
Abstract
Background:
The most common skin cancer is basal cell carcinoma (BCC), and the gold-standard treatment for high-risk tumours is Mohs surgery. However, alternative methods are needed for high-risk tumours in countries where the performance rate of Mohs surgery is low.
Objectives:
The objective of this article is to investigate the feasibility, efficacy, and safety of margin-controlled, staged surgical excision (MCSSE) in high-risk tumours as a possible treatment alternative.
Methods:
A retrospective cohort study, including patients diagnosed with high-risk BCC in the head and neck region and treated with MCSSE between 2003 and 2010, was conducted.
Results:
During the study period 50 tumours in 47 patients were treated, with low adverse event rates and high patient satisfaction rates. Of the 50 tumours, 1 recurred at the 12-month follow-up.
Conclusions:
Despite the small sample size and relatively short follow-up period, the present study shows that MCSSE might be a feasible alternative for the treatment of high-risk BCCs in institutions where Mohs surgery is not performed. Future studies on long-term recurrence rates are needed.
Introduction
Nonmelanoma skin cancer (NMSC), comprising basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), is the most common malignancy and has an increasing incidence anually.1-3 However, BCC is the most common and can be treated with a wide spectrum of modalities, depending on multiple variables related to the patient and tumour, such as the age of the patient, immunosuppression, location, size, histopathologic subtype of the tumour, and risk factors for recurrence.1,2
Considering that incomplete excision of the tumour is associated with increased recurrence rates, Mohs micrographic surgery (MMS) is the treatment of choice in high-risk BCCs to achieve tumour-free surgical margins.1,2,4,5 However, the proper implementation of MMS requires specialized training, and it may also pose an economic burden for many centres. Only 44 Mohs surgeons are registered in the European Society for Micrographic Surgery. Although studies on the subject are scarce, margin-controlled, staged surgical excision (MCSSE) was previously shown to be effective in treating high-risk BCCs6,7; thus, we believe that it might be a reliable and feasible alternative to MMS in centres or countries where MMS cannot be performed. The primary aim of the present study is to evaluate the feasibility, efficacy, and safety of MCSSE in high-risk BCCs in the head and neck region.
Patients and Methods
A retrospective cohort study was conducted in close collaboration with the dermatology, plastic surgery, and pathology departments. The study was reviewed and approved by our institutional ethics committee before patient enrolment. All patients signed an informed consent form.
Patients diagnosed with high-risk BCC in the head and neck region between 2003 and 2010 were included in the study.
Based on the National Comprehensive Cancer Network (NCCN) guidelines, tumours were stratified as high-risk BCCs in the presence of 1 or more of the following risk factors: poorly defined borders, recurrent tumours, tumours located on the site of previous radiotherapy, immunosuppression, aggressive histopathologic growth patterns (morpheaform, basosquamous, sclerosing, mixed infiltrative, or micronodular) or perineural involvement, tumours of any size in area H, and tumours > 10 mm and 20 mm in areas M and L, respectively (area L consists of trunk and extremities [except for hands, feet, pretibial region, and ankles]; area M includes cheeks, forehead, scalp, neck, and pretibial region; and area H includes central face, periorbital area, nose, lips, pre- and postauricular skin, ear, genitalia, hands, and feet).
Patients with coexisting serious medical conditions or who were high risk for anaesthesia or older than 85 years for whom repeated hospital visits and wound care would be bothersome were excluded from the study.
Dermatologic Evaluation
Demographic data, medical history, skin phototype, hair and eye color, sun exposure history, and sun protection behaviour of the patients were recorded. Size, localization, and clinical characteristics of the tumour and previous treatment methods in case of recurrent tumours were noted.
Clinical diagnosis and identification of histopathologic subtypes were confirmed by incisional or punch biopsy specimens obtained from all patients. The largest diameter of the clinically palpable tumour was recorded, and clinical photographs were obtained. Subsequently, the patients were referred to the plastic surgery department for MCSSE.
Surgical Treatment
Tumours were excised with 5-mm surgical margins under local anaesthesia. After the excision, tumour tissue was marked with a suture from its “superior,” “lateral,” or “medial” sections when needed. To specify the tumour localization, the marked sections of the tumour were indicated on a schematic facial illustration (Figure 1).
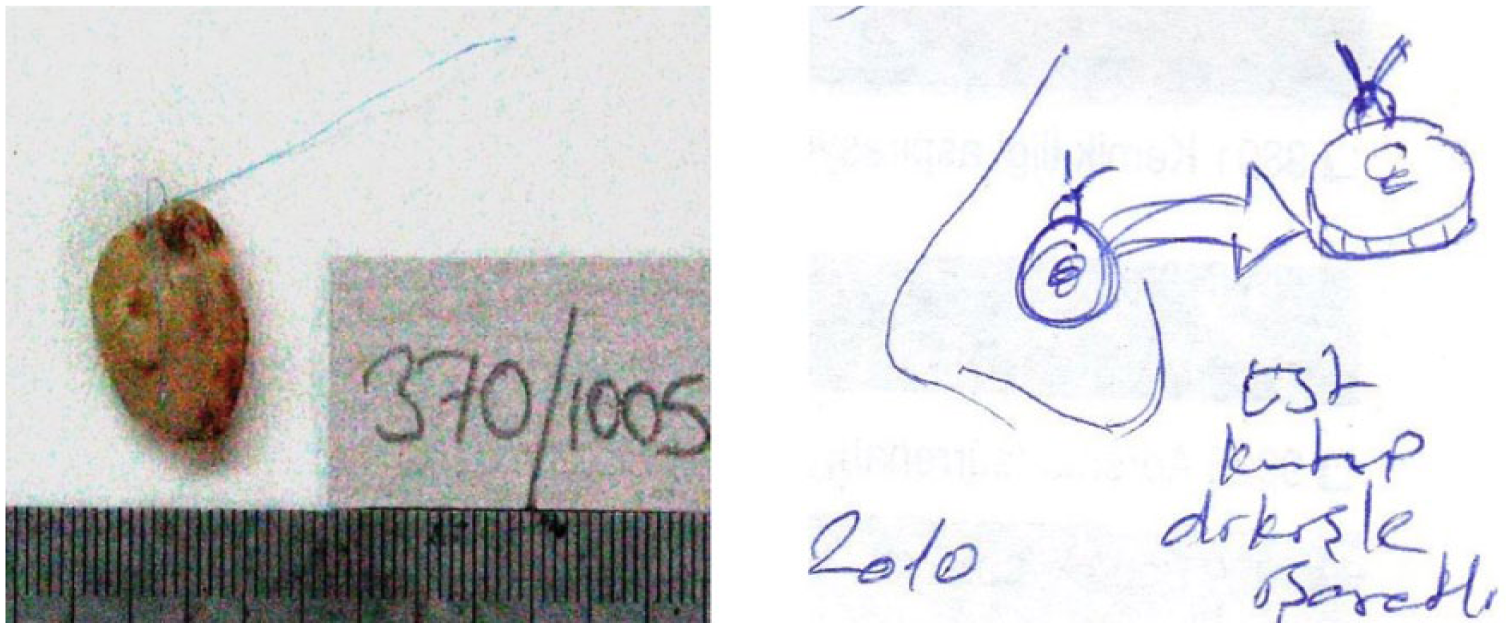
Mapping of the Excision Material on a Schematic Facial Illustration
Tissues fixated in 10% formaldehyde solution were submitted to pathology for a 2-day histopathological examination. The excision was advanced by 2 to 3 mm at each stage if the surgical margin was positive histopathologically. Each stage was at 2- to 4-day intervals. Prophylaxis with oral antibiotics was administered for delayed repairs. Only after all surgical margins were tumour free was the repair strategy established based on the size of the remaining defect. Before the repair, the defect was photographed and its largest diameter was recorded. The occurrence of surgical complications, such as bleeding or infection, was recorded at each stage.
Histopathological Examination
The excised specimen was examined by positioning the tissue based on the schematic facial illustration sent by the surgeon (Figure 2A). First, the tissue was divided into 2 pieces along the long axis. Subsequently, parallel sections sized 2-10 mm thick were made perpendicular to the long axis, proportionately to the size of the material (Figure 2B). Sections obtained from the excision material were numbered and mapped (Figure 2C). Vertical sections 2-μm thick were obtained from each section and examined microscopically. The excised tissue was mapped after repeating the surgical stages (Figures 2D and 2E). The surgical margin was considered positive if the tumour was present at the surgical margin or close to the margin by < 1 mm.
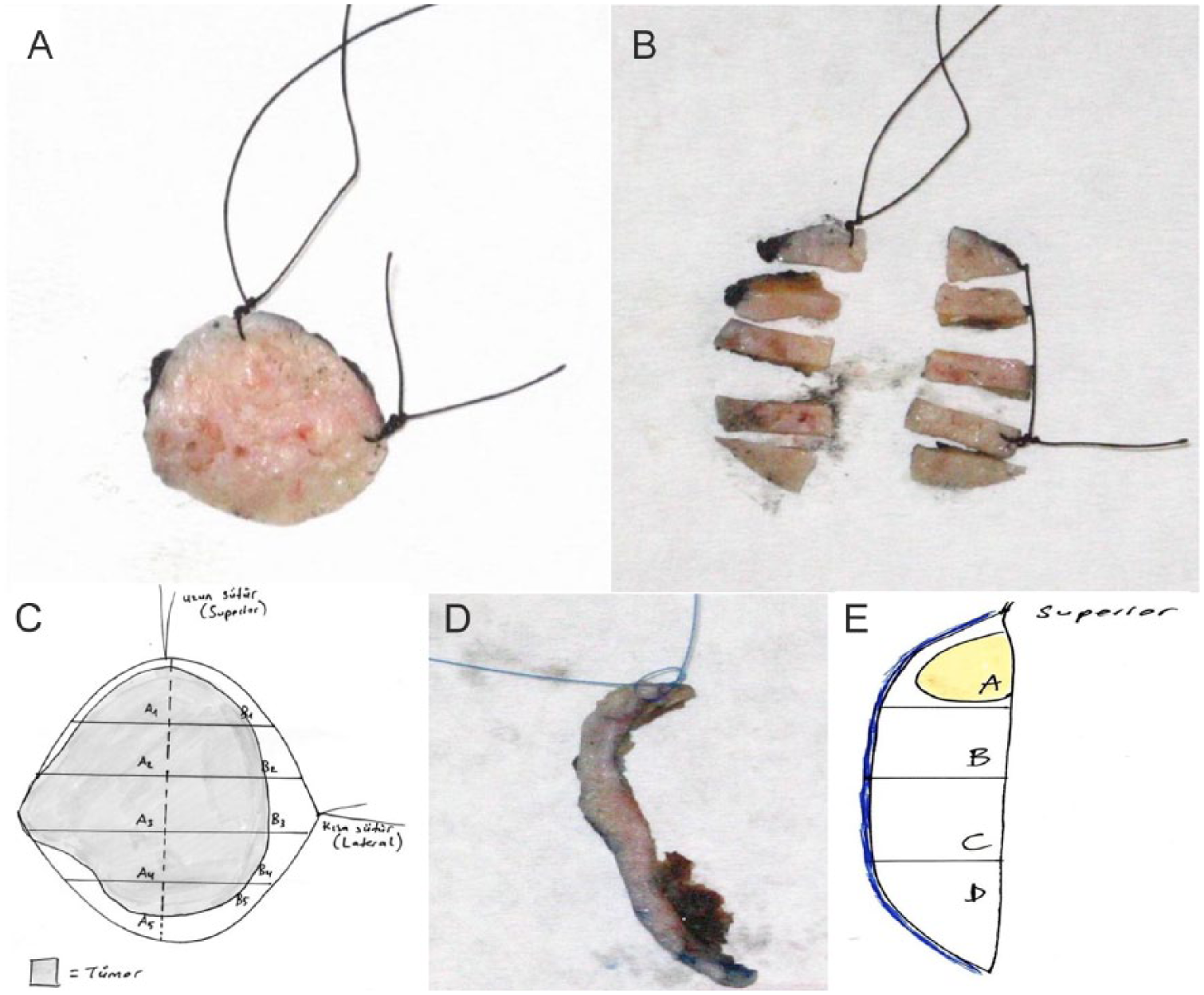
Histopathological examination of the excision material. A, Tissue positioning and B, tissue sectioning. C, The sections obtained are numbered and mapped. In repeated surgical stages, D, E, the excised specimen and mapping of the tumour on the material are shown.
Follow-Up
The patients were scheduled for a follow-up visit the first week after repair of the defect. Follow-up examinations were performed at the third, sixth, and twelfth months and once every 6 months thereafter in a dermatology outpatient clinic. The presence of any recurrence or development of a new primary skin cancer was recorded. During each follow-up visit, the surgery site was photographed. The patients were instructed to complete the patient satisfaction form (PSF) during the third month of treatment. The PSF consists of 4 Likert-type questions evaluating the difficulties experienced regarding hospital visits, wound care, and personal care/bathing throughout the treatment process and another question on whether the patients would choose the same treatment method again.
Statistical Analysis
Statistical analysis of the study data was performed using Statistical Package for Social Sciences (SPSS Inc, Chicago, IL, USA) v11.5 software. Descriptive analyses and frequency distributions of measurable and qualitative data, which can be expressed in numbers or numerical codes, were indicated with percentages and mean ± standard deviation. Follow-up duration, a continuous variable, was shown as median. To compare the means between independent samples, Student t-test was used for parametric data, and chi-squared and Mann–Whitney U-test were used for nonparametric data. A P value < .05 was considered statistically significant.
Results
Patient Characteristics
During the study period with MCSSE, 50 high-risk BCCs in 47 patients (23 women [49%], 24 men [51%]) were treated. The mean age of the patients was 63 ± 11.5 years (range, 32-85 years). Among the study population, 27 patients were younger than 65 years (57.5%). Skin phototype was determined in 45 patients: 34 (76%) and 11 (24%) patients had skin phototypes II and III, respectively. Of the 45 patients, 26 (56%) had light eye color. History of occupational or recreational and intense ultraviolet exposure was evident in 36 (80%) patients. None of the patients used sunscreens regularly.
Clinical Features
Of the 47 patients included in the study, 44 had a single high-risk BCC, whereas 3 had multiple lesions.
Of the 50 lesions treated with MCSSE, 44 and 6 were in high- and moderate-risk areas, respectively. The nasal region was the most commonly involved anatomic site, with 28 tumours. Table 1 shows the anatomic site distribution of the excised tumours.
Clinical, Histopathological, and Treatment Characteristics of Primary and Recurrent Tumours.
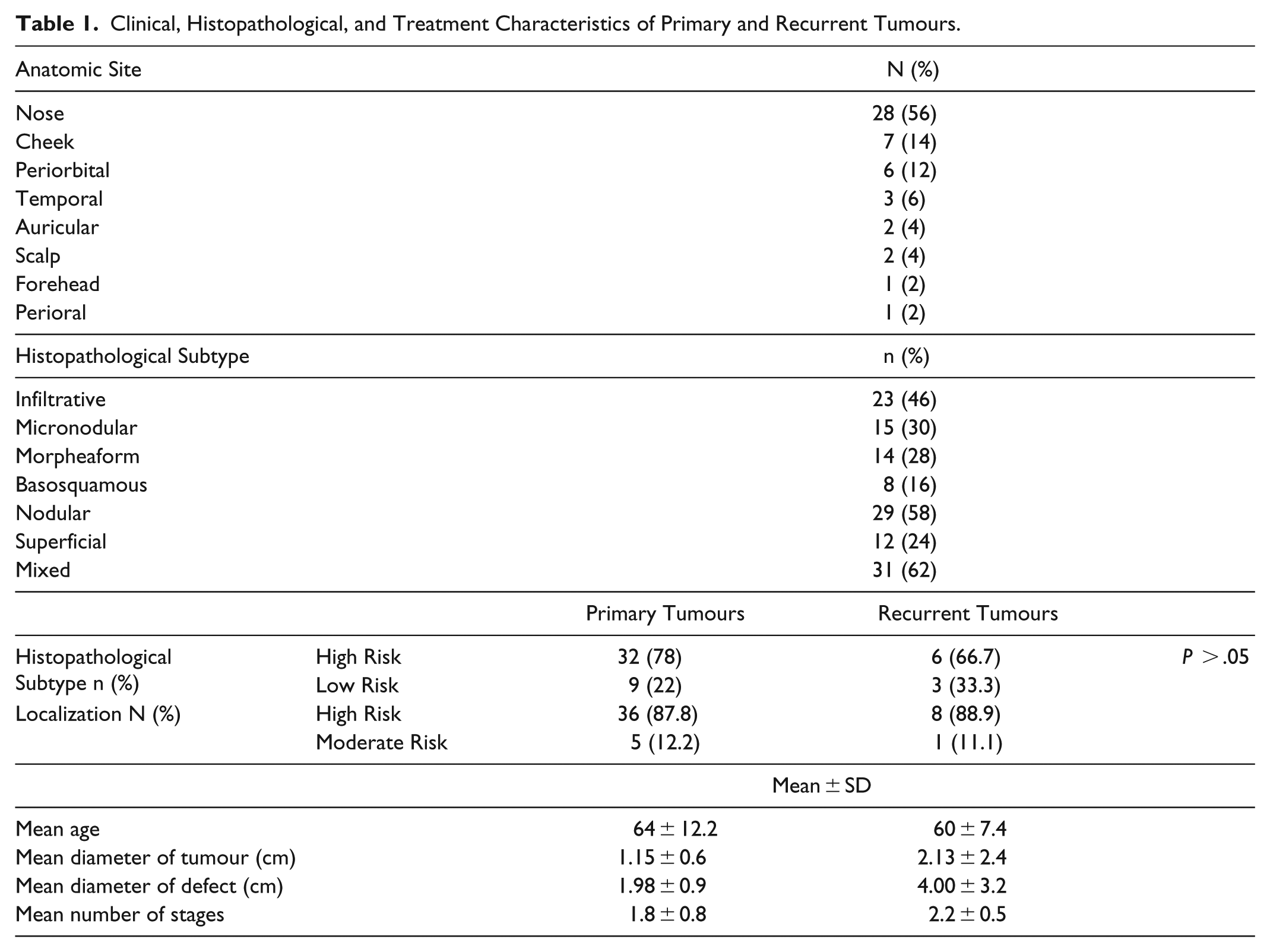
Evaluation for the presence of risk factors for recurrence showed 13 tumours had a single risk factor, whereas the remaining 37 tumours had 2 or more risk factors. Of the 50 tumours, 44 were in a high-risk area, 38 had an aggressive histopathologic subtype (morpheaform, basosquamous, infiltrative or micronodular), and 9 were recurrent lesions.
The mean tumour diameter of the 50 BCCs was 1.33 ± 1.2 cm (range, 0.3-8 cm). The diameter of the final defect after obtaining tumour-free margins was measured in all lesions. These lesions had a mean tumour diameter of 1.3 ± 1.4 cm, and the mean diameter of the tissue defect was 2.4 ± 1.7 cm (range, 0.5-10 cm). The mean free surgical margin required to achieve complete tumour removal was 1.1 ± 0.6 cm (range, 0.2-3 cm).
Of the 50 BCCs treated with MCSSE, 41 (82%) and 9 (18%) were primary and recurrent tumours, respectively. Although not statistically significant, the mean diameter of the final defect and the mean number of stages required to achieve complete tumour removal were significantly higher in recurrent tumours. Table 1 shows the clinical, histopathological, and treatment characteristics of the primary and recurrent tumours.
Histopathological Findings
Aggressive growth patterns (infiltrative, micronodular, basosquamous, morpheaform) were seen in 38 (76%) of the tumours; perineural invasion was seen in 7 of these. Histopathological subtypes of the tumours are summarized in Table 1. Additional subtypes on the excision specimen were observed in 21 of 30 tumours in which a biopsy was initially obtained. Three tumours did not show an aggressive growth pattern on biopsy; however, an aggressive histopathological subtype was seen upon examination of the excision specimen.
Comparing the presence of tumours showing high- and low-risk subtypes, no statistically significant difference was found between the nasal region and the other anatomic sites (P > .05).
Treatment Characteristics
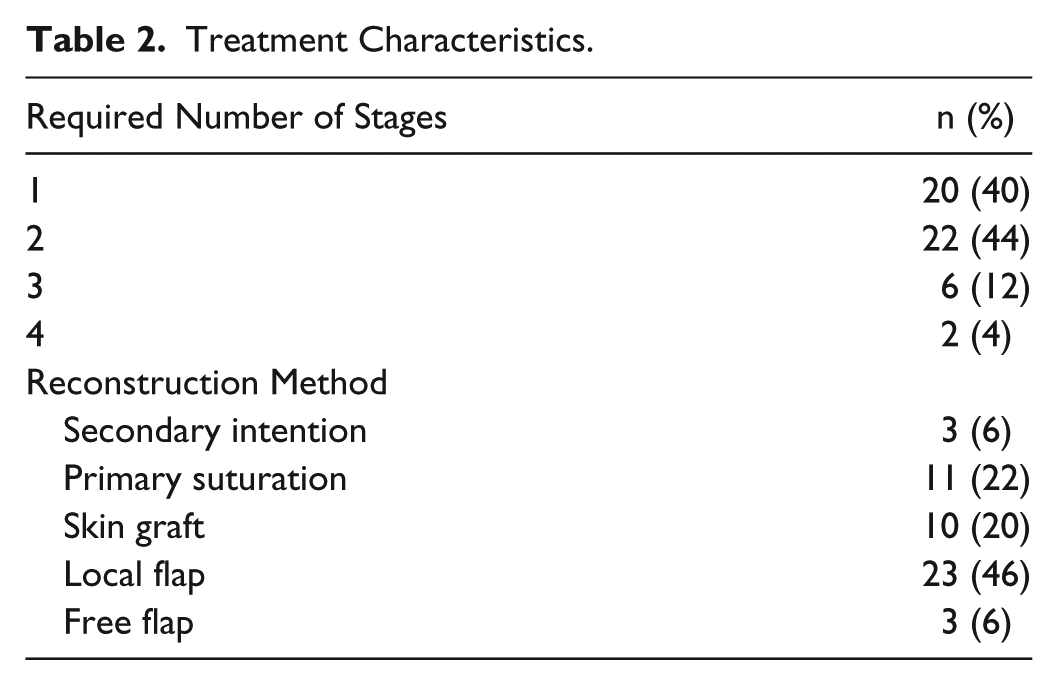
The mean number of treatment stages was 1.8 ± 0.8 per tumour. Of the 50 BCCs, 20 (40%) underwent 1 stage, whereas 2 or more stages were required for the remaining 30 (60%). No statistically significant difference was found between the lesions requiring 1 stage and lesions requiring 2 or more stages in terms of histopathological subtype, location, age, and tumour diameter (P > .05). The mean time between the first stage and the final repair was 4 ± 3.7 days (range, 2-21 days). No complication, including soft-tissue infection or bleeding, was seen during the study period. Table 2 shows the treatment characteristics and reconstruction methods.
Treatment Characteristics.
Patient Satisfaction
A total of 15 patients completed the PSF, with most of the patients not experiencing any difficulties during the treatment process. Only 2 patients experienced slight difficulty attending hospital visits frequently, and another 2 patients reported slight difficulty regarding wound care. Finally, 13 of the 15 patients would definitely choose the same treatment again, and the remaining 2 patients would choose the same treatment method despite slight difficulties.
Follow-Up
The patients were followed up for a median period of 24 months (range, 3-84 months). Of 50 tumours, only 1 lesion (2%) recurred 12 months after treatment.
The initial tumour pattern of this patient was morpheaform and infiltrative-type BCC in the lower eyelid. After the second MCSSE, the patient was followed up for 2 more years without any recurrences. However, a new primary BCC developed and was treated with MCSSE.
During the follow-up period, new primary BCCs were found in 7 patients (15%). Development of any other NMSCs was not observed within the follow-up period.
Discussion
In the present study, 50 high-risk BCCs in the head and neck region in 47 patients were treated with MCSSE. Our results demonstrated that MCSSE is a feasible surgical treatment method for high-risk BCCs and provides high patient satisfaction and low recurrence rates.
In accordance with the existing data, most of the patients in our study had fair skin, light eye color, and a history of intense ultraviolet exposure, but none had a genetic predisposing syndrome or immunosuppression. The median age at diagnosis for BCC is 68 years, which is similar to our cohort with a mean age of 63 years. 8
MMS remains the treatment of choice for high-risk BCCs with 5-year recurrence rates of 1% to 5.6%.2,9 Moreover, a randomized, controlled trial comparing MMS with standard excision in facial BCC reported a 10-year recurrence rate of 4.4% and 12.2% with MMS and standard excision, respectively. 10 Despite advantages of MMS, such as being a tissue-sparing surgical method and having low long-term recurrence rates, the major disadvantage in developing countries is the low utilization rate. 11 There is still a need for a tissue-sparing surgical method for high-risk BCCs in centres where MMS is not performed, which is similar to ours.
Similar to our method, Niederhagen et al treated 279 facial BCCs in 211 patients using staged surgeries with a 5-year recurrence rate of 3%. Of the 279 BCCs, 88 were recurrent tumours, but the researchers did not further classify the tumours as low or high risk. 6 Similarly, Hüsler and colleagues reported a recurrence rate of 3.6% after a median follow-up of 58 months. 7 Although the follow-up period in the present study is relatively shorter, the 2-year recurrence rate was 2%. This could be explained because our study included only cases of high-risk BCCs. Another study investigating our cohort’s long-term results has also been conducted. In the study by Niederhagen et al, more than 1 stage was required in only 18% of tumours to achieve tumour-free margins. 6 However, in our study, 60% of the tumours had 2 or more excisions with a mean stage number of 1.8. This discrepancy may also be attributed to our study population, which comprised only high-risk BCCs. In the other study, Hüsler et al treated 228 patients with staged surgical therapy. Similar to our results, the mean number of stages per tumour was 1.8, and 2 or more stages were required for 60% of the tumours. 7 Nizamoglu and colleagues have treated 69 patients with NMSC using a frozen-section, margin-control technique. After a mean 1.3 stages of excision, complete excision was obtained in 98% of the patients and there was no recurrence at first year follow-up. 12 Moreover, 2 studies have utilized formalin-fixed tissue Mohs surgery, also referred to as slow Mohs, in patients with BCCs. They have reported 5-year-recurrrence rates of 0.58% and 2.8%, which are comparable to MMS.13,14
Skin flap, skin graft, or free radial forearm flap was used for the final repair. In MCSSE, the final size of the defect might be discrepant from the clinically perceived size of the tumour; hence, the physician should be experienced enough to perform any repair method based on the resulting defect. The initial surgical margin of 5 mm and subsequent stages might have resulted in more tissue defect compared with MMS. The initial surgical margin may be lowered for less tissue defect in future studies.
The primary aim of this study was to investigate the feasibility of MCSSE. In general, the patients and medical staff were pleased with the treatment process throughout the study period. The patients were instructed to complete the PSF to further evaluate the patients’ perspective on the treatment; however, only 15 patients completed the questionnaire. Although our study was conducted with the cooperation of 2 centres 20 km apart, only 2 patients reported slight difficulty regarding hospital visits. MCSSE was well tolerated by most of the patients without any complications. Despite the majority of the patients undergoing more than 1 surgical excision, we believe that a relatively short period of 4 days from first stage to final repair could be a major satisfying factor for patients. Overall, 15 patients who completed the PSF stated they would choose the same treatment method again.
Although the present study has successfully demonstrated that MCSSE is an important alternative in areas where Mohs surgery is not performed, it has certain limitations because of the relatively small sample size and lack of long-term follow-up for recurrences. Other research focusing on the long-term recurrence rates in this patient cohort is being conducted. Another important limitation of this work is the low response rates for the PSF, which, we believe, might be attributed to advanced age and possible low literacy rates of our cohort. Finally, although the determination of recurrence rates was not the primary aim of this study, the NCCN criteria used for high-risk BCC might not be considered high risk by some physicians and this might have resulted in lower recurrence rates.
In conclusion, considering the high patient satisfaction rates and low short-term recurrence and complication rates demonstrated in the present study, we believe that MCSSE is a valuable and feasible surgical option for the treatment of high-risk BCCs, particularly in settings where MMS is not performed. Future studies investigating the long-term recurrence rates in high-risk BCCs and the use of MCSSE in SCCs are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.