
Abstract
Introduction:
Laser and light-based therapies have emerged as interesting treatment options with minimal side effects or contraindications to treat onychomycosis. Although increasing reports of successful treatment exist, few randomized, controlled, prospective studies have evaluated their true efficacy. We conducted a prospective, randomized, double-blind, controlled trial to evaluate the cure rate of onychomycosis treated by laser.
Methods:
Fifty-one patients were randomized to receive 3 treatments (0, 12, 24 weeks) of 1064 Nd:YAG short-pulse (Cutera GenesisPlus) laser or placebo sham laser. The primary efficacy end point is the proportion of patients with a complete cure rate of the target great toenail at week 52. The secondary efficacy end points, at week 52, were treatment success defined as almost clear nail (≤ 10%) and negative mycology, completely or almost clear nail of the great toenail, negative mycology, improvement from one OSI severity class to another of the target toenail, and the difference in proximal nail plate clearance between baseline and week 52.
Results:
No patient (0%) in the laser group and 2 patients (7.7%) in the placebo group reached the primary outcome. One patient (4.8%) in the laser group reached treatment success vs 2 (7.7%) in the placebo group. Only 6 patients (33%) had negative cultures in the laser group vs 11 (50%) in the placebo group. None of the secondary end points were met.
Conclusions:
This study demonstrated that 3 treatments of Nd:YAG 1064 nm laser at 3-month intervals were not effective to treat onychomycosis.
Introduction
Onychomycosis, a fungal infection of the finger and/or toenails, is the most common nail disorder in adults, affecting 2% to 8% of the population.1,2 At present, systemic antifungal agents are the most effective treatment. However, their use is limited by the risk of serious side effects and potential drug interactions as well as the need for relatively long-term treatment. Even after successful treatment, onychomycosis has a 20% to 25% rate of relapse and/or recurrence. 3 Laser and light-based therapies have emerged as interesting treatment options with minimal side effects or contraindications. 4 Although increasing reports of successful treatment of onychomycosis with lasers exist, few randomized, controlled, prospective studies have evaluated their true efficacy. Data are also lacking on the optimal treatment schedule, duration, and laser parameters.
The FDA has approved multiple device systems since 2010 for the treatment of onychomycosis. However, they have been approved only to temporarily increase nail clarity, and not for a definitive cure. Although the precise mechanism of action of lasers in the treatment of onychomycosis is still unknown, one of the proposed mechanisms is that heat inhibits fungal growth, causing cell damage and ultimately fungal death. We selected the Nd:YAG laser because it penetrates more deeply into the tissue and better targets fungal overgrowth in the nail bed. Most studies published were using Nd:YAG lasers. These studies were small and uncontrolled, with inconsistently reported methodology, clinical and mycological evaluations, and treatment parameters. 5
We conducted a randomized, single-centre, controlled, double-blind study to evaluate the efficacy of the 1064 Nd:YAG short-pulse laser in the treatment of onychomycosis vs no treatment (sham laser).
Methods
This study is a randomized, double-blind, controlled trial to evaluate the efficacy and safety of the Cutera GenesisPlus, Nd:YAG 1064 nm short-pulse laser in treating onychomycosis of the toenails in adult patients, compared with a sham placebo laser. The primary efficacy end point for this study is the proportion of patients with a complete cure rate of the target great toenail at week 52.
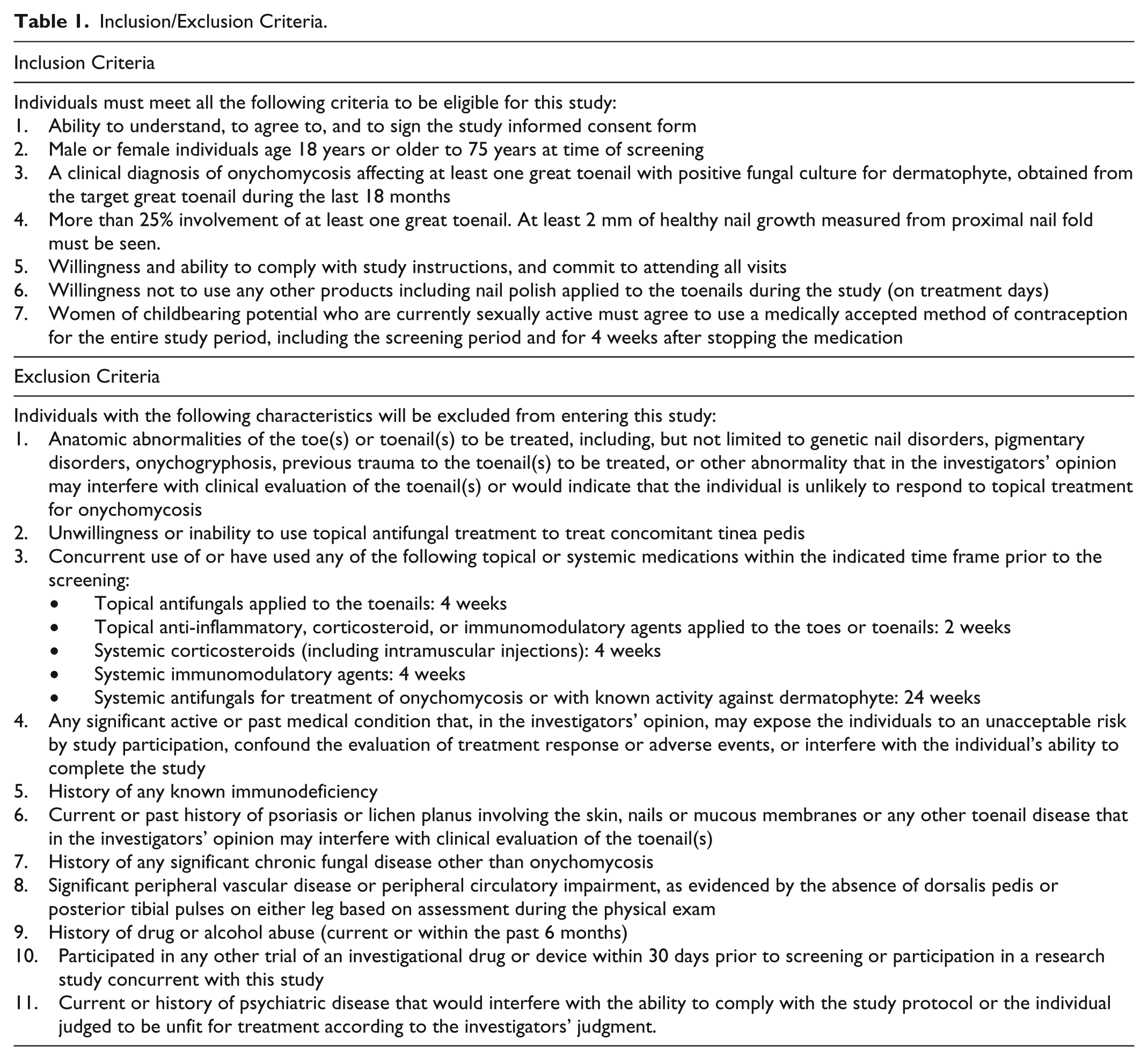
The study was conducted at a single academic centre between November 2013 and December 2014 and was approved by the institution’s ethics committee of the University of Montreal Hospital Center, in Quebec, Canada. The protocol can be found through the ethics committee. All patients signed an informed written consent. We recruited patients between age 18 and 75 years, with onychomycosis involving at least 25% of one great toenail and having a positive fungal culture for a dermatophyte (see Table 1 for complete inclusion and exclusion criteria). To reflect clinical practice, patients were not excluded based on the severity of disease unless they had proximal matrix involvement because these cases are the most difficult to treat.
Inclusion/Exclusion Criteria.
Participants were randomly assigned following a simple randomization procedure in a 1:1 ratio to either the 1064 nm Nd:YAG laser group or a sham laser group. The sham placebo laser procedure consisted of turning on the laser and aiming it at the different toenails while using the usual motions but without firing it. All patients were required to wear metal opaque goggles; hence they did not witness the change in light when the laser was fired. Patients were also advised that they may feel heat or nothing at all when treatments were given.
They were required to attend a total of 4 or 5 visits to the clinic. If criteria were met at screening then a baseline visit would occur the same day, followed by laser treatments at weeks 12 and 24 and a follow-up at week 52.
At the baseline visit, the most severely affected great toenail (excluding those with matrix involvement) was chosen as the target nail. This nail became the subject of our primary outcome. Although the great toenail represented the target toenail, all other clinically affected toenails were treated and evaluated. Participants were treated by a nonblinded investigator at baseline and at weeks 12 and 24. All patients were evaluated by a blinded investigator (same evaluator for all patients) at week 52.
Each visit included a clinical assessment of the extent of involvement in the percentage of the target great toenail. Evaluation of all other nails, other than the target great toenail, was performed at every visit and defined as a completely clear (0% toenail involvement), almost clear (disease present but ≤ 10% involvement), or more than 10% affected.
Calculation of the Onychomycosis Severity Index (OSI) 6 of the target nail was performed at every visit. The OSI provides a score by evaluating the percentage of nail plate involvement, the proximity of infection to the matrix, the degree of subungual hyperkeratosis, and presence of dermatophytoma. The score is obtained by multiplying the score for the involved area (range, 0-5) by the score for the proximity of disease to the matrix (range, 1-5). For the presence of dermatophytoma or for greater than 2 mm of subungual hyperkeratosis, 10 points are added. A cumulative score of 0 indicates cured, 1 through 5 mild onychomycosis, 6 through 15 moderate onychomycosis, and 16 through 35 severe onychomycosis. 6 Measurement of healthy nail growth from proximal nail fold was taken at baseline and final visit. Patients were questioned regarding adverse effects at each visit.
The following laser parameters were used at each visit: fluence of 6-8 J/cm2, pulse duration of 0.3 ms, spot size of 8 mm, and a repetition rate of 2.0 Hz. The entire nail plate of the great toenails was treated with 4 passes with a total pulse count of 400. The other affected toenails were treated with 4 passes, with a total pulse count of 25 pulses per nail per passage. Fluence was at a minimum of 6 J/cm2 but was increased up to a maximum of 8 J/cm2 according to patient tolerance to pain.
For the sham laser group, the laser was turned on, and the same amount of time was spent on the affected nails as in the treatment group but without firing the laser.
Photographs of the affected nails were taken at each visit. Patients were encouraged to use a topical antifungal treatment to treat concomitant tinea pedis if necessary without using it on affected nails. A fungal culture of the target nail was performed at week 52.
The primary efficacy end point of this study was the proportion of patients that reached complete cure of the target great toenail at week 52. Complete cure is defined as completely clear nail (CN) (0% involvement) and negative mycology of the target toenail.
The secondary efficacy end points were treatment success, defined as almost clear target nail (≤ 10% of the toenail) in addition to negative mycology at week 52, completely CN or almost CN of the target great toenail at week 52, negative mycology of the target great toenail at week 52, improvement from one OSI severity class to another of the target toenail, and the difference in proximal nail plate clearance between baseline and week 52. An additional secondary end point was the number of nails (other than the target) with complete clinical nail plate clearance at week 52.
Statistical Methods
To have 80% power to detect a minimum difference of 0.32 (with a 2-sided alpha of 0.5) in the proportion of patients achieving a complete cure, sample size calculations indicated that we needed to enrol 52 patients at a 1:1 allocation ratio of laser to placebo.
Descriptive statistics (t-tests and chi-squared tests) were used to compare the characteristics of patients at baseline and ensure that randomization was successful. The proportion of patients experiencing a complete cure, treatment success, improvement in OSI severity class, or negative mycology results at week 52 were compared using chi-squared tests or Fisher exact tests when cell sizes less than 5 were observed. The difference in mean OSI score between groups and mean proximal nail plate clearance was assessed at each time point using t-tests. When missing data were observed, we imputed results using last observation carried forward for all continuous variables, and nonresponder imputation for all categorical variables. To test the robustness of our results, we conducted a sensitivity analysis in which we imputed missing observations of categorical variables to favour the laser treatment group and defavour the placebo group.
Results
Fifty-four patients with positive fungal culture in the previous 18 months were assessed for eligibility. Three were excluded because they did not meet inclusion criteria (2 were on systemic prednisone, and 1 lacked the minimal involvement of a great toenail). The remaining 51 patients were randomly assigned in a 1:1 ratio to receive either the 1064 Nd:YAG short-pulse (Cutera GenesisPlus) laser treatment (N = 25) or the placebo sham laser (N = 26). Seven patients were lost to follow-up after 1 treatment and did not complete the study: 4 in the laser group and 3 in the placebo group. Baseline characteristics were similar in both groups (Table 2).
Characteristics of Patients at Baseline.
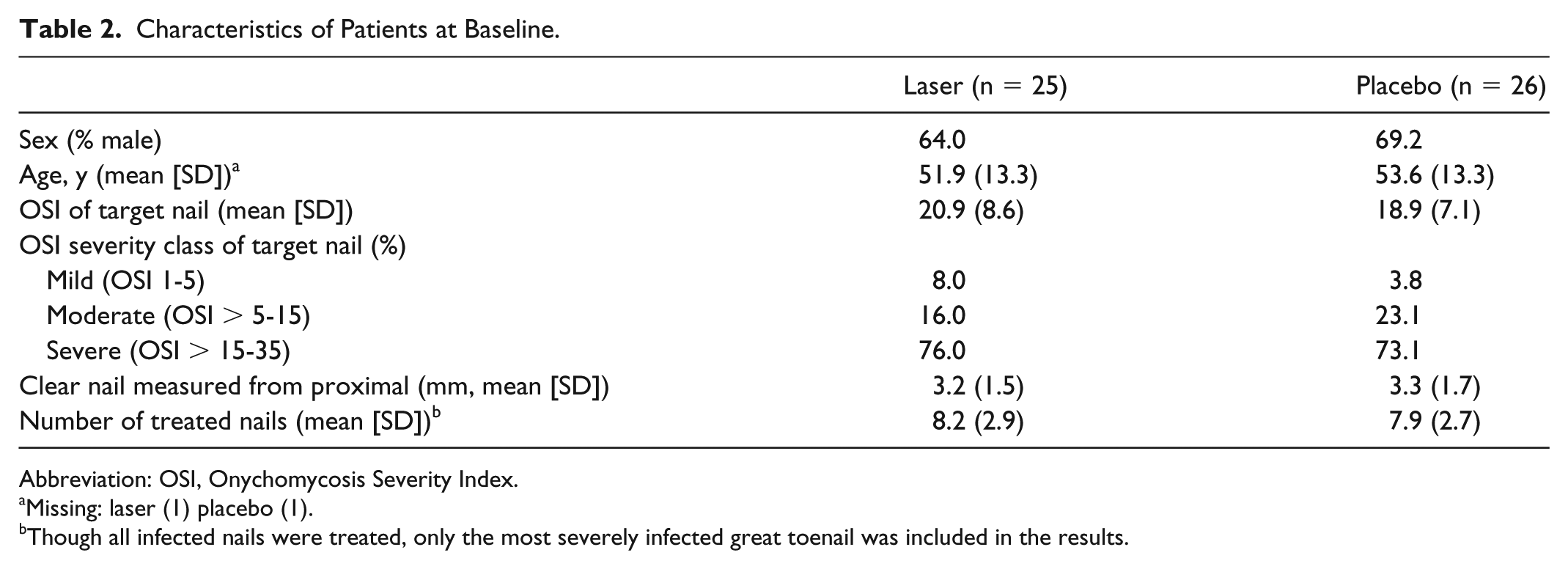
Abbreviation: OSI, Onychomycosis Severity Index.
Missing: laser (1) placebo (1).
Though all infected nails were treated, only the most severely infected great toenail was included in the results.
No patient (0%) in the laser group, whereas 2 patients (7.7%) in the placebo group, reached the primary outcome (a completely CN and negative mycology).
For the secondary end points (Table 3), 1 patient (4.0%) in the laser group reached treatment success (almost CN and negative mycology) compared with 2 patients (7.7%)in the placebo group. Only 6 patients (24%) had negative cultures in the laser group vs 11 (42.3%) in the placebo group. Cultures were performed in 40 patients at 52 weeks (omitted/inadequate specimen in 4 patients: 3 patients in the laser group and 1 in the placebo group). For the 4 patients for whom the cultures were not obtained, none would have reached the primary outcome because they all had more than 10% of their target nail involved at week 52.
Clinical and Mycological Results of Target Nail.
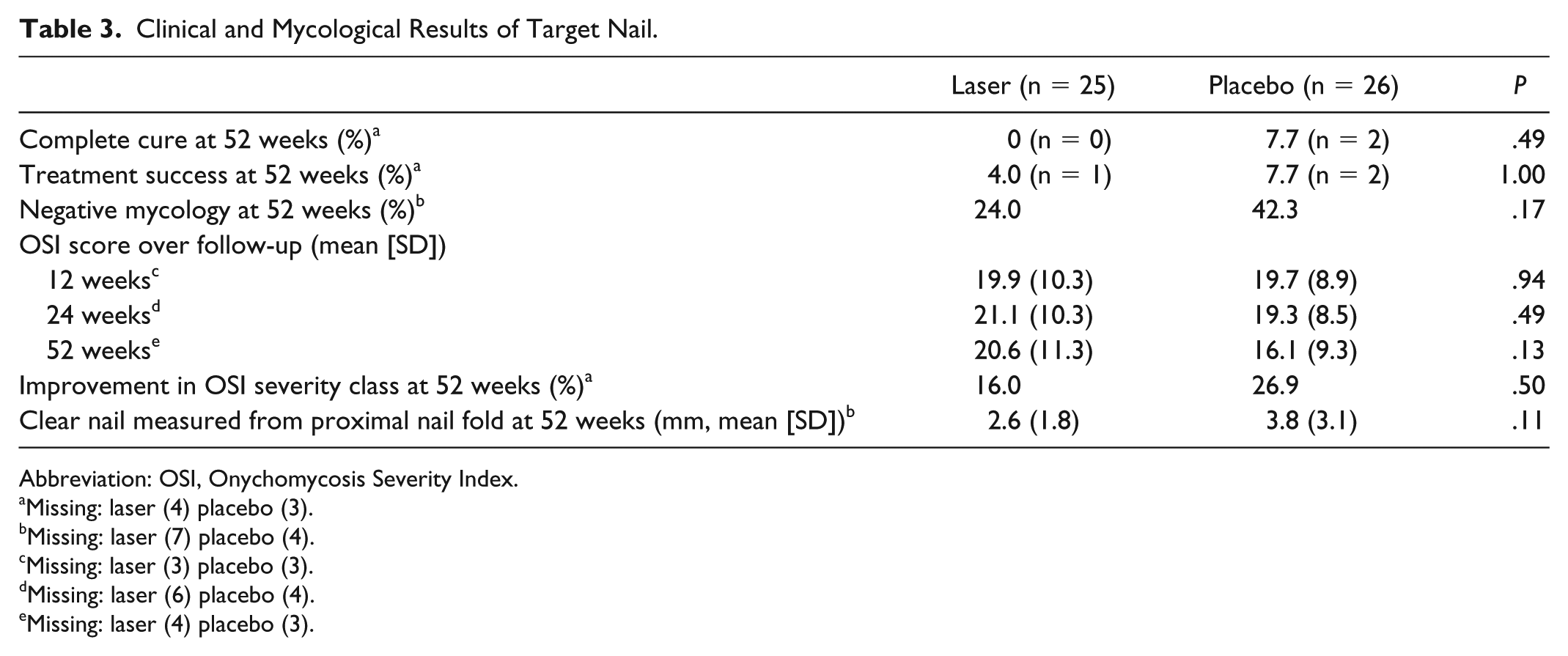
Abbreviation: OSI, Onychomycosis Severity Index.
Missing: laser (4) placebo (3).
Missing: laser (7) placebo (4).
Missing: laser (3) placebo (3).
Missing: laser (6) placebo (4).
Missing: laser (4) placebo (3).
In the laser group, 3 patients had 1 grade category of OSI improvement and 1 had 2 grades of improvement (from severe to mild). Three patients had 1-grade improvement and 1 had 2-grade improvement (from severe to mild). None of the patients at week 52 had a worsening in OSI category. Seven patients in the placebo group had at least 1 grade of improvement in severity of OSI (5 had a 1-grade improvement, 1 went from severe to cured, and 1 from moderate to cured). Two patients in the placebo group at week 52 had worsened their OSI category by 1 grade.
Most patients in the laser group experienced multiple temporary burning/intense heat sensations, often requiring a few seconds of pause during the treatment, but none resulted in dropout from the study. No other serious or adverse reactions were observed.
When missing data were imputed to favour the laser group, the proportion of patients who responded successfully to treatment was not significantly different between groups (complete cure: laser 16.0%, placebo 7.7%, P = .42).
Though data were not complete for all patients, our sensitivity analyses show that the observed lack of efficacy of the laser was not due to differential dropout because even if all missing laser patients had successfully responded to treatment, this would not have been sufficient to show a significant benefit of the laser over placebo.
Discussion
In this study, 51 patients with onychomycosis were randomly assigned to receive either an Nd:YAG 1064 nm short-pulse laser vs a sham laser (no treatment). We found that the Nd:YAG laser was not effective in achieving either our primary end point nor any of our secondary end points. In many studies, the outcome is mycological cure and not clinical cure. Mycological tests are often falsely negative. Because we conducted a trial that was not sponsored by either the pharmaceutical industry or a laser manufacturer, we selected a more stringent measurement outcome. Complete cure was chosen as a primary end point as we felt it was a more meaningful target to be reached in clinical practice.
Our study allocated patients, rather than individual toenails, to the groups for the same clinically meaningful reason. We found that 2 patients in the placebo group and no patients in the treatment group achieved the primary end point of complete cure of the target toenail.
One patient in the treatment group and 2 in the placebo group achieved treatment success. Even if this 1 patient achieved an almost clear target toenail (less than 10%) with laser treatment, the other treated nails remained involved and it did not result in an overall acceptable esthetic outcome for this individual (Figures 1 and 2).
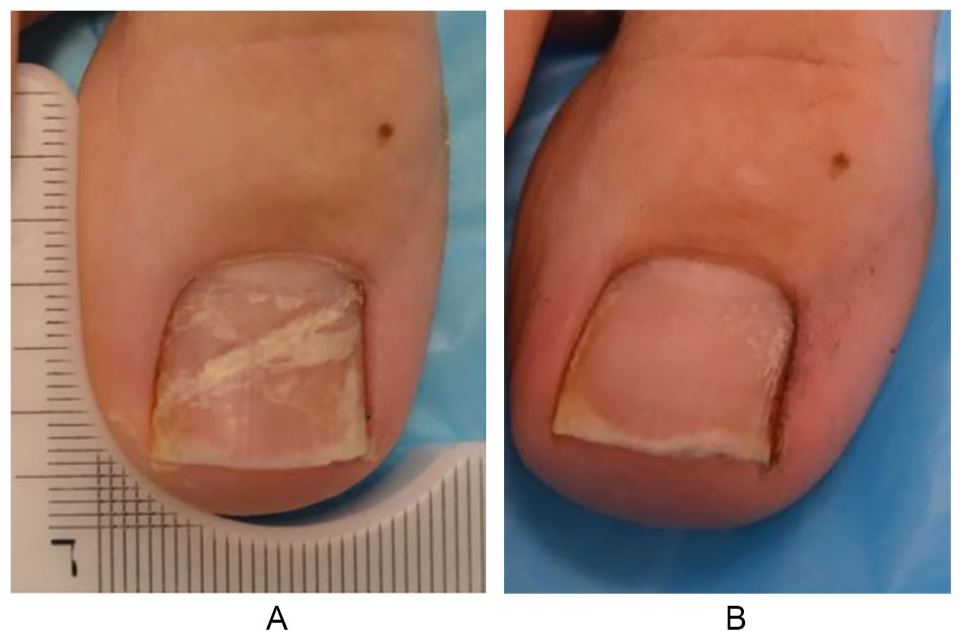
Target nail, onychomycosis, patient 16.

Nontarget nails, patient 16.
Our laser parameters and treatment intervals were chosen based on previous studies that reported success with the Nd:YAG 1064 nm laser as well as those suggested by the laser manufacturer.7,8 We chose to follow our patients for a total of 52 weeks to allow sufficient time for clear nail regrowth.
Our results are in contrast with a few open-treatment previous studies. Zalacain et al, 9 in a case series of 156 patients, showed an 85% cure rate (negative culture and clear nail) after 18 months with 3 treatments spaced 15 days apart. Rivers and colleagues 10 published their real-life experience: A total of 72.5% of nails with more than 67% involvement had statistically significant improvement in 100 patients. Galvan Garcia 11 showed a 100% clinical and mycological response (potassium hydroxide negative) rate at 9 months with 1 laser treatment in 120 patients.
Our results demonstrating lack of efficacy are in line with 2 other randomized, controlled trials: Hollmig and colleagues 12 failed to demonstrate a statistically significant mycological cure (at 3 months) or clinical nail plate clearance (at 3 and 12 months) after 2 treatments compared with controls (n = 27), and Karsai et al 13 showed no difference in mycological remission or improvement of OSI between the laser group (n = 20) receiving 4 treatments in 4- to 6-week intervals and the no-treatment group.
The main limitation of our study includes the treatment schedule (3 sessions only). It is possible that patients could have cleared with a different treatment schedule, including more treatments and shorter intervals or with more-intensified laser parameters, for example, with increased fluence. However, some previous noncontrolled studies have demonstrated clearance with as few as 1 or 2 treatment sessions.9,11,14 Also, from our experience, our patients would not have tolerated higher fluence because of significant discomfort at the fluences used (6-8 J/cm2). The absence of planimetry to measure the primary outcome is also a limitation but, as evaluated in the study by Gupta and Cooper, 15 comparison showed good statistical agreement of visual and planimetry measures.
Although the patients were truly blinded, because the administration of the treatment was identical in both groups (metal shields, turning on the machine for all patients, same physical motion, same time spent with each patient), some potential patients could have been unblinded because of the heating sensation related to the laser. However, we feel this is of limited impact since our trial did not show benefits in the laser group. Finally, our study was not registered on Clinicaltrials.gov, but it was accepted by our ethics board.
We should also discuss the fact that potentially only patients with milder nail involvement could improve with laser treatments. In our study, all severity grades were included as long as they did not have matrix involvement (a 2 mm clear nail from the matrix). This resulted in 38 (75%) of our patients having a baseline OSI of severe. In the laser group, 2 of the only 4 moderate OSI patients became mild at week 52 and the only mild OSI patient remained mild at the end of the study. We made the decision to include patients based on real-life cases and not to select only milder patients in whom we might have had more potential to see improvement with the laser.
In conclusion, this study demonstrated that 3 treatments of Nd:YAG 1064 nm laser at 3-month intervals were not effective in the treatment of onychomycosis. Future studies should continue to assess its efficacy as well as other types of lasers in randomized, controlled trials in an attempt to clarify whether there is efficacy and what the ideal treatment schedules should be. At this time there are not sufficient data to support this modality as a treatment for onychomycosis.
Footnotes
Acknowledgements
The authors acknowledge Sara Johnson for data analysis assistance and writing assistance, and Robert Bissonnette for writing assistance.
This study was successfully approved by the hospital ethics committee. The study was not registered.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A $5000 research grant was received from the University of Montreal Lise Bachand Fund.