
Abstract
Introduction:
There is a paucity of prevalence data for genital angiokeratomas in adults. The objective of this article is to determine prevalence of genital angiokeratomas in adults as a function of sex, age, and race/ethnicity.
Methods:
A cross-sectional study was conducted over 11 months during 2013 and 2014 using a convenience sample of adult men and women consenting to genital examination during melanoma screening and surveillance by a senior dermatologist in an outpatient clinic. The analysis was conducted from April through December 2016.
Results:
Of 213 white/European American adults examined (127 men and 86 women), genital angiokeratomas were detected in 30.0% (64/213). Presence of at least one genital angiokeratoma was significantly associated with male sex (odds ratio [OR], 2.4; 95% confidence interval [CI], 1.3-4.5; P < .001) and age older than 50 years (OR, 3.4; 95% CI, 1.7-6.7; P = .008).
Conclusions:
Genital angiokeratomas are relatively common in adults of white/European American origin and important to recognize because of their benign nature and occasional confusion with other tumors.
Keywords
Introduction
Genital angiokeratomas are relatively small red or purple papules consisting of hyperkeratotic epidermis and ectasia of superficial vessels, first described on the adult scrotum by Fordyce in 1896.1,2 Early in their evolution, lesions are red, shiny, and compressible, eventually becoming purple, hyperkeratotic, and less compressible over time. Fordyce angiokeratomas have been broadened to include genital angiokeratomas both in women and men. In women, lesions most commonly involve the labia majora, and rarely the clitoris, thighs, and lower abdomen. In men, lesions most commonly involve the scrotum, and rarely the glans penis, penile shaft, thighs, and lower abdomen.
Histopathologic features of genital angiokeratomas in men and women alike, described in detail by Imperial and Helwig,3-5 consist of enormously dilated vessels that form lacunae, surrounded by collarets of epidermal acanthosis and elongated rete ridges, with moderate to marked epidermal hyperkeratosis. Thrombosis of tiny venules may be noted, especially for lesions in the elderly. Elastic tissue surrounding vascular lacunae is reduced and fragmented.
Basic epidemiologic information is lacking for genital angiokeratomas. Although usually recognized as benign, these lesions are important to recognize because of occasional confusion with other tumors. Furthermore, determining the prevalence of these lesions may help providers understand the burden of disease and prevent unnecessary biopsies or referrals. Our study was an attempt to determine the prevalence of genital angiokeratomas and their predisposing factors in a convenience sample of adults presenting to one senior dermatologist’s outpatient practice in which inspection of the genitalia and perianal area is routinely offered as an integral component of a complete mucocutaneous examination during melanoma/skin cancer screening and surveillance.
Materials and Methods
The study population consisted of adults presenting to a senior dermatologist (A.R.R.) in the outpatient Dermatology Department at Rush University Medical Center (RUMC), Chicago, IL, USA, between November 25, 2013 and October 16, 2014, as previously described. 6 Men and women of age at least 18 years were included regardless of race/ethnicity, sex, or pregnancy status but were excluded if the medical encounter was related to a genital lesion or if exigencies precluded complete examination or data collection. Written informed consent procedures were approved by the RUMC Institutional Review Board on Human Studies.
Race/ethnicity was determined by self-report and observation according to classifications outlined by the US Office of Management and Budget, the US Census Bureau, and the Canadian Census Bureau. White/European American (W/EA) was used to refer to individuals with white skin and of European ethnic origins. Non-white/non-European American (non-W/EA) was used to refer to individuals of other ethnic origins.
Genitalia were examined by the senior author (A.R.R.) with patients lying in a supine position, thighs and legs spread laterally. For males, all surfaces of the penile shaft (with foreskin self-retracted if uncircumcised), and scrotum were visualized. For females, both the medial and lateral surfaces of the internal and external labia were visualized, as were the clitoral hood, and clitoris with clitoral hood retracted.
Genital angiokeratomas were defined as well circumscribed, single or multiple red or purple papules 0.5 to 2 mm in diameter, occasionally larger (Figure 1, A and B). Dermatoscopic examination was used to confirm a lacunar pattern if there was a single lesion that could be confused for some other tumor. Presence or absence of one or more genital angiokeratomas was noted, with lesion counts recorded as none, 1-5, 6-10, 11-20, and more than 20.
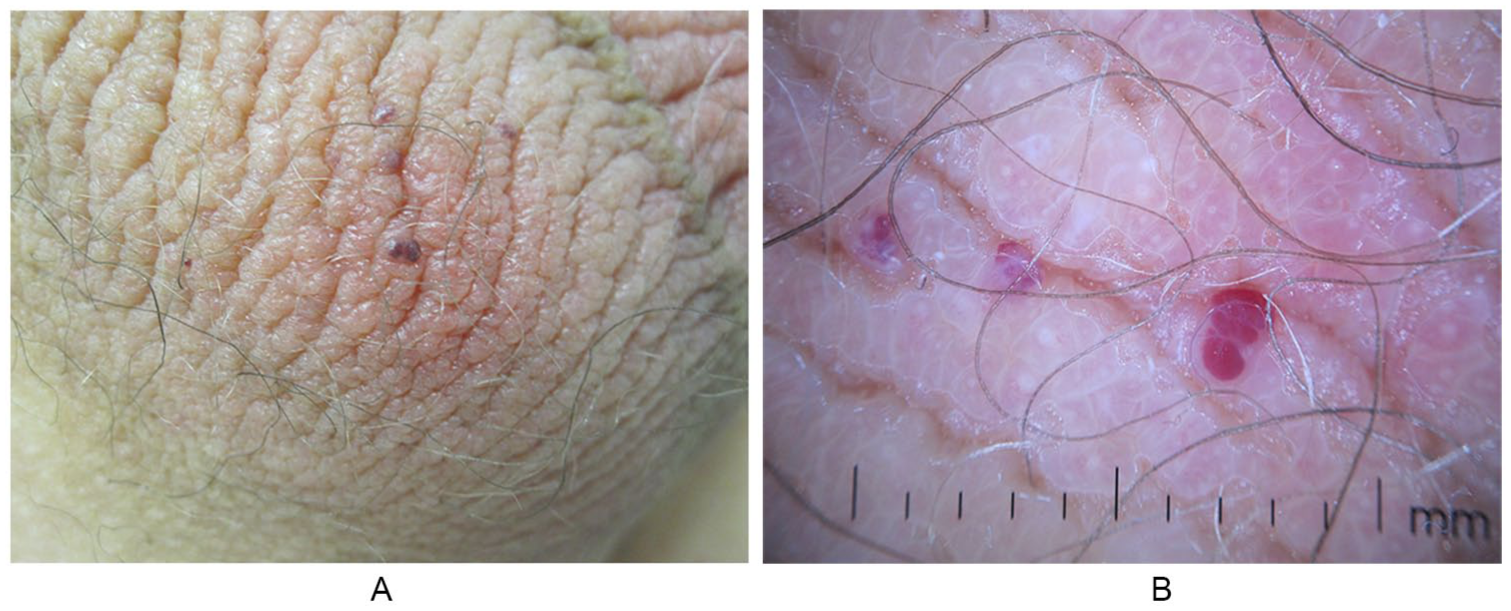
Scrotal angiokeratomas in a 47-year-old White/European American man
Data were analyzed using Microsoft Excel Office 2011 software (Microsoft Corp). The main outcome measure was absence or presence of one or more genital angiokeratomas, with comparisons to demographic variables. Categorical variables were compared using Pearson χ2 test. Crude odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were calculated. Reported P values are 2-tailed, with significance set at P < .05. The coefficient of determination, r2, was used to determine the proportion of variance in the dependent variable that is predictable from the independent variable. An r2 of 1 indicates that the regression line perfectly fits the data.
Results
In a convenience sample of 238 consecutive adults asked to participate, 4 declined genital examination, and 4 were excluded from our analyses because of missing data points. Of the remaining 230 individuals, 213 were W/EA and 17 non-W/EA. Small numbers of non-W/EA adults precluded statistical comparisons with W/EA adults. All subsequent statistics relate to the 213 total W/EA adults.
The 213 W/EA adults included 127 men and 86 women, ages 23 to 84 years (median 55 years; mean [SD], 53.2 [15.2] years). Genital angiokeratomas were detected in 30.0% (64/213) of the W/EA adults. Of these 64 men and women who had 1 or more genital angiokeratomas, 1-5 lesions were detected in 59.4% (38/64), 6-10 lesions in 18.8% (12/64), 11-20 lesions in 15.6% (10/64), and more than 20 lesions in 6.3% (4/64) (Table 1). Among the 47 men who had 1 or more angiokeratomas, 53.2% (25/47) had 1-5 lesions; 23.4% (11/47) had 6-10 lesions; 14.9% (7/47) had 11-20 lesions; and 8.5% (4/47) had more than 20 lesions. Among the 17 women who had 1 or more angiokeratomas, 76.5% (13/17) had 1-5 lesions; 5.9% (1/17) had 6-10 lesions; 17.6% (3/17) had 11-20 lesions; and none had more than 20 lesions.
Prevalence of Genital Angiokeratomas and Number of Lesions per Person in White/European American Adults, According to Sex and Age.
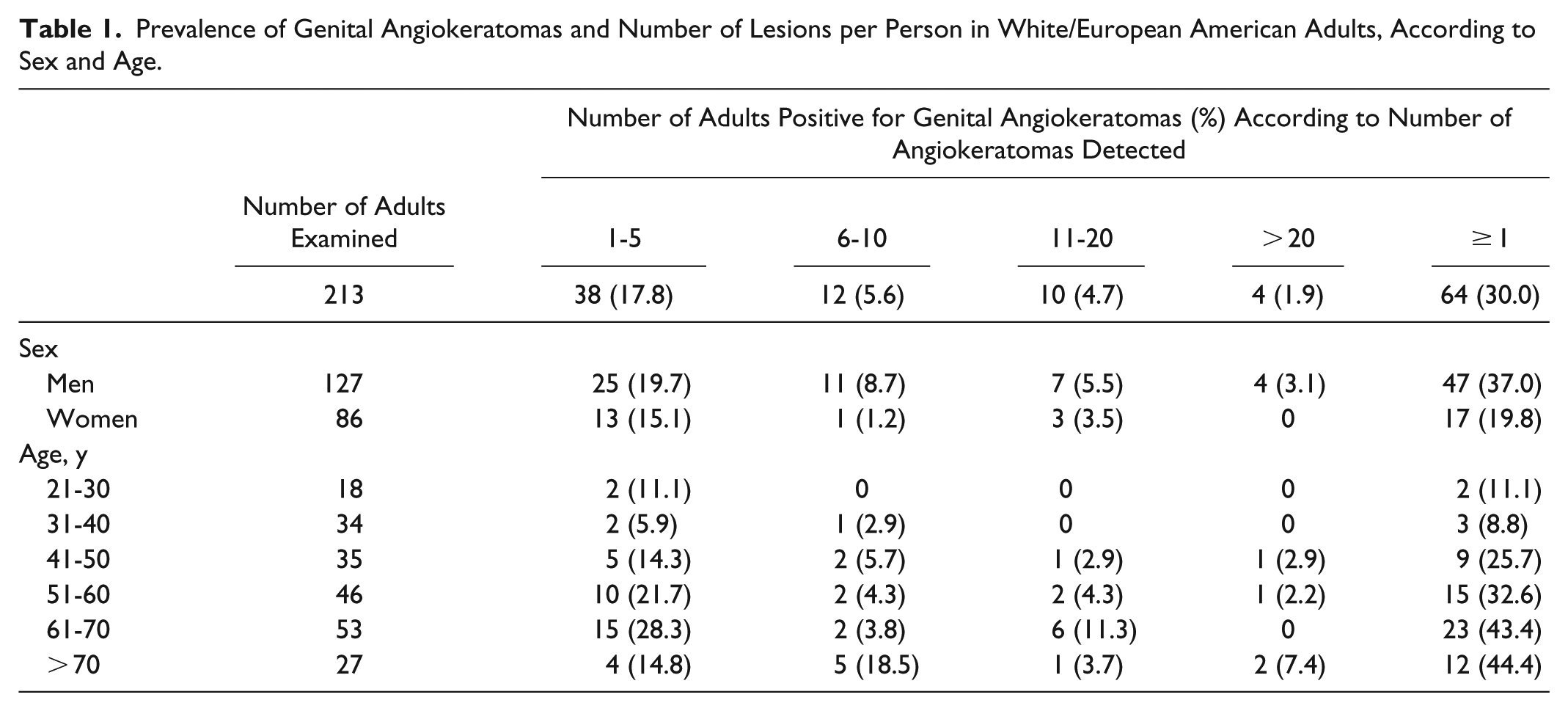
For W/EA men and women combined, prevalence of genital angiokeratomas was positively correlated with increasing age: 21-30 years, 11.1%; 31-40 years, 8.8%; 41-50 years, 25.7%; 51-60 years, 32.6%; 61-70 years, 43.4%; and older than 70 years, 44.4% (Table 1) (r2 = 0.925).
Prevalence of genital angiokeratomas in W/EA men (37.0%, 47/127) was significantly greater than in W/EA women (19.8%, 17/86) (OR, 2.4; 95% CI, 1.3-4.5; P = .008) (Table 2). There was a more than 2-fold greater prevalence of genital angiokeratomas in W/EA adults older than 50 years vs 50 years or younger: 39.7% (50/126) vs 16.1% (14/87) (OR, 3.4; 95% CI, 1.7-6.7; P < .001). When examined by subdividing age groups according to sex in W/EA adults, there was a significantly greater prevalence of genital angiokeratomas in men older than 50 years vs men 50 years or younger: 48.1% (39/81) vs 17.4% (8/46) (OR, 4.4; 95% CI, 1.8-10.6; P < .001) and a nonsignificant trend of greater prevalence of genital angiokeratomas in women older than 50 years vs women 50 years or younger: 24.4% (11/45) vs 14.6% (6/41) (OR, 1.9; 95% CI, 0.6-5.7; P = .26).
Demographic Factors Associated With Genital Angiokeratomas in White/European American Adults.
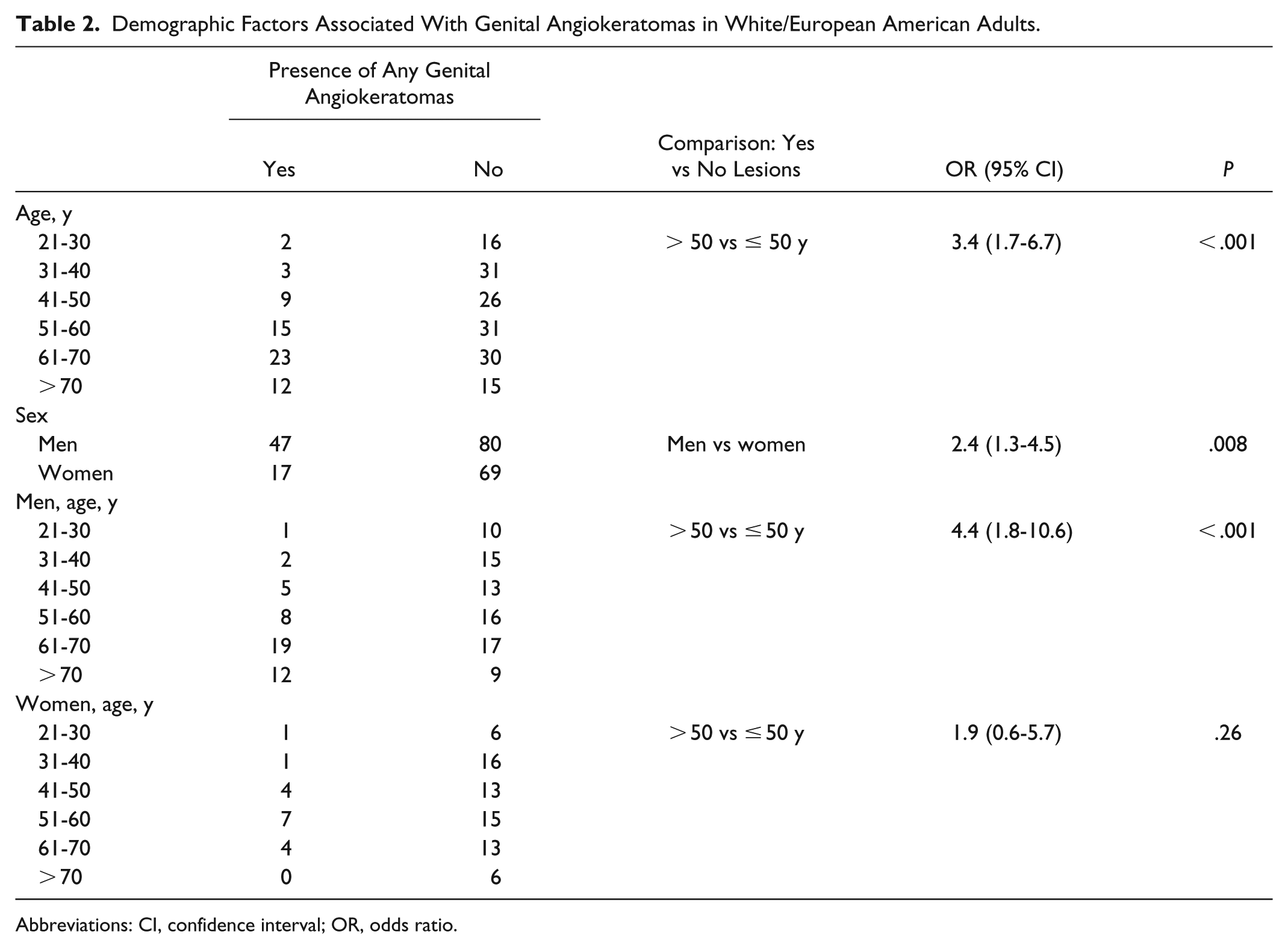
Abbreviations: CI, confidence interval; OR, odds ratio.
Of the 64 W/EA men and women who had 1 or more genital angiokeratomas, there were nonsignificant trends for more than 10 lesions in adults older than 50 years (24%, 12/50) vs adults 50 years or younger (14.3%, 2/14) (OR, 1.9; 95% CI, 0.4-9.7; P = .72); and more than 10 lesions per person in men (23.4%, 11/47) vs women (17.6%, 3/17) (OR, 1.4; 95% CI, 0.3-5.9; P = .74) (Table 3).
Number of Genital Angiokeratomas in White/European American Adults Who Had Any Genital Angiokeratomas, According to Sex and Age.
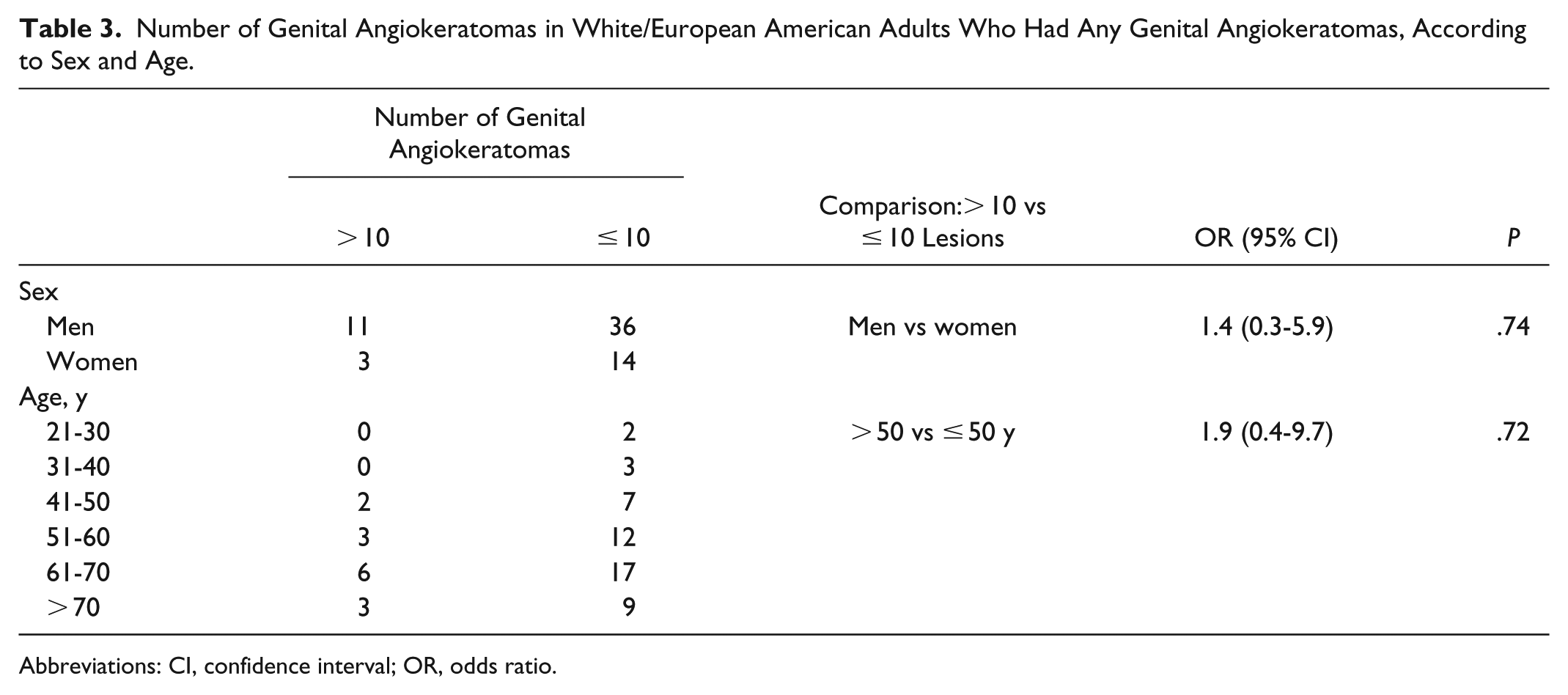
Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
Angiokeratomas are commonly classified into 5 subtypes based on gross morphologic features, localization, etiology, and age at presentation. Angiokeratoma corporis diffusum, associated with Fabry disease, is the only subtype that is generalized and commonly apparent within the first decade of life. 7 Solitary or multiple papular angiokeratomas usually appear in middle age and have a predilection for the lower extremities. 7 Angiokeratoma circumscriptum naviforme is a congenital capillary-lymphatic malformation commonly localized to the extremities.7,8 Angiokeratomas of Mibelli appear on the lateral and dorsal hands and feet during adolescence, noted primarily in women with a history of chilblains. 8 Angiokeratomas of Fordyce, also known as angiokeratomas of the scrotum and vulva, are acquired lesions noted predominantly in adults and are the focus of this study.
We determined the prevalence of genital angiokeratomas in a convenience sample of 213 adults attending the outpatient practice of one senior dermatologist specializing in screening and surveillance for cutaneous melanoma and keratinocytic skin cancer. We found that the prevalence of genital angiokeratomas was 30.0% in this W/EA adult population, significantly correlated with age older than 50 years and male sex. Providers should be cognizant of the high prevalence of genital angiokeratomas to prevent unnecessary biopsies or specialist referrals. Greater numbers of genital angiokeratomas per person were not significantly associated with sex or age, but there may have been too few individuals examined to specifically assess these associations.
There is a paucity of data related to prevalence of genital angiokeratomas according to sex, age, and race/ethnicity. Izaki reported the prevalence of angiokeratomas of the scrotum in Japanese men according to age: 16-20 years, 0.6% (5/887); 21-30 years, 1.5% (5/330); 31-40 years, 6.2% (6/97); 41-50 years, 13.1% (11/84); 51-60 years, 13.4% (9/67); 61-70 years, 15.9% (10/63); and older than 70 years, 16.7% (4/24). 9 When these numbers are collated, the prevalence of genital angiokeratomas in Japanese men studied by Izaki was 14.9% (23/154) for men older than 50 years vs 1.9% (27/1398) for men 50 years or younger. 9 In our study, we found that the prevalence of genital angiokeratomas in W/EA adults was 48.1% (39/81) for men older than 50 years vs 17.4% (8/46) for men 50 years or younger. When our results are compared with those of Izaki, it appears that genital angiokeratomas may be more common in W/EA men compared with Japanese men within the same age ranges. Additional studies will be required to assess the prevalence of genital angiokeratomas according to race/ethnicity and skin color.
Most available studies of genital angiokeratomas consist of case reports and small case series.2-5,10-21 Bean reported the prevalence of scrotal angiokeratomas in men 50 years or older to be 14% (70/500). 22 In contrast, we found that 48.2% (40/83) of W/EA men 50 years or older had genital angiokeratomas.
Although the histopathologic features of genital angiokeratomas in men and women are identical, their etiology is unknown. One theory suggests that these lesions are congenital but do not present visibly until much later in life. 19 Other theories suggest a relation to degeneration of elastic tissue surrounding blood vessels, capillary injury from trauma, or venous hypertension. 20 Although an association has been made between presence of genital angiokeratomas and varicoceles,1,2 Orvieto et al reported lack of such an association in a population of 435 young adult Israeli male soldiers age 18-19 years: Forty-six of these men had varicoceles, but none had concurrent genital angiokeratomas. 23 None of the men examined in our study were younger than 23 years.
The inheritance pattern of Fordyce angiokeratomas has not been determined. 12 Although it appears that the prevalence of genital angiokeratomas increases with age, rare cases have been noted in children.19,21 We are unaware of studies assessing the prevalence of genital angiokeratomas in prepubertal children but believe the occurrence to be uncommon (personal observation, A.R.R.).
Although generally recognized as benign, 13 genital angiokeratomas may be mistaken for benign or atypical nevi, warts, hemangiomas, keratinocytic skin cancer, and even melanoma and angiosarcoma. 24 Lesions may present with bleeding,1,3,4,11-13,17 pain,3,14,15 redness,3,16 pruritus,3,10,12,15 burning, 15 and swelling, 3 as well as psychological burden16,17 and cosmetic concerns. 18
Study Limitations
Our study sample comprised W/EA adults in one dermatologist’s outpatient clinic specializing in cutaneous melanoma and keratinocytic skin cancer. However, we are unaware of a positive or negative association between genital angiokeratomas and risk for melanoma and keratinocytic skin cancer. Numbers of non-W/EA adults were too small for statistical comparison. Additional studies will be necessary to assess prevalence of genital angiokeratomas among various racial/ethnic groups.
Additional limitations of our study were lack of precision in assessing numbers of lesions, based on naked-eye counts only. Whereas dermatoscopy was used selectively for confirmation of questionable single lesions, this method of assessment was not used for all lesions identified by the naked eye as angiokeratomas.
Conclusions
We determined that genital angiokeratomas are relatively common based on examination of a selected population of W/EA adults presenting in one senior dermatologist’s outpatient practice. Genital angiokeratomas are important to recognize because of their benign nature and occasional confusion with other tumors. Additional studies in a more general population are warranted to better determine prevalence and predisposing factors for genital angiokeratomas.
Footnotes
Acknowledgements
This study was reviewed and approved by the Rush Institutional Review Board, Master Project number 13021803.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.