in the study, and other vascular tumours were excluded. Controlled trials, observational studies, case series, and case reports were included if the treatment modality was clearly described, and resolution of ulceration was an end point of the study. In studies where the primary indication for treatment was not ulceration (eg, other primary indications were obstruction or pain), studies were included if they included response of the ulceration to treatment. Exclusion criteria were (1) review articles, (2) no English language version available, (3) patients were over 18 years of age, (4) other types of vascular lesions that were analyzed within the same cohort as IHs, or (5) the outcomes of treatments were not clearly described in the results.
Data Extraction
Two reviewers independently conducted title and abstract screening. Conflicts were resolved through discussion between the reviewers. Data were abstracted from full-text manuscripts by 1 reviewer and double-checked for accuracy by a second reviewer. Data were collected on patient demographics; lesion morphology and characteristics; treatment modality, duration, and outcome; adverse events; and relapse of disease. In studies that examined both ulcerated and nonulcerated lesions, we extracted only the data for ulcerated lesions. Complete healing was defined as complete reepithelialization of the affected area. To assess bias within each study, we defined the level of evidence for each study using the Oxford Centre for Evidence-Based Medicine (CEBM) method.
Analyses
Data analyses were descriptive. The primary end point we assessed was time to complete reepithelialization of ulceration. In consideration of the significant variability in severity of ulceration amongst studies, we have not suggested a timeframe to define therapeutic failure. To obtain total numbers of patients receiving each treatment modality, we have pooled patients from multiple studies. A meta-analysis was not performed, as there were an insufficient number of comparative studies.
Results
Study Selection
Our first search for articles from inception to January 2016 generated 9134 studies. When the search was repeated for studies published between January and July 2016, we retrieved 516 additional results. Following title and abstract screening, we selected 138 studies for full-text review and ultimately included 78 studies in our analysis1-4,7-81 (Figure 1).
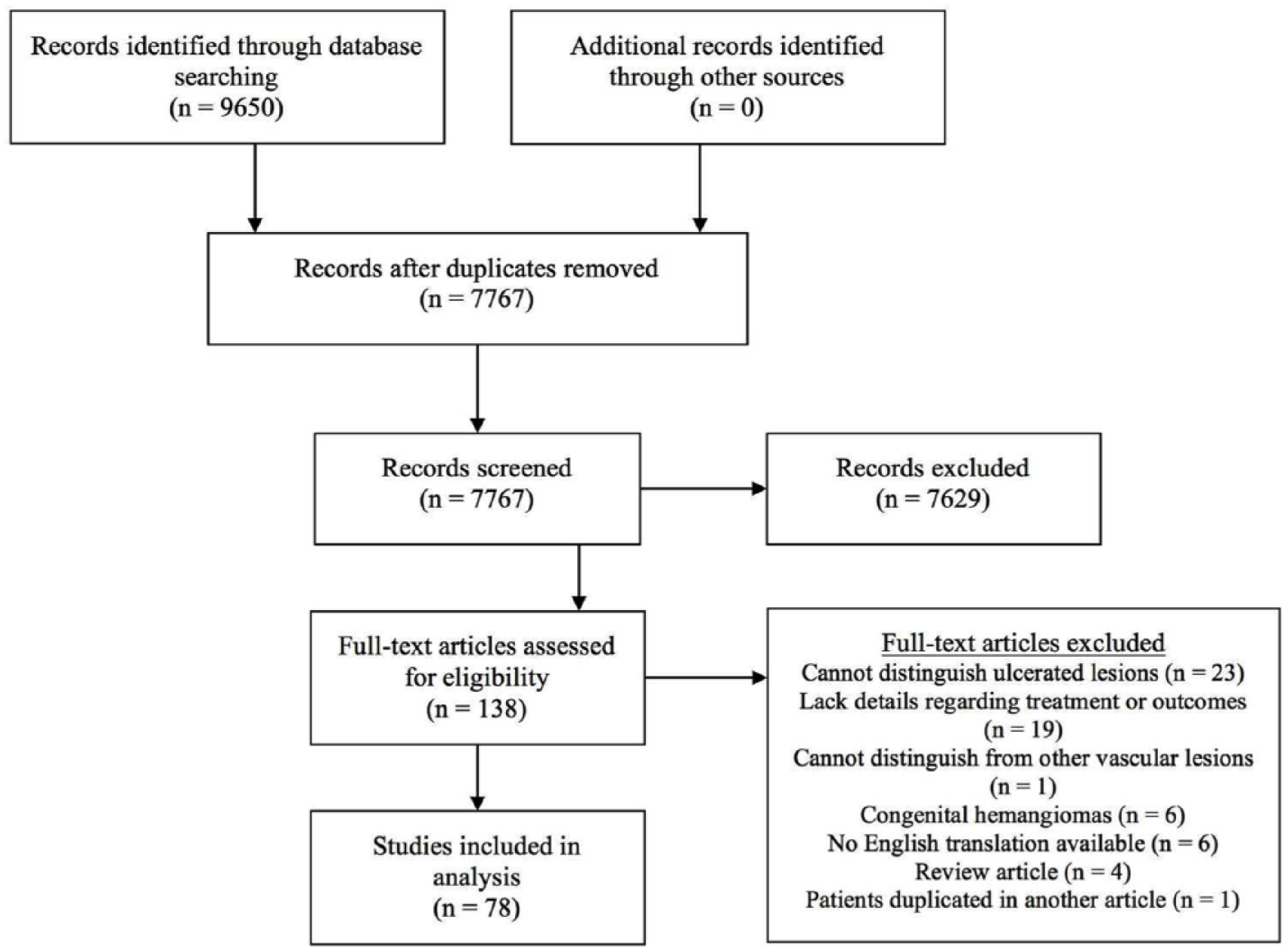
PRISMA flow diagram of study selection process. n = number of studies.
Overview of Studies
Among the 78 studies, 46 were case reports or case series, 16 were retrospective observational studies, 15 were prospective observational studies, and 1 was a randomized controlled trial (RCT). The RCT represents CEBM level 2b evidence, 7 while all other studies represent level 4 evidence, as there are no comparator groups. It is recognized that the degree of bias in these observational studies is inherently high due to the lack of comparators.
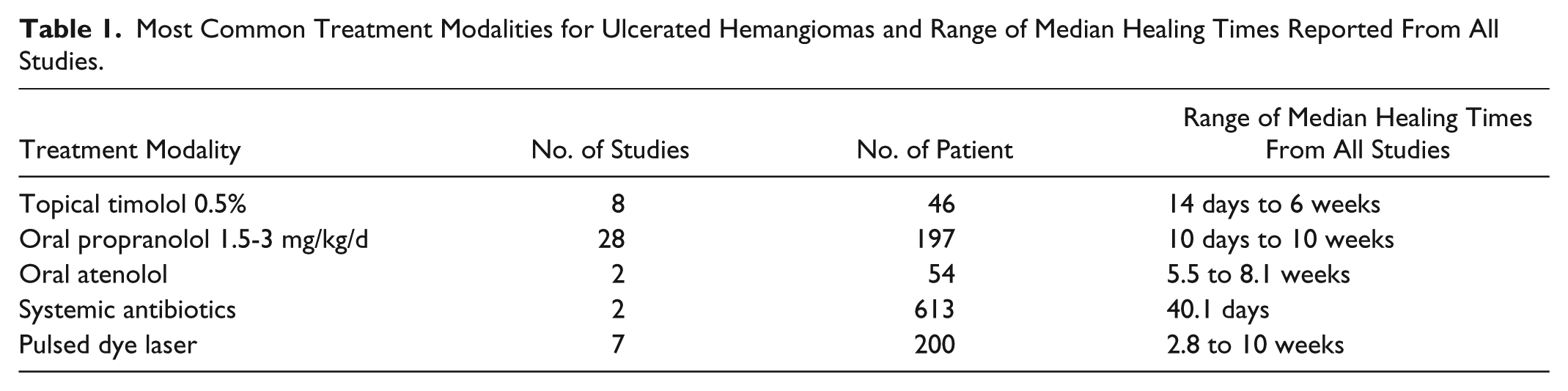
The 5 treatment modalities best described in the literature are topical timolol, oral propranolol, oral atenolol, systemic antibiotics, and pulsed dye laser. The range of median healing times from all studies using these modalities is summarized in Table 1.
Most Common Treatment Modalities for Ulcerated Hemangiomas and Range of Median Healing Times Reported From All Studies.
Systemic Therapy
Twenty-eight studies used oral propranolol as the primary treatment modality. The range of dosing used was 1.5 to 3 mg/kg/d, divided into twice daily or 3 times daily dosing. Amongst the 197 patients treated with propranolol, 191 (97.0%) achieved complete wound healing. Saint-Jean et al 8 (n = 33) used doses of 2 to 3 mg/kg/d and reported a mean healing time of 5.7 weeks. Tiwari et al 7 (n = 28) used doses of 2 mg/kg/d and reported a mean healing time of 17.9 ± 2.2 days of uninterrupted treatment. Time to healing for all other studies is reported in Appendix S2. In our review, there were no reports of epithelialized lesions becoming ulcerated while on propranolol therapy. Of these 191 patients successfully treated with propranolol, 10 had previously been trialed on systemic corticosteroids and experienced no wound healing or incomplete healing.2,8-12 Hyperkalemia was reported in 3 patients, although none were severe enough to necessitate discontinuation of therapy.13-15 In 1 case, laboratory tumour lysis syndrome due to propranolol therapy was diagnosed on the basis of hyperkalemia and hyperphosphatemia in the absence of clinical symptoms. 13
Two studies reported the use of atenolol for ulcerated IH. Ji et al 16 used atenolol 1 mg/kg/d, supplemented with oral antibiotics in 9 patients. They reported a mean healing time of 5.5 weeks. Ruitenberg et al 17 (n = 45) used atenolol at a mean dose of 1.3 mg/kg/d for a mean duration of therapy of 45.5 weeks. The mean healing time was 8.1 ± 6.6 weeks. However, 5 of their 45 patients had recurrence of the ulceration after discontinuation of therapy. 17
Tan et al 18 treated 5 patients with captopril 1.5 mg/kg/d divided in 3 doses. All ulcers healed in less than 3 weeks. One patient experienced a mild, transient elevation in serum creatinine.
Corticosteroids were used as primary treatment modalities in only 3 studies. Hasan et al 53 used intralesional triamcinolone 4 mg/kg, 2 doses, 5 weeks apart, in 1 patient. This ulcer resolved in 5 weeks. Strand and Smidt 75 used oral prednisolone 3 mg/kg/d in 1 patient, which produced ulcer healing in 1 month. Thomas et al80 used systemic steroids combined with pulsed dye laser in 2 patients. These lesions healed in 6 weeks and 9 weeks, respectively. More interestingly, amongst all of the patients in our analysis, 21 failed oral steroids,2,8,9,11,18-26 3 failed intralesional steroids, 19 and 7 failed topical steroids.9,22,27-30 Steroid therapy often produced lesion shrinkage but failed to produce ulcer healing. All 31 were subsequently treated successfully with other therapies.
Topical Therapy
Pandey et al 3 treated 608 patients with topical antibiotics for smaller ulcerations or both topical and systemic antibiotics for larger ulcerations (>10 cm2). The mean time to healing was 40.1 days (range, 16-96 days). Antibiotics were initiated based on history and clinical suspicion alone; wound cultures were not performed consistently. Three other studies, in which antibiotics were used as adjunctive therapy, performed wound cultures prior to antibiotic treatment.7,15,27
Topical timolol was used in 8 studies. Seven studies used a 0.5% solution or gel, applied 1, 2, or 3 times daily, and 1 study used a combination solution, containing brimonidine 0.2% and timolol 0.5%, applied twice daily. Of the 46 patients treated, 39 (84.8%) responded, 6 required transition to oral propranolol, and 1 required surgical resection. Mean healing time reported for a cohort of 9 patients (Weibel et al 31 ) was 14 days. Weibel et al 31 measured urine levels of timolol in 6 of their 9 patients. All 6 samples were positive, but no clinically significant adverse effects were observed. Blood levels were not drawn.
Topical becaplermin 0.01% gel, applied once daily, was used in 5 studies with a total of 21 patients. Nineteen patients experienced ulcer healing, 1 patient partially responded, and 1 was a nonresponder. McCuaig et al 81 (n = 9) reported a healing time range of 2 to 4 weeks. Metz et al 20 (n = 8) reported a median healing time of 13.5 days (range, 3-21 days). 20 Five patients had previously failed to improve on systemic corticosteroids.19-21
A single study of 2 patients reported that topical breast milk, applied once daily, used concurrently with propranolol, at 1 mg/kg/d, produced wound healing of ulcerated IH. 27 Both patients had previously been given propranolol 1 mg/kg/d, without topical breast milk, for 6 weeks and 1 week, respectively, with persistence of ulceration in both cases. After adding topical breast milk to propranolol, the first patient achieved wound healing at 4 weeks and the latter patient at 20 weeks. These healing times are not significantly shorter than those for propranolol therapy alone. Given the limited sample size, it cannot be determined whether topical breast milk is an effective adjunct therapy.
Laser and Light Therapy
Six studies used 585-nm pulsed dye laser alone, 1 study used 595-nm pulsed dye laser in combination with Nd:YAG laser, 32 and 1 study used multiple combinations of pulsed dye laser. 33 Energy fluencies ranged from 4.75 to 11 J/m2, and between 1 and 5 treatments were given at intervals of 2 to 4 weeks. Amongst these 8 studies, all 200 patients treated achieved reepithelialization of their ulcers. Morelli et al 34 (n = 37), using a 585-nm pulsed dye laser, reported a mean healing time of 2.84 ± 0.22 weeks. Li et al 32 (n = 22), using a pulsed dye laser combined with Nd:YAG lasers, reported a mean healing time of 13.5 ± 4.5 days. Kunzi-Rapp 79 (n = 7) used a combination of pulsed dye laser and oral propranolol. They reported a healing time of 1 to 2 weeks, which is amongst the shortest times reported.
Jorge et al 35 treated 2 patients with intense pulsed light and reported a mean healing time of 2 months. Achauer and Vander Kam 24 treated 10 patients with argon laser and reported a median healing time of 4 weeks.
Amongst all patients treated with laser and light therapy, new ulceration occurred at untreated sites in 5 patients.24,35,36
Surgery
Eight investigators performed surgical resections on 12 patients with ulcerated IH. In 5 of these cases, ulceration was the indication for surgery.29,37 The other indications were severe hemorrhage and progressive heart failure (n = 1), 38 risk of bleeding and permanent disfigurement (n = 1), 39 cosmetic (n = 1), 1 parental preference (n = 1), 40 and not reported (n = 2).41,42 One study used negative pressure wound therapy for wound closure, 41 and another used the TopClosure Tension Relief System (IVT Medical Ltd., Ra’anana, Israel), a noninvasive tissue expander. 39 No complications due to surgery were reported in any of the studies.
Wound Care
Only 1 study used wound care exclusively. Oranje et al 43 used polyurethane film for 8 cases of hemangioma less than 1 year old. The dressing was changed 3 times a day for the first 3 days and then once daily. All patients had a wound healing time of 2 to 7 weeks.
Other procedural and wound care therapies include ultrasound and negative pressure wound therapy. These therapies have little supporting evidence. Fox et al 30 treated 6 cases of ulcerated hemangioma with the combination of propranolol and negative pressure wound therapy.
Observational
Tiwari et al 7 were the only authors to report an observational arm. They conducted a randomized controlled trial, where the control group was ibuprofen and acetaminophen for pain control, and the study group was propranolol. The mean healing time for the control group (n = 24) was 27.71 ± 2.33 days.
Discussion
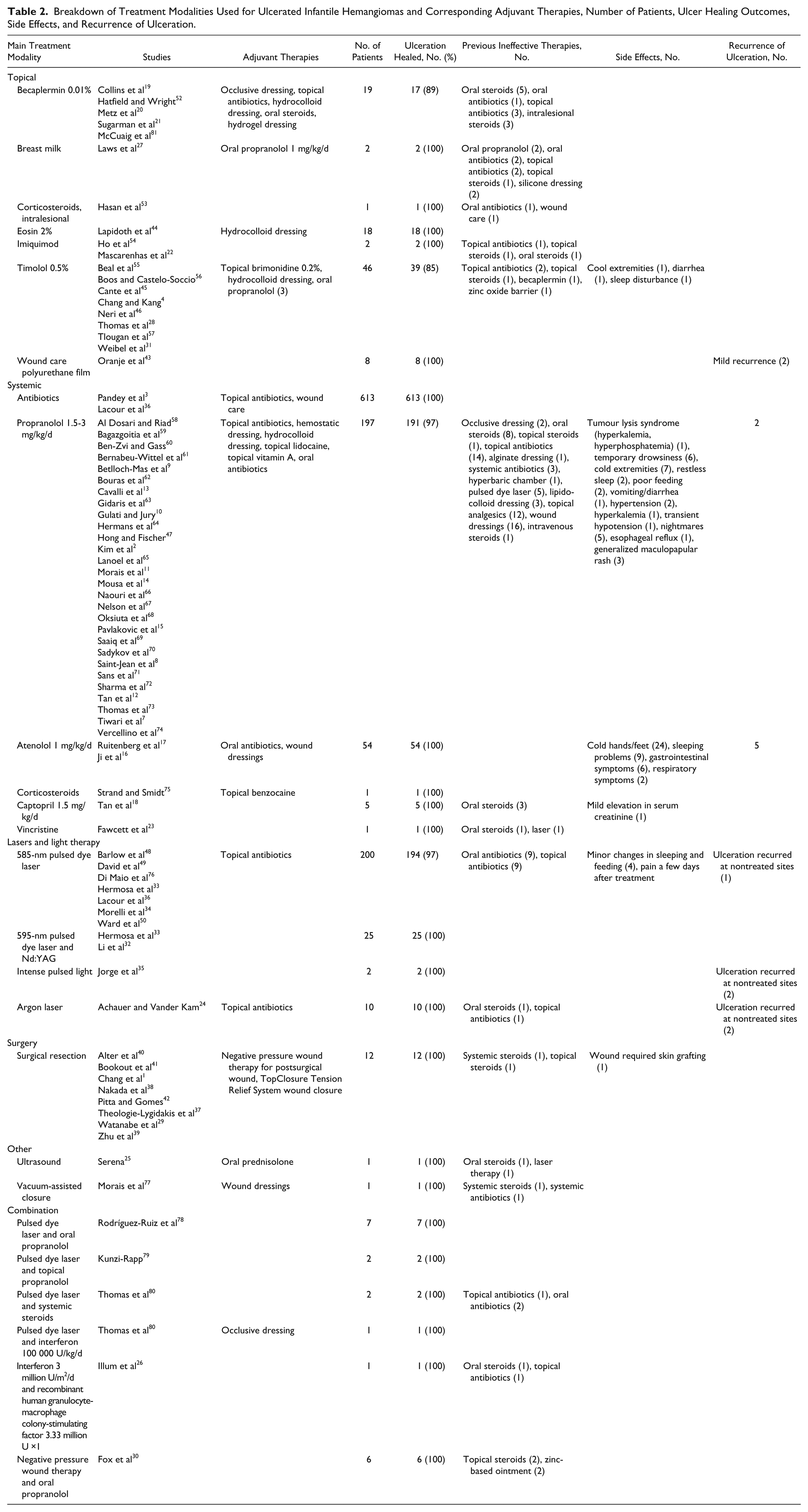
Of the 1230 patients reviewed in our study, 613 were treated with systemic antibiotics, 200 with pulsed dye laser, 197 with oral propranolol, 54 with atenolol, 46 with topical timolol, 25 with pulsed dye laser and Nd:YAG laser, 12 with topical becaplermin, 12 with surgical resection, 8 with wound care alone, 5 with captopril, 1 with vincristine, 19 with combination therapies, and 38 with other, less common, treatment modalities (Table 2).
Breakdown of Treatment Modalities Used for Ulcerated Infantile Hemangiomas and Corresponding Adjuvant Therapies, Number of Patients, Ulcer Healing Outcomes, Side Effects, and Recurrence of Ulceration.
In our analysis, propranolol was the most commonly selected systemic agent for ulcerated IH (28 studies). At a dose of 1.5 to 3 mg/kg/d, 191 of 197 (97.0%) wounds healed. Saint-Jean et al 8 (n = 33) were the only authors to use doses of 2 to 3 mg/kg/d. They reported a mean healing time of 5.7 weeks. Compared to other studies using a maximum of 2 mg/kg/d and shorter healing times, this limited evidence does not suggest that higher doses of propranolol promote faster healing. Pulsed dye laser was the most commonly used local therapy (8 studies). Four of the 8 studies that used pulsed dye laser analysis were published prior to 2008,24,34,36,48-50 before propranolol became a therapeutic option. Results were positive with all 225 (100%) wounds healed.
Studies of pulsed dye laser generally reported shorter mean healing times compared to studies of propranolol (Appendix S2). However, due to the heterogeneity in the methods amongst the studies, we cannot conclude whether these differences are significant. Additionally, there is a much larger range in the healing times reported for propranolol, in part because there were 28 studies of propranolol and only 8 studies of pulsed dye laser.
Topical timolol, currently available as a sterile 0.5% ophthalmic solution or gel, is an alternative β-blocker to propranolol. We found that topical timolol was preferentially used for smaller hemangiomas with smaller ulcerated surface areas, for which the benefits of oral propranolol did not outweigh the risks. Weibel et al 31 detected timolol levels in the urine of all 6 patients whom they tested, suggesting that some systemic absorption does occur.
Corticosteroids demonstrated unfavourable results in our analysis. We found a greater number of patients who failed corticosteroid therapy (n = 31) than patients who were successfully treated (n = 4). Corticosteroid use for IH has decreased in recent years, and our study supports this trend.
Surgical resections were typically performed for larger hemangiomas and those causing complications, such as suffocation, hemorrhage, or disfigurement, where it was deemed unsafe or inadvisable to wait for medical therapy to take effect.
Multiple investigators used topical or oral antibiotics as primary therapy and as adjuvant therapy (Table 2). Antibiotics should be reserved exclusively for IHs that have active infections.
The occlusion of wounds with atraumatic, nonadhesive dressings was the most commonly agreed-on management strategy between wound care experts dealing with ulcerated IH to help relieve pain and improve healing. These goals were achieved with multiple dressings, including silicone dressings and hydrocolloids, which were used in addition to other therapies in multiple studies.4,20,44-47 Debridement is not always necessary, and if needed, autolytic debridement is preferred. 51
Limitations
There are very few comparative studies published in this clinical area, and there is significant heterogeneity amongst the methods used in the observational studies we do have. It is therefore challenging to determine if any one therapy is truly superior in treating ulcerated hemangiomas. The natural history of infantile hemangiomas, which often spontaneously heal, also adds difficulty to interpreting the data. Furthermore, we recognize that publication bias, which favours the publishing of positive results, has limited the number of negatives studies we have available for analysis.
Conclusion
There was significant variability in the methods and outcomes of the studies we reviewed. None of the therapies discussed appear to offer significant advantages over others. Therefore, treatment decisions should be individualized and based on location of disease, extent, symptoms, feasibility, cost, and parental preference. We encourage future studies to conduct comparative analyses to determine which therapies are superior.
Supplemental Material
Heme_-_Appendix_-_10.21.17_clear – Supplemental material for Medical, Surgical, and Wound Care Management of Ulcerated Infantile Hemangiomas: A Systematic Review
Supplemental material, Heme_-_Appendix_-_10.21.17_clear for Medical, Surgical, and Wound Care Management of Ulcerated Infantile Hemangiomas: A Systematic Review by Jane Y. Wang, Arvin Ighani, Ana P. Ayala, Sadanori Akita, Irene Lara-Corrales and Afsaneh Alavi in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Alavi has been a speaker and consultant for AbbVie, Janssen, Novartis, Galderma, Valeant, and Leo. Dr Akita, Dr Lara-Corrales, Mr Ighani, Ms Wang, and Ms Ayala have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.