
Abstract
Background
Presurgical curettage before nonmelanoma skin cancer surgery may help delineate tumor subclinical extensions.
Objective
To determine histologically whether presurgical curettage appropriately or inappropriately changes excision specimen size.
Materials and Methods
One hundred fifty consecutive nonmelanoma skin cancers treated with Mohs micrographic surgery. The clinical margin (CM) was marked. Presurgical curettage was then performed and the resultant presurgical curettage margin (PCM) marked. Frozen section analysis of the CM and PCM revealed whether the curettage-induced margin change was appropriate or unnecessary.
Results
Presurgical curettage appropriately increased the surgical margin in 9.3% of cases, reducing the number of Mohs stages from 2 to 1. It appropriately decreased the surgical margin in 17.3% thereby conserving normal skin. In 19.4% of cases the curettage increased the margin in situations where the CM had underestimated the size of the tumor; however, in these cases, the curettage did not increase the margin sufficiently to clear the tumor. In 44.0% of cases the PCM did not change the size of the stage I specimen compared to the CM and confirmed the CM. In 10.0% of cases, preoperative curettage reduced margin accuracy by removing healthy tissue (8.0%) or underestimating tumor (2.0%). These errors were associated with eyelid location, severe background photodamage, and morpheiform/infiltrating/sclerosing basal cell carcinomas.
Conclusion
Presurgical curettage can improve tumor excision accuracy and efficiency. Careful tumor selection is important to optimize curette utility.
Keywords
Introduction
Many dermatologic surgeons recommend gentle curettage of basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) before stage I of Mohs micrographic surgery or prior to excisional surgery in order to define subclinical tumor extension.1-4 In addition to stretching the skin and performing dermoscopy, light curettage may enhance assessment of tumor size and shape by detecting finger-like tumor projections. However, the efficacy of presurgical curettage has not been well established. Some researchers argue that preoperative curettage may remove normal, healing, or actinically damaged skin, creating an unnecessarily large wound.5,6 In contrast, other researchers have shown that preoperative curettage may be tumor-specific and could potentially assist in delineating the subclinical extensions of tumors.7,8 Because there are no established evidence-based guidelines or recommendations, the decision to perform presurgical curettage rests largely on an individual surgeon’s preferences, training, and personal experience. 9
The goal of curettage is to use a surgical instrument to scrape away poorly adherent tumor cells and leave behind healthy, uninvolved skin. 10 Separation of these 2 types of tissue is attributable to the increased friability of the cancerous cells compared to normal keratinocytes. This property is likely secondary to impaired adherence of the tumor cells to each other and the basement membrane, as histologic studies have demonstrated that BCC cells have increased intercellular spaces and a reduction in desmosomes required for cell-cell attachment.11,12
When using the curette, the surgeon is guided by tactile feedback between the soft, friable tumor cells and the firm resistance of normal skin. Perception of these differing textures is highly subjective, so proper and effective curettage comes only after significant experience.
When curettage increases the estimation of tumor size, the size of the specimen removed is correspondingly enlarged. This sequence of events may be appropriate if the tumor has subclinical extensions that are not appreciated on initial assessment. However, it is also possible that the upgraded estimation of tumor size may improperly remove normal, healthy tissue. The latter outcome may be more likely if the skin adjacent to the tumor is erythematous, photodamaged, and/or friable, lending it a tumor-like texture. This may lead to incorrect curettage of healthy tissue and, consequently, an overestimation of the true tumor margin.
Curettage may also decrease the estimation of tumor size and, accordingly, reduce the size of specimen removed. If the tumor is actually smaller than what was approximated clinically, the reduction in tumor size estimate may be appropriate. This decrease is inappropriate, however, if the margins are deemed positive.
This histologic study aims to determine whether presurgical curettage appropriately changes the size of the excisional specimen submitted for stage I of Mohs surgery.
Materials and Methods
One hundred fifty consecutive, biopsy-proven BCCs and SCCs were prospectively evaluated over a 5-month period from August 2018 to December 2018 at the Division of Dermatologic Surgery, Icahn School of Medicine at Mount Sinai, New York. All tumors were primary skin cancers that had not been previously treated and all were treated with Mohs surgery. Institutional Review Board approval was obtained.
Before surgery, the tumor size and shape were assessed by palpation, naked eye inspection, and dermoscopic examination (tenfold magnification with Dermlite DL3 dermatoscope, 3Gen Inc, San Juan Capistrano, CA, USA). Gentian violet was used to mark a 2 mm margin outside the clinically apparent tumor (clinical margin, CM). This inked-ring CM represented the hypothetical margin if curettage was not used. Length and width of CM were recorded in millimeters. A digital photograph was taken of the CM with a reticle lens camera focused on both the lesion and an adjacent ruler (Nikon D750, Nikon Corporation, Tokyo, Japan).
The tumor was lightly curetted with a Tiemann 5 mm sterile metal curette. A 2-mm surgical margin outside the curetted area was marked with gentian violet, confirmed with digital photography (presurgical curettage margin, PCM). The distance between the CM and PCM was measured. If there was ≥1 mm difference between the CM and the PCM in either length or width, this was considered a change in margin. If there was <1 mm difference between the CM and PCM, the margin was considered unchanged.
If there was ≥1 mm difference between the CM and the PCM, the tissue specimen excised was analyzed using frozen histopathology to detect the presence of tumor cells at the CM and PCM. Standard procedures for processing and analyzing Mohs tissue specimens were applied to the PCM: the tissue was embedded in optimal cutting temperature (frozen sectioning on microtome-cryostat 7 µm horizontal section thickness) and stained with both toluidine blue and hematoxylin and eosin. Frozen section analysis of the CM and PCM revealed whether the change in the stage I specimen size as a result of presurgical curettage was warranted or unnecessary. One-millimeter margin of tumor clearance was deemed appropriate and frozen histopathology revealed the extension of the tumor according to the scenarios outlined in Figure 1.
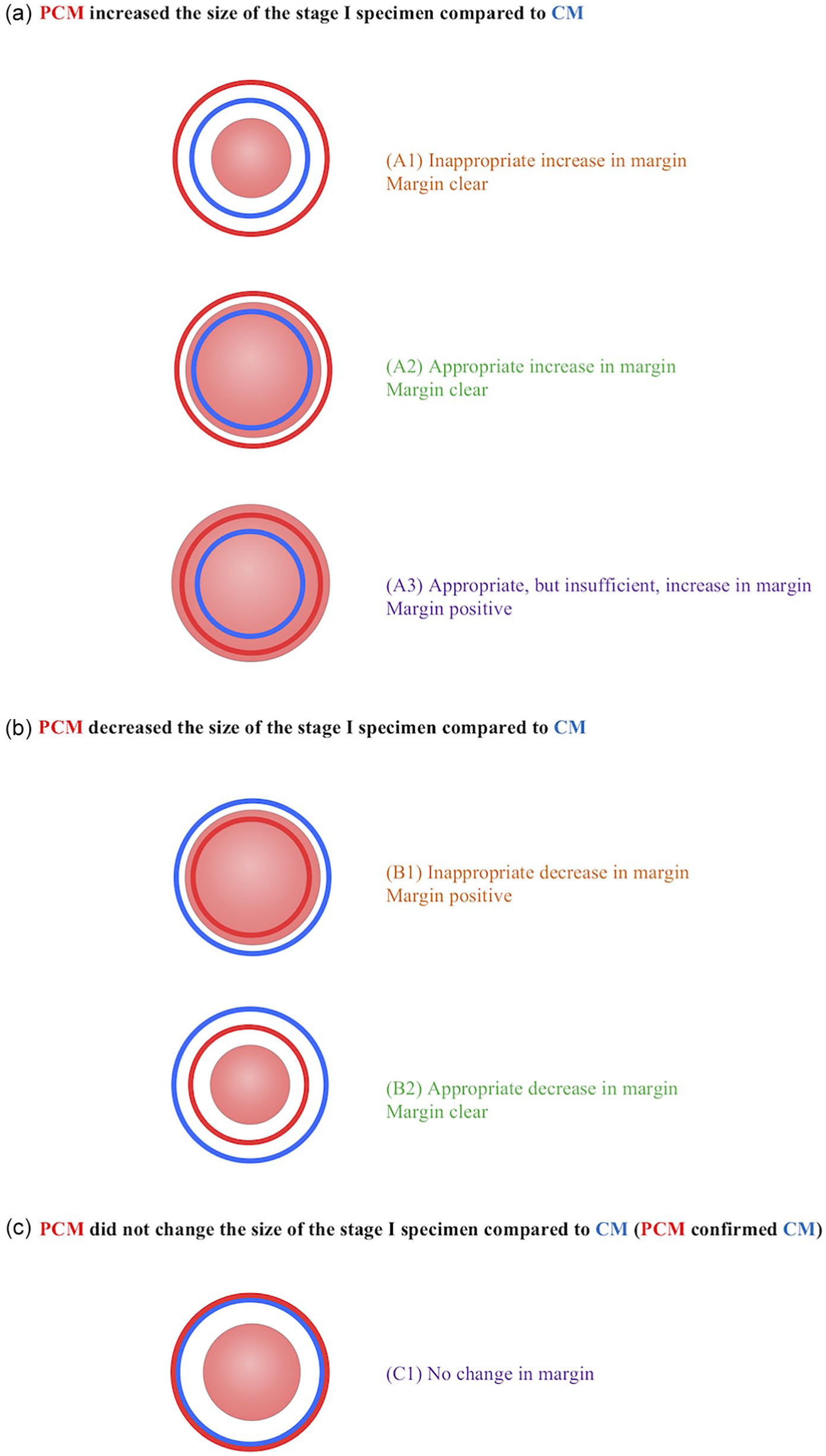
Classification of cases.
The following variables were recorded: patient age, sex, tumor maximum diameter (mm), histological subtype, and site. The tumors were categorized as either poorly defined or well defined based on clinical and dermoscopic morphology. The background skin was characterized as having nil/mild photodamage or severe photodamage. Three surgeons (D.K., H.K., and M.J.L.) with 32, 14, and 6 years of experience performed the presurgical curettage and Mohs procedures. Univariate logistic regression was performed using SPSS Statistics Version 20.0 (IBM, Armonk, NY, USA).
Results
There were 150 cases with a median age of 56 (range 26-94) and a male-to-female ratio of 1.27. The median tumor diameter was 10 mm (range 5-35 mm). Sixty-four percent were BCCs and 36.0% were SCCs. Of the 96 BCCs, the primary subtype pattern was nodular in 40.2%, micronodular in 20.2%, superficial in 24.0%, and morpheiform/infiltrating/sclerosing in 15.6%; 6.3% of these BCCs had a mixed pattern. Seventy-six percent of tumors were located on the head and neck: scalp (6.0%), forehead (24.7%), nose (14.0%), eyelid (6.7%), cheek (6.7%), lip (3.3%), ear (6.7%), and neck (8.0%). Other tumors were located on the upper limb (5.3%), lower limb (13.3%), and trunk (5.3%). Tumors were cleared with 1 Mohs stage in 46.7%, 2 Mohs stages in 43.3%, 3 Mohs stages in 6.7%, 4 Mohs stages in 2.0%, and 5 Mohs stages in 1.3%.
Presurgical curettage appropriately increased the surgical margin in 9.3% of cases and reduced the number of Mohs stages from 2 to 1 (Figure 2). It appropriately decreased the surgical margin in 17.3%, thereby conserving normal skin. Factors associated with useful presurgical curettage were non-eyelid location (other sites vs. eyelids, odds ratio [OR] = 2.32, P = .03) and nil/mild photodamage (nil/mild photodamage vs. severe photodamage, OR = 1.82, P = .05). Sex, age, tumor type (BCC vs. SCC), tumor definition (well defined vs. poorly defined), tumor size, and surgeon were not associated with useful or inaccurate surgical curettage.
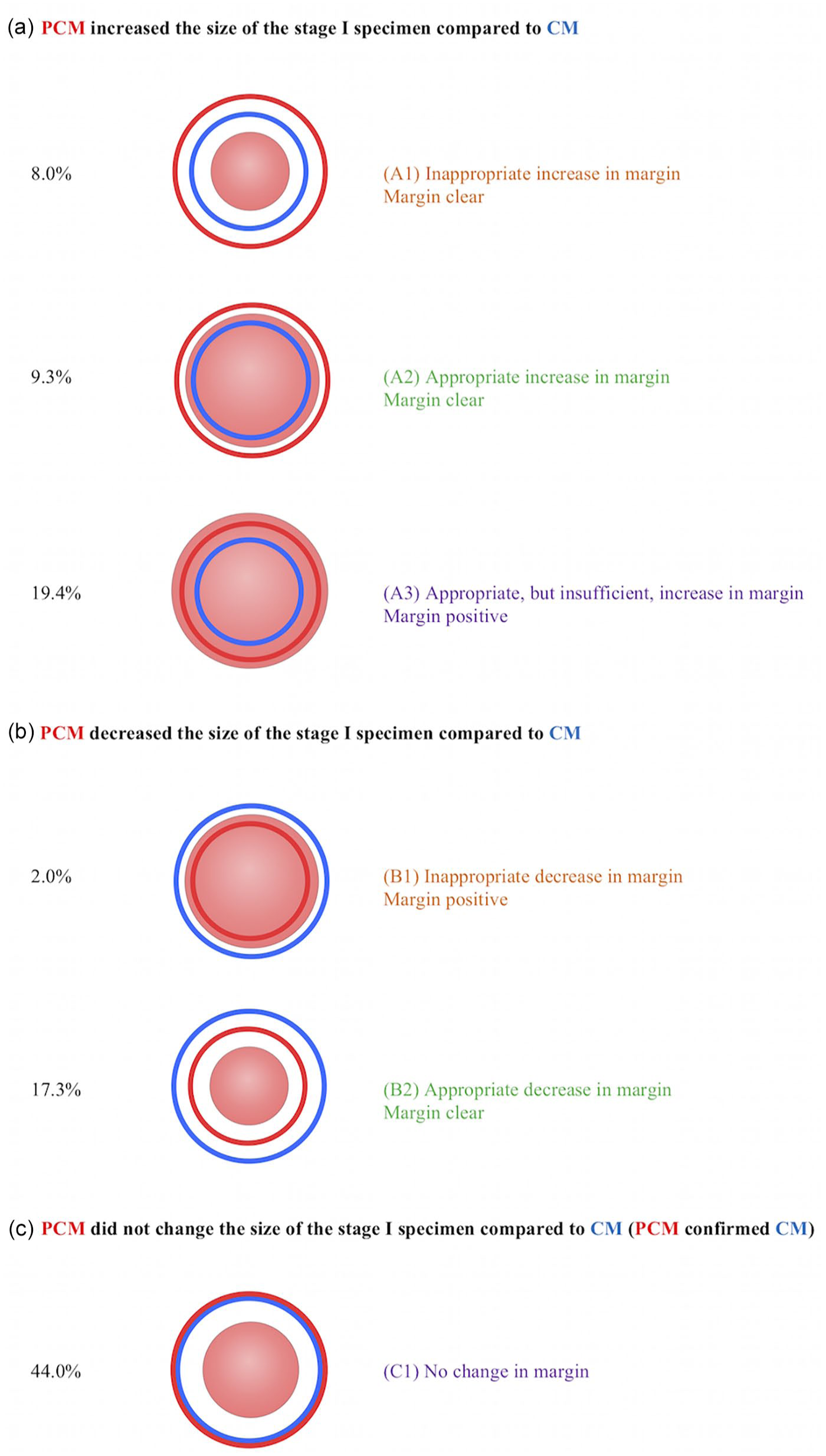
The impact of presurgical curettage on the accuracy of surgical margins.
In 19.4% of cases the curettage increased the margin in situations where the CM had underestimated the size of the tumor; however, in these cases, the curettage did not increase the margin sufficiently to clear the tumor (ie, PCM was more accurate than the CM but still not accurate enough to perfectly delineate the tumor). In 44.0% of cases the PCM did not change the size of the stage I specimen compared to the CM. In these cases the PCM confirmed the CM.
In 10.0% of cases, preoperative curettage reduced margin accuracy by removing healthy tissue (8.0%) or underestimating tumor (2.0%). These errors were commonly associated with tumors located on the eyelids or patients with severe background photodamage. Additionally, subanalysis revealed that, when compared to nodular/micronodular/superficial BCCs, BCCs with morpheiform/infiltrating/sclerosing histology were also associated with less accurate curettage (OR = 5.23, P < .01).
Discussion
In contrast to the established therapeutic efficacy of aggressive curettage for the treatment of skin cancer,13-22 gentle curettage as a preliminary step to determine the subclinical extensions of a tumor margin has not been well documented. In this study we found that presurgical curettage appropriately increased the surgical margin in 9.3% of cases and appropriately decreased the surgical margin in 17.3%. Proper case selection is important because site (non-eyelid skin vs. eyelid skin), background photodamage (nil/mild vs. severe), and BCC subtype (nodular/micronodular/superficial vs. morpheiform/infiltrative/sclerosing) were associated with improved curette accuracy. These findings provide evidence that with appropriate case selection, this simple, quick, and inexpensive technique may allow surgeons to better delineate subclinical tumor and improve excision accuracy. Although our analysis was performed only on Mohs surgeries, the benefit of presurgical curettage may have the potential to extend to other excisional surgeries by better delineating subclinical extension of tumors and guiding surgical margins.
Curettage improved surgical margin accuracy by appropriately increasing the margin and clearing the tumor in 9.3% of cases. In these cases, the blunt curette detected invisible strands of the cancer that extended beyond the clinical and dermoscopic boundaries. This allowed for a reduction in the number of Mohs stages from 2 to 1 for these cases, a finding consistent with other studies that support the efficacy of presurgical curettage in reducing the number of Mohs stages needed for tumor extirpation.7,8,23 A decrease in the number of Mohs stages from 2 to 1 has been correlated with a quantifiable, significant economic benefit due to time and cost savings. 23 Additionally, fewer Mohs stages lessen patient discomfort and anxiety.
In 17.3% of cases where clinical assessment overestimated the tumor margins, curettage increased surgical margin accuracy by appropriately reducing the size of the excision and conserving normal skin. This implies that presurgical curettage may be useful in reducing the size of the final defect and the resultant scar. Decreased scarring is one of the aims of dermatologic surgery; therefore, curettage was critical in optimizing surgical results for these select cases.
Preoperative curettage confirmed the CM and did not change the size of the excision by more than 1 mm for 44.0% of the tumors. No harm was incurred by performing this quick, simple procedure and confirmation of tumor size provided the surgeon with a more confident assessment of the appropriate margin for excision.
For 10% of tumors, preoperative curettage was detrimental in that it reduced surgical margin accuracy by either inappropriately removing healthy tissue (8.0%) or incorrectly decreasing the surgical margin (2.0%). Unhelpful curettage was more likely to occur in the following situations: severe background actinic damage, tumors on the eyelid and morpheiform/infiltrative/sclerosing BCC. These factors, therefore, represent relative contraindications to presurgical curettage and reinforce the necessity of appropriate case selection to optimize the utility of this clinical tool.
The authors do not recommend routinely curetting tumors in areas with severe actinic damage, as tactile differentiation between tumor and normal skin is dampened in these regions due to the gritty, friable textures of both types of tissue. Curetting in these instances may, therefore, result in an overestimation of the tumor margin into the surrounding actinically damaged skin. This finding is consistent with other studies, which reported that curetting actinically damaged areas may create unnecessary large wounds.5,6
A randomized controlled study by Huang et al reported that presurgical curettage resulted in unnecessary removal of normal, healthy tissue. 5 The investigators examined 79 cases that underwent presurgical curettage and compared them to 87 cases that were not curetted. In the preoperative curettage group, there was an absolute surface area increase of 1.78 cm2 (95% confidence interval [CI], 1.57-1.99) between the true tumor size and the stage I wound. The control group, which did not undergo curettage, demonstrated only a 1.40 cm2 (95% CI, 1.15-1.65) increase in absolute surface area. This 0.38 cm2 difference led the investigators to conclude that preoperative curettage may result in a defect that is larger than the actual margin of the tumor, suggesting unnecessary removal of normal skin. However, Huang et al did not report on the level of background actinic damage and studied a different population. Their study described older patients and only included BCCs less than 2 cm in diameter located on the head and neck.
The authors do not recommend routine curettage of eyelid skin. Eyelid skin is the thinnest skin on the entire body and is inherently challenging to curette. 24 It is too easy to remove normal eyelid skin with the curette and, for this reason, it is not an accurate tool in this location.
Morpheiform/infiltrative/sclerosing BCCs are also challenging to curette because they lack the same level of friability as nodular or superficial BCCs. The absence of this unique texture may be attributed to the structure of morpheiform/infiltrative/sclerosing BCCs, because these tumors are composed of thin strands of cancer cells interspersed diffusely throughout the dermis. This causes the unhealthy tissue to feel firm during curettage, rendering it difficult to distinguish from normal skin. As such, the authors do not recommend routine curettage of these particular BCC subtypes. This stands in contrast to nodular and superficial BCCs, which have the greatest potential to benefit from presurgical curettage.
Although recurrent tumors were excluded from our study protocol, in our experience presurgical curettage is less useful in recurrent tumors. Curetting a recurrent tumor yields the same feel as normal skin because it is composed of fibrous tissue.
It is acknowledged that presurgical curettage is operator dependent and that there is a learning curve associated with the technique. The curettage is guided by the physical sensation of the curette against friable tumor tissue, which is distinguished from the “feel” of normal skin. As Arpey described, when curetting before Mohs surgery, the attitude should be of “exploration” rather than “destruction” because all margins will ultimately be examined. 4 Overly aggressive pressure or extended strokes may produce superficial abrasion of surrounding normal epidermis, which would lead to a unnecessarily large Mohs stage I. Overly light curettage could result in an underestimation of the tumor positive margins. Thus, there is a learning curve associated with the use of the curette, and the efficacy of preoperative curettage may vary with the aggressiveness of an individual surgeon’s technique.
A limitation of our study and previous studies on this topic is that the size of CM and PCM was based on length and width and grounded on the assumption that the tumor was round and reasonably symmetrical. There may have been irregular strands of tumor that were not accounted for by our method. Furthermore, the curettage in the study was performed using a Tiemann 5 mm metal curette, so the results can be applied only to this particular curette. We cannot make recommendations for use of other types of curettes. From the authors’ experience, we have found that the disposable curettes are sharper, which may lead to overestimation of the tumor margins and induce collateral tissue damage. The plastic handle on the disposable curette is also more flexible, which lends a different “feel” to the curetting process. In the future, we hope to include data from different curettes to determine which instruments provide the best estimation of tumor size and shape.
Conclusion
Presurgical curettage is a simple, inexpensive procedure that can improve the accuracy and efficiency of tumor excision for the majority of cases. Tumor selection is of paramount importance because of the inaccurate results associated with curettage on the eyelid, severely photodamaged skin, and morpheiform/sclerosing/infiltrative BCCs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Status
Institutional Review Board of the Mount Sinai School of Medicine (HS#: 18-01263)