
Abstract

Patient decision aids (PDAs) are tools to engage patients in shared decision making by informing them of treatment options, associated risks, and benefits, as well as eliciting their preferences and values relevant to treatment. A PDA for psoriasis grounded in evidence-based clinical practice guidelines 1 was shown to reduce decisional conflict and improve patient knowledge. 2 This was recently updated to include newly approved treatments and was transformed into an online format.
Our objective was to assess the effectiveness of this updated psoriasis PDA. Participants were recruited through a dermatology practice in Windsor, Ontario, Canada. All provided written consent, completed a pretest survey, used the PDA, and attended a consultation with a dermatologist. They then completed 2 follow-up surveys (1 week [n = 11] and 4 weeks [n = 10]). The surveys assessed knowledge of psoriasis, treatments, decisional conflict, acceptability of the PDA, preparation for decision making, and decisional regret.
Participants were prepared to decide immediately after viewing the PDA (mean = 3.38, SD = 1.03). At follow-up, patients experienced very little decisional regret (mean = 15.0, SD = 12.25). A nonsignificant increase in total decisional conflict from pre- to posttest surveys was observed (Table 1), but these levels decreased by the 4-week follow-up (Table 2). Furthermore, there was a significant increase in knowledge from pre to post (P = .03), which was only marginally significant (P = .06) at the follow-up.
Results of t Tests and Descriptive Statistics for Decisional Conflict and Knowledge (n = 11).
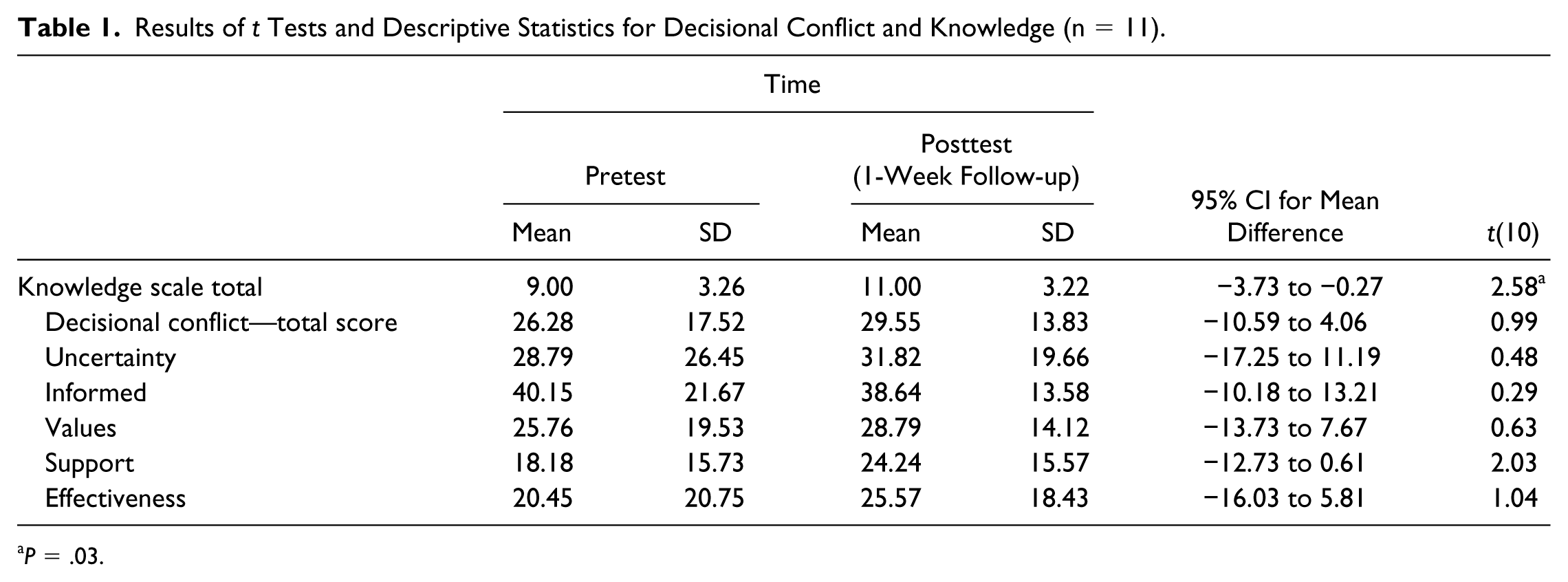
P = .03.
Results of t Tests and Descriptive Statistics for Decisional Conflict and Knowledge Scale (n = 10).
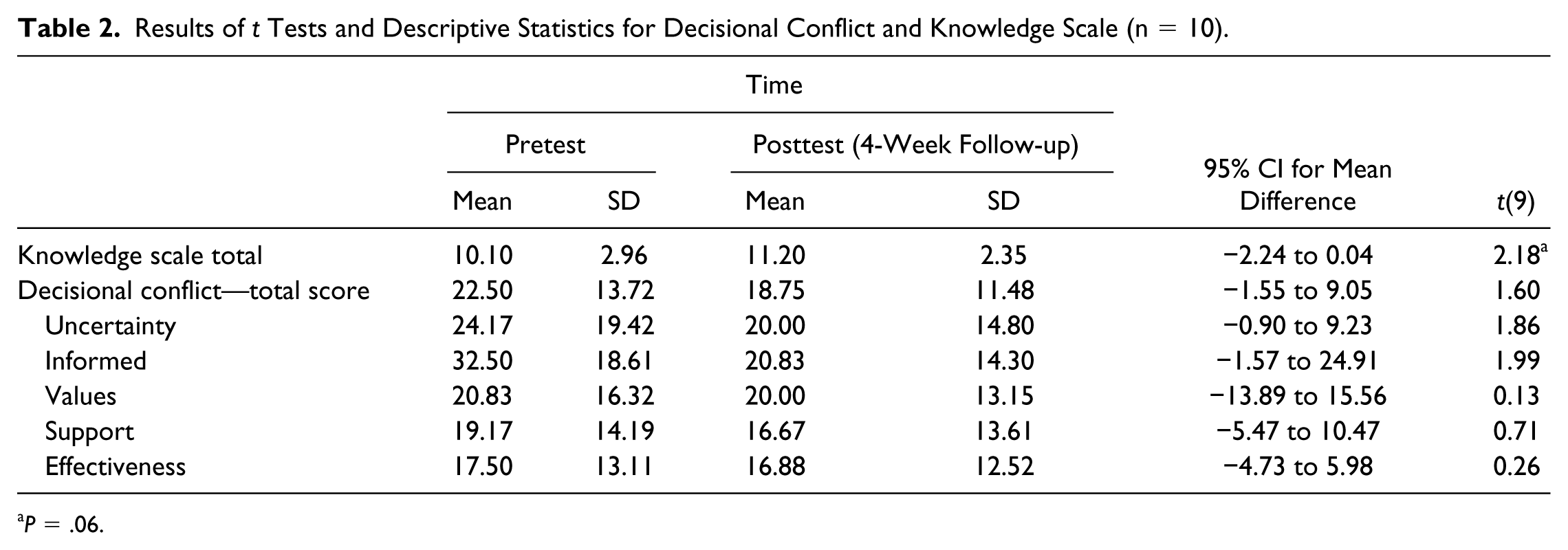
P = .06.
Most participants indicated that the PDA would help them decide (n = 7; 64%), made their decision easier (n = 9; 82%), and was an adequate length (n = 10; 91%) with the right amount of information (n = 10; 91%).
The PDA was successful in teaching patients new information. In an earlier study, 3 patients indicated a desire for more information; our findings suggest that we met this need. Surprisingly, the PDA did not significantly improve decisional conflict. This finding is likely due to the nature of our sample. First, decisional conflict scores were very low across all time points, suggesting the current patients experienced very little uncertainty from the beginning of the decision-making process. Second, since all participants had a history of psoriasis treatment, they had already been through the process of choosing a treatment. It is possible that pretest decisional conflict was quite low because they felt positively toward their current or previous treatments. By providing new information and prompting reflection on ones’ values, the PDA may have led to a temporary increase in conflict that the patient would have to reconcile. Indeed, decisional conflict scores decreased nonsignificantly at the 4-week follow-up.
Overall, participants responded positively to the PDA, reporting that it was appropriate in both content and length. Furthermore, most participants indicated that it was useful in helping them decide. Limitations of this study include a small sample size and lack of a control group. Future research should incorporate a larger sample for a randomized control trial of patients who are actively seeking treatment.
The current PDA shows promise for implementation. It was successful in increasing knowledge, with patients also reporting an acceptance of the PDA, moderate preparedness, and low decisional regret. The psoriasis PDA is online and accessible without cost at http://www.informed-decisions.org.
Footnotes
Acknowledgements
We thank Abbvie Innovation for focus group training and support, Toni Janek at Windsor Regional Hospital Library for research support, and Trackie for PDA web design.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Tan has been an advisor, clinical investigator, speaker, and/or received honoraria from Abbvie, Boehringer Ingelheim, Cipher, Dermira, Galderma, Novartis, Pfizer, Roche, Valeant, and Xenon. Dr Dellavalle has received grants, research, and clinical trial support from Pfizer, and provides medical consulting to Altus Labs in exchange for expense reimbursement and vestment in the company. Dr Dellavalle also has royalties from UpToDate and editorial stipends from the Journal of Investigative Dermatology and Journal of the American Academy of Dermatology.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Pfizer Independent Grant for Learning and Change and the American Academy of Dermatology (grant 24067701) and a Valeant Unrestricted Educational Grant.