
Abstract
This document is intended to provide practical guidance to physicians treating pediatric atopic dermatitis (AD), especially dermatologists, pediatricians, allergists, and other health-care professionals. The recommendations contained here were formalized based on a consensus of 12 Canadian pediatric dermatologists, dermatologists, pediatricians, and pediatric allergists with extensive experience managing AD in the pediatric population. A modified Delphi process was adopted with iterative voting on a 5-point Likert scale, with a prespecified agreement cutoff of 75%. Topic areas addressed in the 17 consensus statements reflect areas of practical management, including counselling, assessment, comorbidity management, and therapy.
In recent years, there has been an increase in our understanding of the disease impact and pathogenesis of atopic dermatitis (AD), which has led to a rapidly evolving treatment landscape. Because AD can present very differently in adults and children, there is a need for up-to-date, practical, and clinically relevant guidance for both pharmacologic and nonpharmacologic treatment considerations in pediatric AD. The present document is intended to provide guidance to physicians treating pediatric AD, especially dermatologists, pediatricians, allergists, and other health-care providers (HCPs).
Topic areas addressed in the final 17 consensus statements reflect areas of practical management, including counselling, assessment, comorbidity management, and therapy. It is the intent of the authors that these statements will help guide clinical decision-making and optimize care for pediatric patients with AD. A summary of the statements and voting results is provided in Table 1.
Final Consensus Statements and Voting Results. a
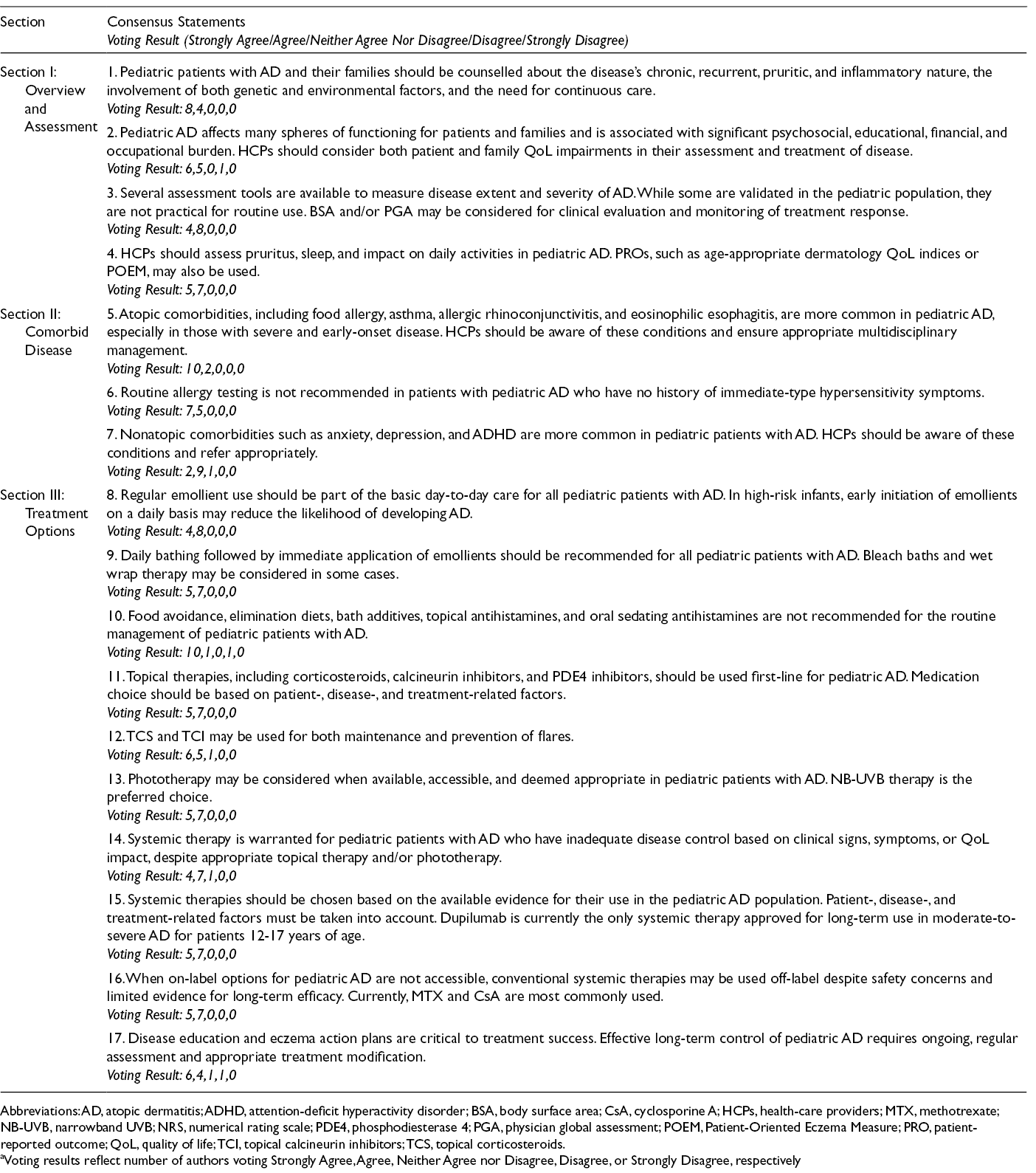
Abbreviations: AD, atopic dermatitis; ADHD, attention-deficit hyperactivity disorder; BSA, body surface area; CsA, cyclosporine A; HCPs, health-care providers; MTX, methotrexate; NB-UVB, narrowband UVB; NRS, numerical rating scale; PDE4, phosphodiesterase 4; PGA, physician global assessment; POEM, Patient-Oriented Eczema Measure; PRO, patient-reported outcome; QoL, quality of life; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids.
aVoting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively
Methods
A working group was formed consisting of 12 Canadian pediatric dermatologists, dermatologists, pediatricians, and pediatric allergists with extensive experience managing AD in the pediatric population. All authors declared conflicts of interest, and none were deemed to preclude their participation in this publication. The consensus-building process used by our group follows the same process as a previously published consensus document for adult AD. 1
Based on gaps identified by our group in the disease management literature, three topic areas of interest related to pediatric AD were identified: (1) overview and assessment of pediatric AD, (2) comorbid disease, and (3) treatment options. As a basis to guide content development for this document, and in order to provide an evidence framework for the consensus statements, structured PubMed literature searches were conducted in February 2019 for each of the three sections. Authors agreed on search parameters and identified keywords, considering articles published in the past five years. Search results were filtered for English-language articles plus limited to studies conducted in humans and relevant to the pediatric AD population. A manual search of relevant additional literature was performed as needed. This library, along with the authors’ expertise and experience, served as the basis for content development and the clinical recommendations contained in each section of this publication (Appendix A). Sections I-III of this manuscript series include narrative summaries of the literature reviews. These manuscripts may be consulted for a summary of the literature considered by our group. 2 -4
Experts reviewed and aligned on the draft manuscript content at a meeting held in Toronto, Canada on May 11, 2019. At this meeting, a summary of the literature was presented by the authors, and the panel voted on 18 initial consensus statements based on the three identified topic areas. Using a modified Delphi approach, an iterative process of review, voting, discussion, and amendment took place as required, until the final statements achieved consensus.
Voting was captured anonymously on a 5-point Likert scale, with responses ranging from strongly agree to strongly disagree, and a prespecified cutoff of 75% agree or strongly agree was required to achieve consensus. A final result of 17 consensus statements was agreed on by the expert panel. The voting results for all statements failing to achieve consensus are captured in supplemental Table S1.
Overview and Assessment of Pediatric AD
Consensus: 100% (Voting Result*: 8,4,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
This expert panel agreed on highlighting the chronic inflammatory nature of AD, with pruritus noted as a major diagnostic criterion. HCPs should help patients and caregivers understand that AD is a recurrent and relapsing condition, and although the disease may go into periods of remission, it is important to be proactive about management in order to minimize future flares. This may include avoidance of triggers and maintenance therapy. Disease pathology is complex and affected by both genetic and environmental factors that drive immune dysregulation, skin barrier dysfunction, and altered microbiome.
Consensus: 92% (Voting Result*: 6,5,0,1,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
The burden of pediatric AD includes many factors impacting the whole family. In addition to financial burden of disease, patients and families suffer physical and mental impairment, including impact on productivity at work or school. AD affects family dynamics and functioning as well. These significant impacts highlight the need to take these factors into consideration when deciding on management.
Consensus: 100% (Voting Result*: 4,8,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Clinical evaluation of disease extent and severity should be based primarily on physician assessment, since no single assessment tool sufficiently captures this in a clinically practical manner. In addition to clinical assessment, BSA may be used to measure extent of disease and PGA to measure dermatitis severity in a clinical setting, allowing physicians to evaluate baseline disease and response to therapy over time.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Although PROs are helpful and capture different dimensions of disease severity and complexity, they should be used as a complement to clinical evaluation. Pruritus and sleep disturbance are important subjective outcomes to consider during AD assessment. Various QoL questionnaires exist and age-appropriate assessments, completed by the patient or caregiver, may be used in conjunction with family impact questionnaires to capture the significant burden on families that is often understated in the literature. These include age-appropriate Dermatology Life Quality Index (DLQI) instruments, including Children’s DLQI (CDLQI) and Infant’s DLQI (IDLQI), as well as the Dermatitis Family Impact instrument (DFI), the Children’s AD Impact Scale (CADIS), and the Infants’ Dermatitis Quality of Life Index (IDQOL).
Comorbid Disease in Pediatric AD
Consensus: 100% (Voting Result*: 10,2,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
HCPs should be aware of atopic comorbidities that commonly present or develop in pediatric patients with AD. These include food allergy, asthma, allergic rhinoconjunctivitis, and eosinophilic esophagitis. Ocular disorders, both allergic and nonallergic, are also possible comorbidities. Assessment and referral may be indicated, when appropriate.
Consensus: 100% (Voting Result*: 7,5,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Although other atopic conditions may commonly develop in pediatric patients with AD, testing for food allergy is only recommended in patients with a history of immediate-type hypersensitivity symptoms such as wheals, urticaria, erythema reactions, wheezing, and anaphylaxis. Referral to an appropriate specialist may be considered based on clinical judgment. When indicated, allergy testing may include skin prick testing and/or serologic assays for food-specific immunoglobulin E (IgE) antibodies. It is important to note that immunoglobulin G (IgG) testing is not a validated diagnostic test for food allergies and should not be recommended.
Consensus: 92% (Voting Result*: 2,9,1,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Psychosocial impacts, effects on family functioning, disturbance of school performance, sleep loss, and impairment of daily functioning should be considered during pediatric AD assessment. It is also important for HCPs to be aware of the increased risk of suicidal ideation in pediatric AD patients. Screening and appropriate management, which may include specialist referral, is advised. Treatment of disease symptoms can reduce the psychosocial impact.
Treatment Options for Pediatric AD
Consensus: 100% (Voting Result*: 4,8,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Even in the absence of active disease, the chronic nature of AD requires ongoing basic care to maintain the skin barrier and prevent future flares. Early daily use of emollients has been shown to reduce or delay the onset of AD and the importance of their regular use should be highlighted to patients and caregivers during counselling.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Regular bathing is an important part of basic care for pediatric AD, even in episodes of remission, to prevent flares. Regular bathing is defined by this group as daily bathing, when tolerated. The preference is to use fragrance-free, pH-neutral, hypoallergenic cleansers. Emollients should be applied immediately after bathing to maintain a healthy skin barrier. Bleach baths and wet wrap therapy are not part of routine treatment but may be considered when appropriate. Specifically, wet wrap therapy may be used as short-term rescue therapy for severe AD flares. Bleach baths have not been consistently shown to improve outcomes in AD and may be used at the discretion of the treating HCP.
Consensus: 92% (Voting Result*: 10,1,0,1,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
There was strong consensus that several therapeutic strategies commonly tried by patients with AD are not effective in treating disease and may lead to negative outcomes. Food avoidance and elimination diets are not routinely recommended in the absence of specific food allergy nor advised, particularly in younger children. There is no evidence for the use of bath additives in managing signs and symptoms of AD; in fact, some ingredients may aggravate disease or lead to irritant and allergic contact dermatitis. Topical and oral antihistamines have little evidence to support their use. Oral first-generation antihistamines have adverse effects including prolongation of QT interval and sedation. They may interfere with school performance and/or driving in adolescents. Oral second-generation antihistamines used in management of pruritus do not have any added benefit in the treatment of AD.
There was strong consensus that several therapeutic strategies commonly tried by patients with AD are not effective in treating disease and may lead to negative outcomes. Food avoidance and elimination diets are not routinely recommended in the absence of specific food allergy nor advised, particularly in younger children. There is no evidence for the use of bath additives in managing signs and symptoms of AD; in fact, some ingredients may aggravate disease or lead to irritant and allergic contact dermatitis. Topical and oral antihistamines have little evidence to support their use. Oral first-generation antihistamines have adverse effects including prolongation of QT interval and sedation. They may interfere with school performance and/or driving in adolescents. Oral second-generation antihistamines used in management of pruritus do not have any added benefit in the treatment of AD.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Although topical corticosteroids (TCS) are traditionally indicated as a first-line treatment in pediatric AD, this group agreed that TCS do not need to be the only first-line topical considered and that the use of topical therapies need not be approached in a stepwise manner. Topical calcineurin inhibitors (TCI) and PDE4 inhibitors can be used as first-line treatment in select cases where corticosteroid use is not ideal, including sensitive areas such as the face and intertriginous areas. TCI are not well tolerated on very inflamed skin as burning and stinging may occur with application. However, they are safe to use long-term on all areas of the body. TCS failure is related to nonadherence and corticosteroid phobia; therefore, patients and caregivers should be appropriately counselled to ensure therapy compliance.
Consensus: 92% (Voting Result*: 6,5,1,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Maintenance therapy and flare prevention in pediatric AD can be achieved with intermittent therapy with TCS or TCI. This is a valuable strategy in pediatric AD patients.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Phototherapy is an option to treat flares either during or after topical therapy; however, practical considerations such as accessibility, convenience, and patient temperament and maturity should be taken into account. Accessibility is an issue and often implies missed time from school or work to attend sessions, both for the patient and the caregivers. There is also an unconfirmed risk of photocarcinogenesis and photoaging that prevents some HCPs from adopting this practice, especially as a long-term treatment strategy.
Consensus: 92% (Voting Result*: 4,7,1,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Systemic therapy may include oral noncorticosteroid immunosuppressants such as methotrexate (MTX), cyclosporine A (CsA), azathioprine (AZA), and mycophenolate mofetil (MMF); oral corticosteroids such as prednisone; and targeted therapies such as dupilumab. Most are used off-label in treating pediatric AD, with the exception of dupilumab, CsA, and oral corticosteroids in some countries. It is important to note that although oral corticosteroids are approved for use in AD, they should be reserved for rescue treatment only due to long-term safety concerns.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
When first-line topical therapies fail, systemic immunosuppressive therapies have often been used off-label to treat moderate-to-severe cases of pediatric AD, with limited efficacy and safety data related to their use, particularly in the pediatric AD population. At this time, dupilumab is the only systemic therapy approved for long-term treatment of moderate-to-severe AD in patients 12-17 years of age and should be considered first-line for this age group.
Consensus: 100% (Voting Result*: 5,7,0,0,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Conventional systemic therapies, including oral immunosuppressive agents, such as MTX, CsA, AZA, and MMF, may be considered in patients with moderate-to-severe disease when on-label therapies are not accessible or appropriate. MTX and CsA are the most commonly used, and while there is limited evidence to support their use in pediatric AD, they are relatively well tolerated and efficacious based on clinical experience. MTX is commonly used due in part to its low cost, and CsA may be considered for flare management due to its relatively rapid onset of action. The use of CsA should be limited to less than one year based on long-term safety concerns related to nephrotoxicity and carcinogenesis.
Consensus: 83% (Voting Result*: 6,4,1,1,0)
*Voting results reflect number of authors voting Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, or Strongly Disagree, respectively.
Disease education includes patient and caregiver counselling by specialists treating AD, as well as corresponding education and appropriate counselling by primary care HCPs and pharmacists when relevant. Written eczema action plans may be helpful to increase adherence to treatment and decrease treatment failure. A pictogram action plan can be especially helpful in young children. Treatment response should be regularly monitored and modified based on treatment response, tolerability, and patient satisfaction.
Supplemental Material
Appendix - Supplemental material for Approach to the Assessment and Management of Pediatric Patients With Atopic Dermatitis: A Consensus Document. Section IV: Consensus Statements on the Assessment and Management of Pediatric Atopic Dermatitis
Supplemental material, Appendix, for Approach to the Assessment and Management of Pediatric Patients With Atopic Dermatitis: A Consensus Document. Section IV: Consensus Statements on the Assessment and Management of Pediatric Atopic Dermatitis by Perla Lansang, Irene Lara-Corrales, James N. Bergman, Chih-ho Hong, Marissa Joseph, Vy H.D. Kim, Joseph M. Lam, Ian Landells, Danielle Marcoux, Vimal H. Prajapati, Michele L. Ramien and Shanna Spring in Journal of Cutaneous Medicine and Surgery
Supplemental Material
Supplementary Table 1 - Supplemental material for Approach to the Assessment and Management of Pediatric Patients With Atopic Dermatitis: A Consensus Document. Section IV: Consensus Statements on the Assessment and Management of Pediatric Atopic Dermatitis
Supplemental material, Supplementary Table 1, for Approach to the Assessment and Management of Pediatric Patients With Atopic Dermatitis: A Consensus Document. Section IV: Consensus Statements on the Assessment and Management of Pediatric Atopic Dermatitis by Perla Lansang, Irene Lara-Corrales, James N. Bergman, Chih-ho Hong, Marissa Joseph, Vy H.D. Kim, Joseph M. Lam, Ian Landells, Danielle Marcoux, Vimal H. Prajapati, Michele L. Ramien and Shanna Spring in Journal of Cutaneous Medicine and Surgery
Footnotes
Acknowledgments
Anna Czerwonka, BSc, and Tracy Chew, PhD, of FUSE Health (Toronto, ON) provided professional medical writing services and organizational support for this manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PL has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for AbbVie, Amgen, Astellas, Boehringer Ingelheim, Celgene, Eli Lilly, Galderma, Janssen, LEO Pharma, Novartis, Pfizer, Sanofi Genzyme, and Valeant.
ILC has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for AbbVie, Avicanna, Amgen, Eli Lilly, Janssen, Johnson & Johnson, Novartis, Pfizer, Pierre Fabre, Sanofi Genzyme, and Valeant.
JNB has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for Aralez, Cipher, Dermtek, Galderma, GlaxoSmithKline, Janssen, Johnson & Johnson, La Roche Posay, LEO Pharma, Mead Johnson, Nestlé, Novartis, Pediapharm, Pierre Fabre, Pfizer, Sanofi Genzyme, and Valeant.
CHH has been an investigator, speaker, advisor and/or consultant for AbbVie, Amgen, Actelion, Akros, Bausch Health, Boehringer Ingelheim, Bristol Meyers Squibb, Celgene, Eli Lilly, Galderma, GSK, Incyte, Janssen, LEO Pharma, Medimmune, Merck, Novartis, Pfizer, Roche, Roivant Sciences, Regeneron, Sanofi Genzyme, UCB, and Valeant.
MJ has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for LEO Pharma, Pfizer, and Sanofi Genzyme.
VHDK has served as an advisor/consultant for and has received grants/honoraria from Sanofi Genzyme.
IL has served as a consultant, conducted clinical research, or received honoraria from Abbvie, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Galderma, GSK-Stiefel, Janssen, LEO Pharma, Merck, Novartis, Pfizer, Sanofi Genzyme, and Valeant.
JML has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for Cipher, Galderma, Johnson & Johnson, PediaPharm, Pfizer, Pierre Fabre, Sanofi Genzyme, and Valeant.
DM has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for Abbvie, Celgene, LEO Pharma Canada, Eli Lilly, Pfizer and Sanofi Genzyme.
VHP has served as an advisor/consultant for, has received grants/honoraria from, and/or has served as a speaker for Abbvie, Actelion, Amgen, Aralez, Asana, Aspen, Bausch Health, Celgene, Cipher, Eli Lilly, Galderma, GlaxoSmithKline, Homeocan, Incyte, Janssen, LEO Pharma, L’Oréal, Novartis, Pfizer, Regeneron, Sanofi Genzyme, Tribute, and Valeant.
MLR has served as an advisor/consultant for and/or has received grants/honoraria from LEO Pharma, Pfizer, and Sanofi Genzyme.
SS has received grants/honoraria from Abbvie, Amgen, Aralez, Bausch Health, Eli Lilly, Janssen, LaRoche Posay, LEO Pharma, Novartis, Pfizer, Pierre Fabre, Sanofi Genzyme, and Valeant, and has served as a speaker for Pfizer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sanofi Genzyme provided financial support for the planning, professional medical writing, and publication of the manuscript. Sanofi Genzyme had no role in content development for the publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.