
Abstract
Background:
Delivering quality dermatologic instruction to medical students can be difficult; time constraints, limited clinical teachers, and a lack of standardization pose challenges. The literature suggests that many trainees and primary care physicians could benefit from increased clinical dermatology teaching.
Objective:
We sought to deliver and analyze the results of a large-scale patient-viewing undergraduate dermatology education program.
Methods:
A total of 250 third-year medical students participated in a 32-station patient-viewing program. Voluntary pre- and posttest surveys were administered to evaluate knowledge and self-perceived abilities in dermatology. The identical tests were composed of 20 multiple-choice and 5 self-perception questions.
Results:
The response rate for completion of pre- and posttests was 24% (N = 59). Pre- and postknowledge test score means were 69.0% and 93.20%, respectively. Pre- and post–self-perception test score means were 3.95/10 and 7.25/10, respectively. Positive student feedback was received on the patient-viewing educational experience.
Conclusion:
Improvements in knowledge scores and self-assessment scores support the potential integration of structured patient-viewing teaching into undergraduate dermatology medical education curricula.
Background
Delivering quality clinical dermatologic instruction to medical students can prove difficult because of time constraints, limited clinical teachers, and a lack of standardization across North American medical schools. 1 On average, 20 hours are spent on undergraduate dermatology education across medical schools in Canada. 2 A recent survey of Canadian medical schools found that the majority of schools would like to have more time dedicated to dermatology teaching. 2 The literature also suggests that less than 40% of primary care residents felt their medical curricula prepared them to manage common skin disorders. 3
Upon graduation, up to 40% of medical students entering primary care fields can frequently encounter dermatologic issues in day-to-day practice. 4 A recent US study looking at why patients visit their physicians revealed that the prevalence of skin disorders was 47.2%, ranking above all other diagnoses. 5 In a separate study, when clinical slides of common skin disorders were presented to non–dermatologist physicians, a diagnostic accuracy of 25% was reported. 5 As such, providing medical students relevant clinical exposure and effective teaching should be a goal of all undergraduate medical education programs.
In recent years, many novel teaching methods have been applied to undergraduate medical education. The visual aspect of dermatology, in particular, allows for instruction to be provided using many modalities. Digital modules, problem-based learning, and objective structured clinical examination (OSCE) style teaching have all been reported in the literature, and the use of standardized patients consistently appears to be an effective way of teaching dermatology.6,7
In fall 2015, the University of Toronto Division of Dermatology restructured the undergraduate medical education curriculum, moving away from didactic lectures and 3 half-days of clinics and transitioning toward online modules with a large-scale, 32-station patient-viewing education program.
We hypothesized that a large-scale patient viewing covering many dermatology topics would be a novel and effective method of delivering dermatology education to undergraduate medical students. By combining various teaching modalities including videos, simulated surgical procedures, interactive stations, and standardized patients, we hoped to increase students’ knowledge of key dermatologic concepts while raising their confidence in our specialty. The primary objective of this study is to describe the new curriculum and the results of our educational intervention in students’ knowledge, self-perceived abilities, and overall student feedback.
Materials and Methods
Educational Program Background
The University of Toronto has a 4-year, graduate-entry undergraduate medical program typical of most North American medical schools. Our new dermatology program, Dermatology Transition to Clerkship, was delivered over a 2-day period at 2 academic hospitals in downtown Toronto. A total of 250 third-year medical students participated, and attendance was mandatory. The students were randomly assigned to small groups of 8-10 students, with 125 students rotating through 32 stations on Day 1, and the remainder on Day 2. Online modules based on the American Academy of Dermatology curriculum were completed on the alternate day. These educational modules were uploaded to the course website 1 week prior to the patient viewing and were available for voluntary viewing beforehand. Although the viewing of these modules was optional prior to the patient viewing program, their completion after the program was mandatory and enforced by the university. The students received a content test at the end of the Dermatology Unit based on lecture and clinical teaching material, but not specifically on these modules.
The 32 patient-viewing stations featured a mixture of educational videos, standardized patients, simulated dermatologic surgical procedures, and dermatology resident and staff-led teaching (Table 1). Each station was 8 minutes in duration. Students proceeded sequentially from station to station, similar to an OSCE format. Aside from one clinical note station, students were not graded on their performance and were, instead, encouraged to actively participate and ask questions.
Patient-Viewing Station Content.
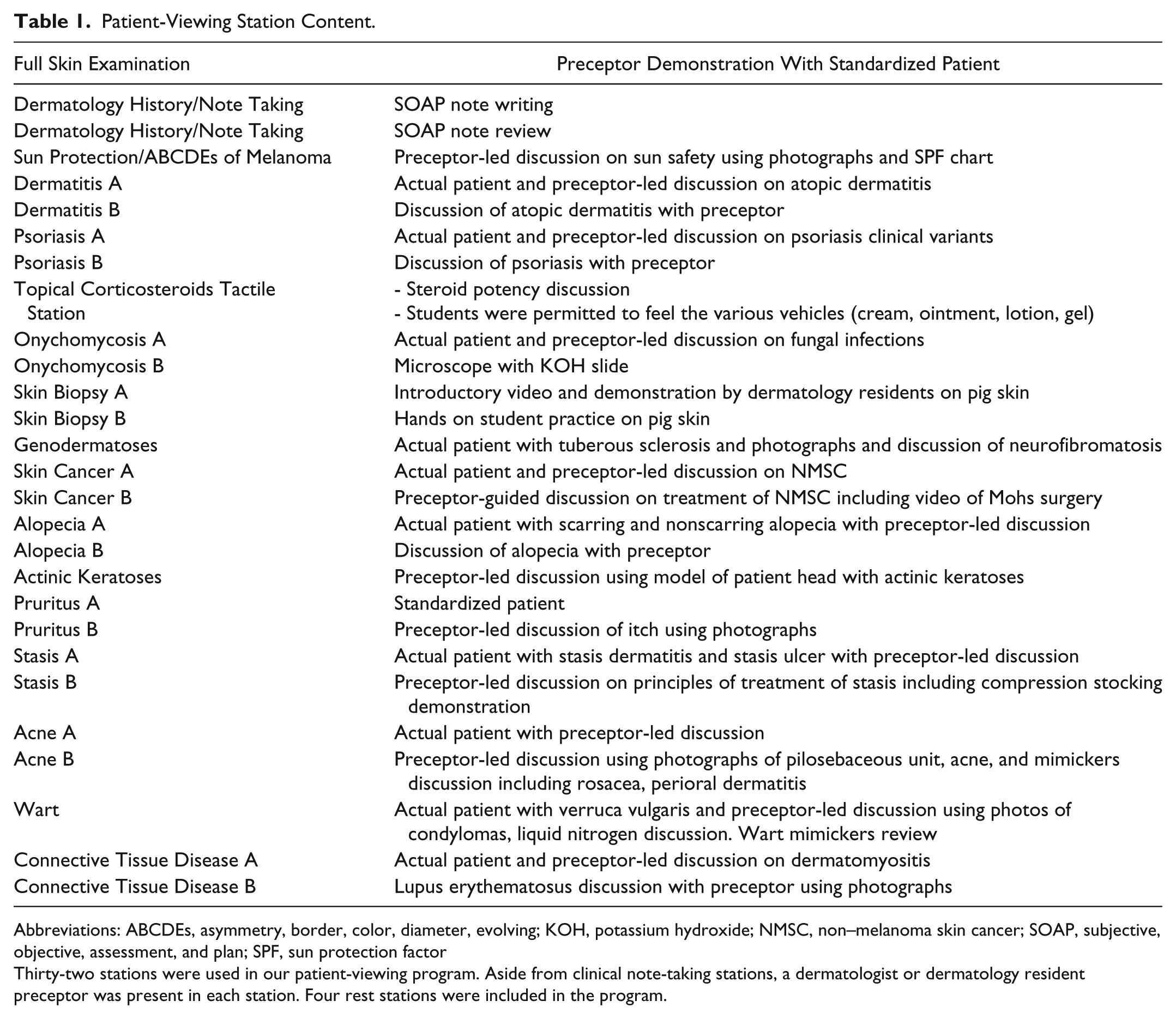
Abbreviations: ABCDEs, asymmetry, border, color, diameter, evolving; KOH, potassium hydroxide; NMSC, non–melanoma skin cancer; SOAP, subjective, objective, assessment, and plan; SPF, sun protection factor
Thirty-two stations were used in our patient-viewing program. Aside from clinical note-taking stations, a dermatologist or dermatology resident preceptor was present in each station. Four rest stations were included in the program.
Study Design, Evaluation, and Analyses
Ethics review is not required for program evaluation and quality improvement initiatives at our institution. Students were invited to complete a voluntary, 20-question multiple-choice examination and a 5-question, 10-point Likert scale questionnaire to evaluate their perceived confidence in areas including history-taking, morphological description, and skin biopsy before and after patient viewing (Tables 2 and 3). Completion of the questionnaire was considered implied consent to provide course feedback.
Multiple Choice Questions.
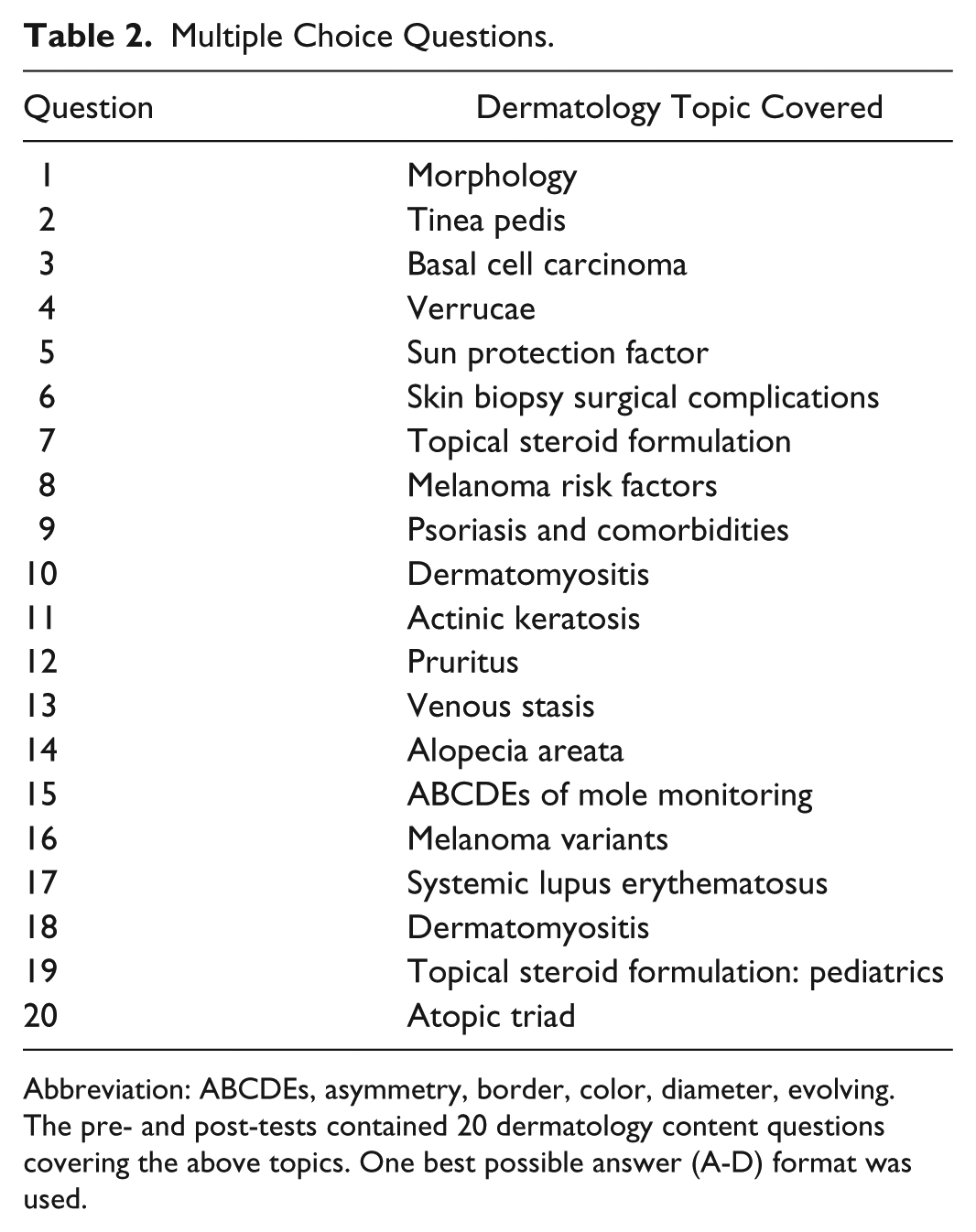
Abbreviation: ABCDEs, asymmetry, border, color, diameter, evolving.
The pre- and post-tests contained 20 dermatology content questions covering the above topics. One best possible answer (A-D) format was used.
Self-Perception Questions.
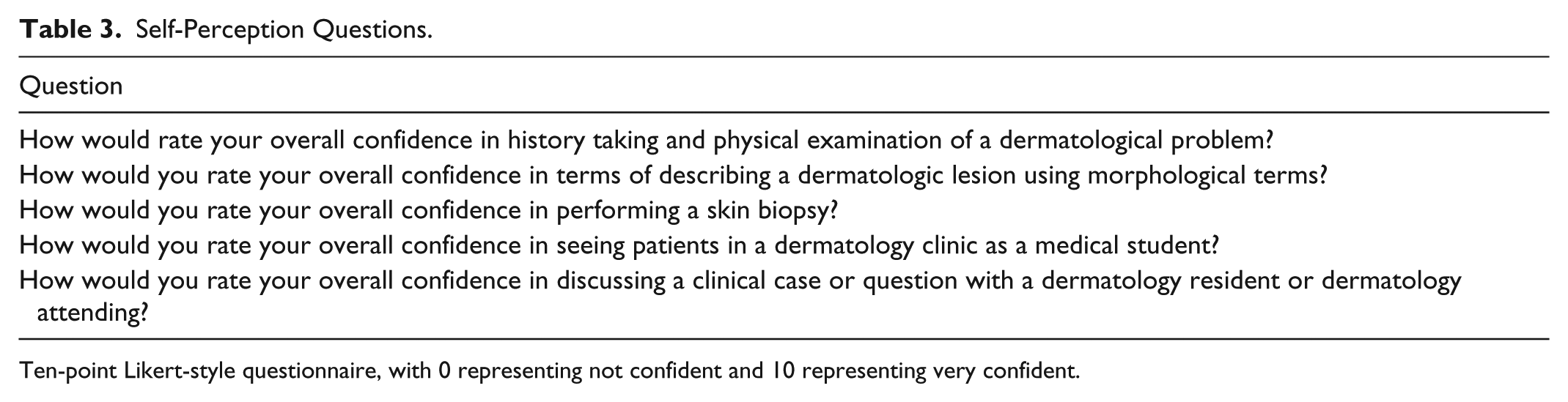
Ten-point Likert-style questionnaire, with 0 representing not confident and 10 representing very confident.
Although responses were anonymous, each student was asked to create a unique identifier to allow for pre- and posttest comparison. The pretest was distributed at an introductory session 1 week prior to patient viewing, and students were given time to complete the pretest in class. The voluntary posttest was administered at the conclusion of the second day of patient viewing at a wrap-up session.
We completed descriptive statistics and frequencies on the pre- and posttest data. A paired t-test comparing pre- and posttest scores was conducted using Stata with alpha = 0.05 (V13.1, College Station, TX, USA). Shapiro–Wilk test was nonsignificant indicating our data was normally distributed.
Results
Of the 250 medical students, 208 completed the pretest (83% response rate) and 68 completed the posttest (27% response rate). The overall pre- and posttest dermatology content mean scores were 68.9% (SD 0.11) and 93.2% (SD 0.06), respectively.
Fifty-nine students completed both pre and posttests (24% response rate) and were included in a detailed subgroup analysis. Within this group, the pretest mean was 68.9%. Areas of greatest baseline deficiency were defined as those achieving an incorrect score rate of 50% or greater. This particular cut-off was chosen to select out topics with which a substantial proportion of the class was uncomfortable. These included non–melanoma and melanoma skin cancer, topical steroid selection, and connective tissue disease (Table 4). After patient viewing, the posttest mean score increased to 93.20%.
Subgroup Dermatology Content Analysis.
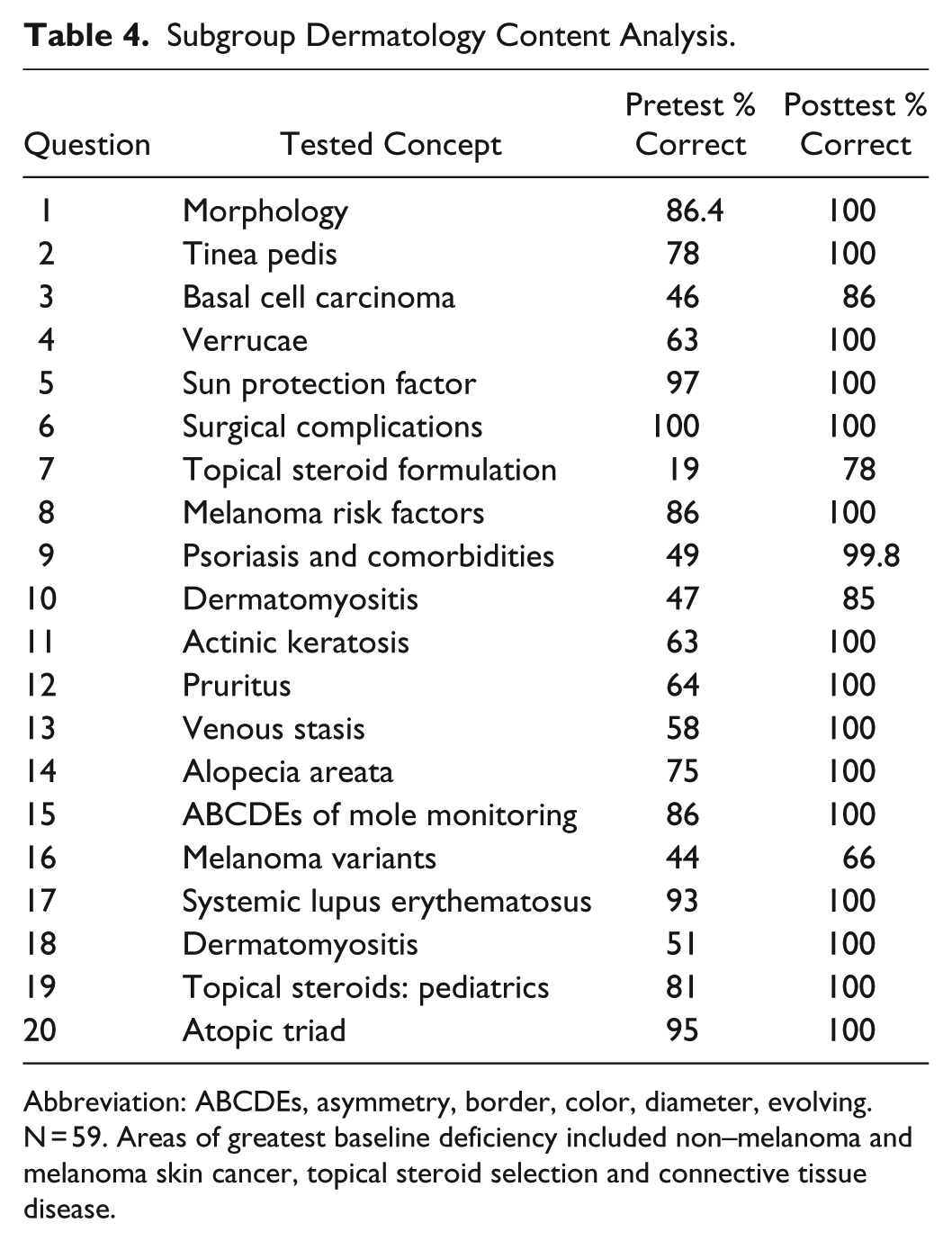
Abbreviation: ABCDEs, asymmetry, border, color, diameter, evolving.
N = 59. Areas of greatest baseline deficiency included non–melanoma and melanoma skin cancer, topical steroid selection and connective tissue disease.
Baseline self-perception analysis revealed low confidence in dermatology, with a mean overall pretest self-assessment score of 4.2/10, SD 1.8. Confidence in performing a skin biopsy, in particular, was extremely low with a mean score of 1.31/10 (SD 1.81, P < .01). Post-test self-assessment scores improved to a mean score of 7.24/10 (SD 1.75, P < .01) (Table 5).
Subgroup Self-Assessment Analysis.
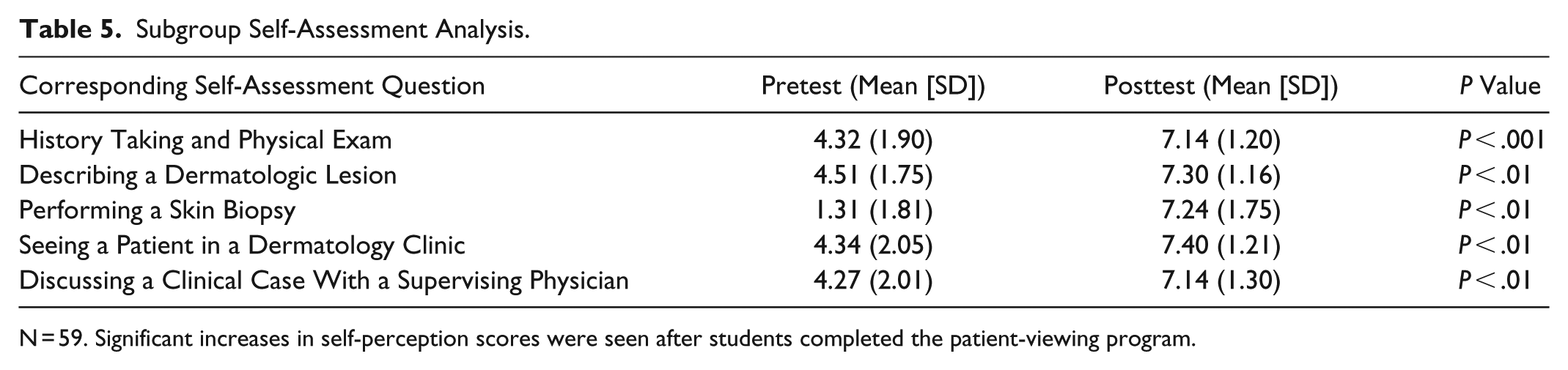
N = 59. Significant increases in self-perception scores were seen after students completed the patient-viewing program.
Overall student feedback on our patient-viewing program was positive across the evaluation categories of organization, learning opportunity, learning environment, and preceptors. The mean score was 4.35/5; scores ranged from 1 to 5, with 1 being the least consistent with a positive learning experience and 5 being the most consistent (Figure 1).
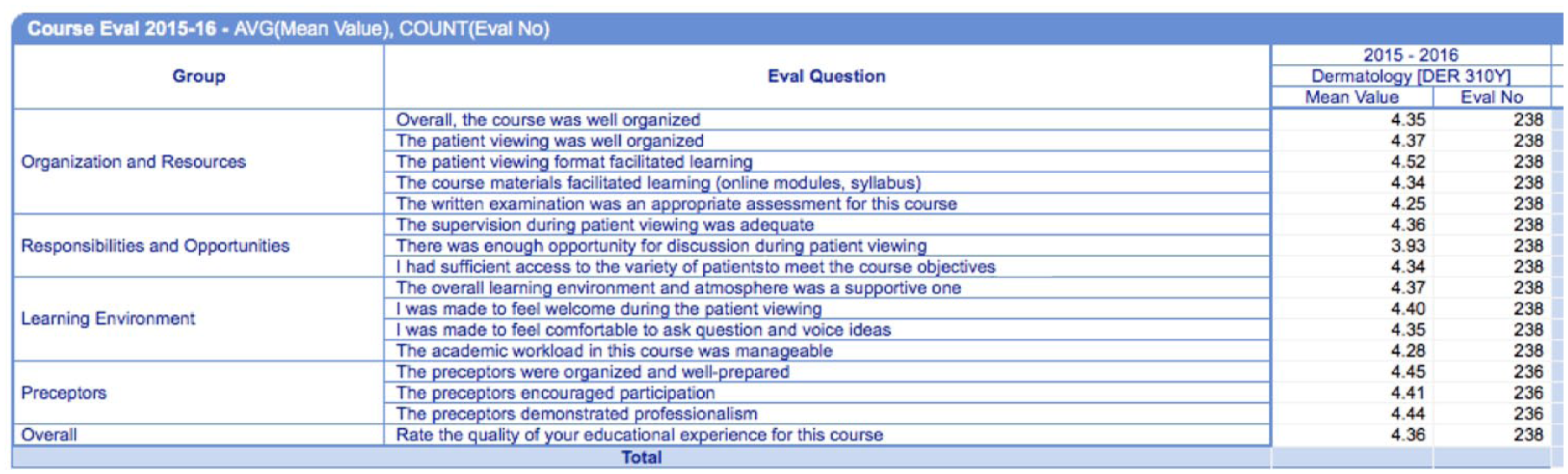
Student course evaluation: Scores range from 1 to 5, with 1 representing the most negative evaluation and 5 representing the most positive evaluation.
Discussion
Our pretest knowledge data showed low overall knowledge scores in third-year medical students nearing clerkship. Topics of deficiency spanned multiple content areas, from cutaneous malignancies to medications and connective tissue diseases. This suggests the need for a generalized increase in dermatology education at the undergraduate medical level, particularly as several of these subjects (eg, topical medications and skin malignances) are highly relevant both in primary care and hospital-based practices. Given the high dermatology case load that primary care providers carry, 8 we believe they are one of the most important stakeholders in defining dermatology curricula. Posttest knowledge data showed an improvement in all subject areas, particularly in discrete topics unique to the field of dermatology (eg, topical steroid formulations). The global improvement in knowledge scores after participation in the patient-viewing program supports its role in dermatology undergraduate medical curricula.
The pretest self-perception survey uncovered overall low mean scores in self-perceived ability. Although this population of medical students had not yet been exposed to clinical dermatology, they previously completed a 1-week, lecture-based dermatology course in their preclerkship curriculum. Their low mean scores in theory-based skills (discussing a case) in addition to clinical skills (performing a punch biopsy) demonstrate a generalized lack of confidence for dermatology abilities, despite prior teaching. The posttest scores demonstrate a significant increase in self-perceived abilities across all measured categories. Of note, performing a biopsy achieved both the lowest mean pretest score (1.4/10) and the greatest posttest score change (453% increase). Many medical schools will instruct on dermatologic procedures, but do not actually expect students to perform them. 3 However, as many as 63% of general practitioners have been found to perform skin biopsies. 9 Our results outline medical students’ lack of confidence with dermatology, particularly skin biopsies, and the significant improvement that patient-viewing education can have on their self-perceived abilities.
Hansra et al performed a similar needs assessment of dermatology education among primary care physicians and resident physicians at the University of California San Francisco and also revealed self-perceived deficiencies in a wide variety of content areas. 3 Additionally, a recent similar United Kingdom study of 595 final-year medical students demonstrated that learning in clinical and small-group settings was associated with higher confidence levels in students’ perceived dermatologic skills compared with lectures and other traditional teaching modalities. 10 Taken together with our knowledge and self-assessments results, such data support the need for increased dermatology education, and the potential suitability of clinical teaching modalities in undergraduate dermatology medical education programs.
Positive student feedback was also obtained regarding the patient-viewing education program. Similarly, the literature reports modular teaching in undergraduate dermatology that, similar to our program, includes active student participation, has also been shown to generate positive student feedback. 11 Independent of program efficacy, student feedback on educational courses remains an important consideration in the development of any curricula.
A dermatology-focused patient-viewing program of this magnitude and style is the first of its kind in Canada. Our program appeared to rapidly increase skill level in an efficient and effective manner. This novel method represents 1 approach to introducing medical students to clinical and surgical dermatology outside the traditional classroom. Given its success, the implementation of structured patient viewing could be a method for standardizing undergraduate dermatology medical education across multiple institutions.
Limitations
The generalizability may be limited as this study was conducted at a single urban academic institution and participation was voluntary. Additionally, the online dermatology modules were available for viewing before the pretest administration and voluntary viewing may have caused variability in baseline dermatologic knowledge. Moreover, students were not monitored in an exam-style setting and could have worked on the pre- and posttests together, which may have affected content scores. In addition, our posttest response rate was low at 23%, and we did not have the data to compare those who completed both pre- and posttests with those who did not. Finally, despite standardized content, different preceptors were involved in the patient-viewing stations on different days because of variable clinical responsibilities, which may have ultimately affected the content teaching received by students.
Conclusions
The first large-scale, patient-viewing education program for undergraduate dermatology curriculum was executed and assessed at the University of Toronto in fall 2015. Since then, this patient-viewing program has continued in full scale annually for third-year medical students. Global improvements in posttest dermatology knowledge and self-assessment scores, as well as positive student feedback on the course, were obtained. This supports the integration of a structured patient-viewing program into undergraduate dermatology medical education curricula. Future assessment of students’ knowledge retention can be pursued to further assess this model as a useful educational tool.
Footnotes
Acknowledgements
We would like to thank the University of Toronto Division of Dermatology, the Dermatology Education Interest Group at the University of Toronto, and the many dermatologists and residents who assisted in the development and implementation of this revised curriculum. We would also like to thank the University of Toronto medical students for their voluntary participation in our research study.
All authors listed contributed to the study design, data collection, analysis, and manuscript production. All authors approved the final version of this manuscript
Ethics approval is not required for program evaluation and quality improvement initiatives at our institution
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.