
Abstract
Background
Oral cavity cancers (OCCs) and oropharyngeal cancers (OPCs) continue to be a major source of morbidity and mortality worldwide requiring the shared effort of numerous specialists. Tobacco and alcohol consumption have long been identified as risk factors for both OCC and OPC. In addition, human papilloma virus (HPV) is gaining its position as the main causal agent for OPC.
Objective
The objective of this study is to analyze the epidemiology of OCC and OPC in Canada.
Methods
Data pertaining to the year of diagnosis, the patient’s sex, age at the time of diagnosis, province/territory, city and postal code of oral cavity, and oropharyngeal malignancies diagnosed during 1992-2010 were extracted from the Canadian Cancer Registry and Le Registre Québécois du Cancer.
Results
In total, 21 685 OCC cases and 15 965 OPC cases were identified from 1992 to 2010. Of those, 84.97% were oral cavity squamous cell carcinomas (SCCs), 88.10% were oropharyngeal SCCs, and both had a significant male predominance. While oral cavity SCC incidence stabilized over the study period, oropharyngeal SCC continued to increase. Oral cavity SCC incidence increased with age, while oropharyngeal SCC incidence peaked in the 50- to 59-year age group. Detailed geographic distribution analysis of patients at the provincial/territorial, city, and postal code levels identified several patient clusters.
Conclusions
This work highlights important epidemiological differences in trends between oral and oropharyngeal cancers, identifies high-incidence postal codes for each malignancy, and correlates incidence/mortality with known risk factors including alcohol/tobacco use and HPV infections, therefore providing a comprehensive understanding of epidemiology for these cancers in Canada.
Keywords
Introduction
Oral cavity cancers (OCCs) and oropharyngeal cancers (OPCs) continue to be a major source of morbidity and mortality worldwide, requiring the shared effort of numerous specialists including otolaryngologists, oncologists, dentists, dermatologists, family physicians, and other specialists in oral medicine. Anatomically, the oral cavity and oropharynx are distinct regions that border each other but do not overlap. 1 Recent evidence supports that tumors arising at these 2 sites have differing etiopathogenesis, treatment, and prognosis. 2 Thus, in this study, we will compare and contrast findings for these two sites.
Tobacco and alcohol consumption have long been identified as risk factors for both OCC and OPC. 3 -5 In addition, human papilloma virus (HPV) is now an established causal agent for OPC. 6 Studies performed in the United States have identified important differences in demographic characteristics between OCC and OPC. 7 Although studies have examined epidemiological differences in oral cavity and oropharyngeal carcinomas in certain Canadian provinces, 8 -10 analyses comparing and contrasting the distribution of the aforementioned malignancies in all Canadian provinces have yet to be performed.
The objective of this registry-based study is to provide a comprehensive description of the incidence and mortality trends for oral cavity and oropharyngeal squamous cell carcinomas (SCCs) across Canada during 1992-2010. These findings could help direct public health programs and provide physicians with data to complement their clinical expertise to help better identify patients at risk for these important malignancies.
Methods
This study was conducted in accordance with the CISS-RDC-668035 and 13-SSH-MCG-3749-S001 protocols approved by the Social Sciences and Humanities Research Council of Canada (SSHRC) and the Québec Inter-University Centre for Social Statistics (QICSS), respectively. This study was exempt from the McGill University Research Ethics Board review in accordance with the institutional policy. Incidence and mortality data for oral cavity and oropharyngeal malignancies were extracted from 3 distinct but complementary population-based cancer databases (Canadian Cancer Registry [CCR], Le Registre Québécois du Cancer [LRQC], and Canadian Vital Statistics [CVS]) using the previously reported and established methods. 11 -34
From the CCR and LRQC databases, demographic, geographic, and clinical information on patients diagnosed with cancer, including sex, year of diagnosis, age at the time of diagnosis, Forward Sortation Area (FSA) of residence, and the ICD-O-3 code of the tumor were extracted. In Canada, postal codes consist of letters and numbers (eg, H3G 1A4), where the FSA defines a geographic region in which all postal codes start with the same 3 entries. The CCR (2014 version) database provides data on all malignancies diagnosed in Canada from 1992 to 2013 except for those in the province of Quebec (QC). Information pertaining to QC cancer patients was retrieved from the LRQC which provides data from 1992 to 2010. Hence, our analysis was limited to the years 1992-2010 in order to include all 10 Canadian provinces and 3 territories.
Oral cavity and oropharyngeal SCC cases were defined based on the International Classification of Diseases for Oncology, Third Edition as the following: Verrucous carcinoma (ICD-O-3 code: 8051), Papillary SCC (8052), SCC, NOS (8070), SCC, keratinizing, NOS (8071), SCC, large cell, nonkeratinizing, NOS (8072), SCC, small cell, nonkeratinizing (8073), SCC, spindle cell (8074), SCC, microinvasive (8076), Lymphoepithelial carcinoma (8082), and Basaloid SCC (8083). In addition, a few cases of Papillary carcinoma, NOS (8050), SCC, adenoid (8075), SCC, clear cell type (8084) were identified for oral cavity site, but not oropharyngeal. The 2018 updated ICD-O-3 table included histology codes 8085 and 8086 that encode HPV-positive and HPV-negative SCC, respectively. However, there is no available data on HPV-related types of SCC within the examined range of 1992 to 2010. Anatomical site codes used for the oral cavity and oropharynx were reported as in the previous studies (Supplemental Table S1). 8,10
Malignancy-associated mortality was performed by extracting data from the CVS database. Codes from the International Statistical Classification of Diseases and Related Health Problems, ninth revision (ICD-9) and tenth revision (ICD-10) were used for deaths between 1992-1999 and 2000-2010, respectively. Unfortunately, deaths are only reported by anatomical site and do not differentiate between different morphologies of cancers. Hence, we were unable to specifically analyze SCCs. Nevertheless, given that SCCs accounted for the great majority of all malignancies in the oral cavity and oropharynx, we proceeded with these analyses based on anatomical sites (Supplemental Table S2).
Raw data were rounded in accordance with the rules put forward by the SSHRC/Statistics Canada to maintain confidentiality. Each cell count was rounded, independent of other cells, to a lower or higher multiple of 5 using a random rounding system. Only counts of 0 and ≥5 could be released.
Unless otherwise specified, the Canadian Census of Population for 1996, 2001, 2006, and 2011 were used to calculate average population size during the associated time period. Forward Sortation Areas with population of <5000 individuals and cities with population of <50 000 individuals based on the census data were excluded to reduce the likelihood that a few cases of malignancies within a scarcely populated area may artificially inflate or deflate the incidence or mortality rate. 95% Confidence intervals (CIs) for the incidence rates were calculated using exact Poisson tests for each geographic region. Statistical significance was defined by 95% CI not overlapping with that of the national average 95% CI. Geographic regions with statistically significant cancer rates were mapped using geographic information systems software.
Results
The clinical and demographic characteristics of Canadian oral cavity and oropharyngeal cancer patients were examined using 2 population-based health registries, namely the CCR and LRQC. In total, 21 685 cases of OCC and 15 965 cases of OPC were identified from 1992 to 2010. Of those, the majority were SCCs: 84.97% of oral cavity malignancies were oral cavity SCC and 88.10% of oropharyngeal malignancies were oropharyngeal SCC (Supplemental Table S2).
Demographic Characteristics of Canadian Oral Cavity and Oropharyngeal SCC Patients
Approximately 18 420 patients were diagnosed with oral cavity SCC in Canada during the period 1992-2010. These cases predominantly consisted of SCC, NOS (8070), and SCC, keratinizing, NOS (8071) representing 73.28% and 19.89% of oral cavity SCC cases, respectively. Approximately 14 055 patients were diagnosed with oropharyngeal SCC in Canada during the period 1992-2010 (Supplemental Table S2). Like oral cavity cancers, these cases predominantly consisted of SCC, NOS (8070), and SCC, keratinizing, NOS (8071) representing 76.06% and 12.17% of all oropharyngeal SCC cases, respectively.
The greatest proportion of oral cavity SCC were diagnosed in the eldest age group of ≥90 years, with the steepest rise in incidence in the 50- to 69-year age group. Conversely, oropharyngeal SCC incidence followed a normal distribution, with incidence peaking in the 60- to 69-year age group at 82.88 cases per million individuals per year (Figure 2).
Incidence of Oral Cavity and Oropharyngeal SCC Patients in Canada During 1992-2010
During 1992-2010, the crude mean incidence was 31.19 cases per million individuals per year for oral cavity SCC and 23.81 cases per million individuals per year for oropharyngeal SCC. Oropharyngeal SCC incidence increased over the course of the study period, rising from 15.16 cases per million in 1992 to 34.85 cases per million in 2010. On the contrary, oral cavity SCC incidence remained relatively stable over the same study period, from 33.84 to 34.99 cases per million over the study period (Figures 1 and 2).
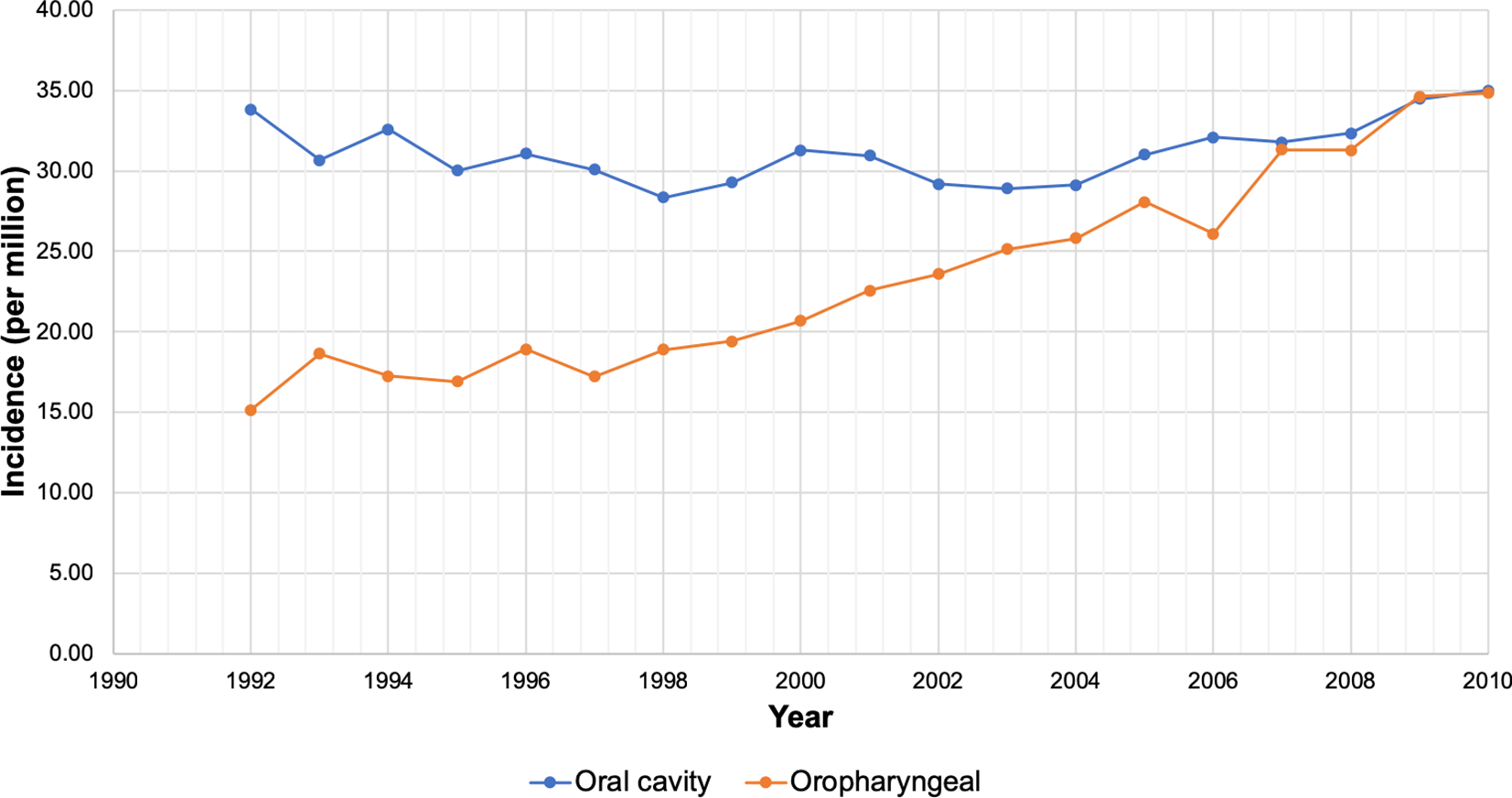
Oral cavity and oropharyngeal squamous cell carcinoma incidence per million between 1992 and 2010.
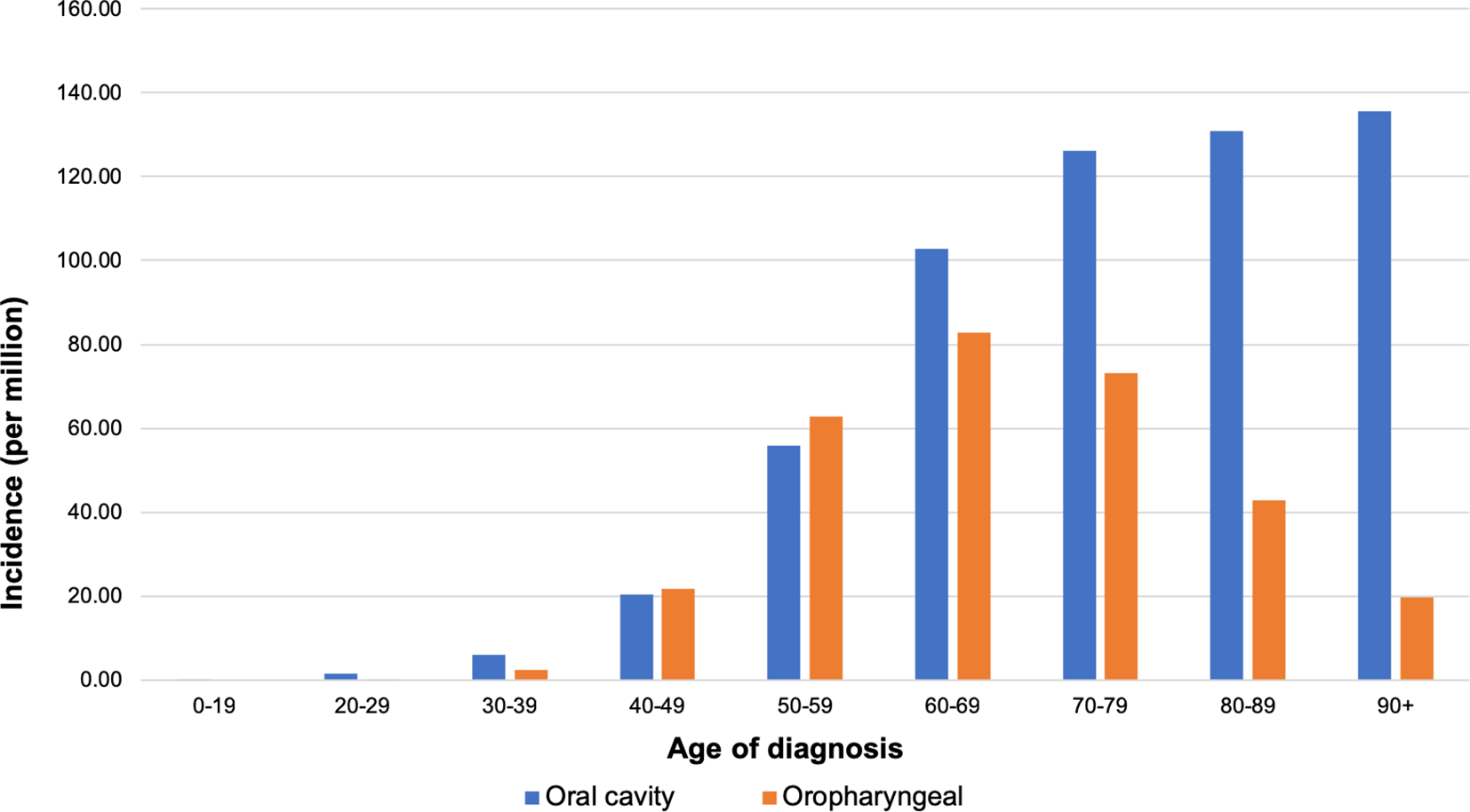
Incidence of oral cavity and oropharyngeal squamous cell carcinoma by age of diagnosis between 1992 and 2010.
Analysis by sex showed a considerably higher proportion of cases diagnosed in males compared to females, with a sex-standardized rate ratio of 1.69:1 (male:female) for oral cavity and 3.26:1 for oropharyngeal SCC (incidence per million per year).
Geographic Distribution of SCC Cases in Canada by Province
The incidence rates analysis for Canadian provinces revealed notable trends. Nova Scotia (NS), Prince Edward Island (PE), British Columbia (BC), and Manitoba (MB) had significantly higher number of oral cavity SCC cases than the national average. On the other hand, Newfoundland and Labrador (NL), Alberta (AB), and QC had incidence rates significantly lower than the national average. As for the oropharyngeal SCC, New Brunswick (NB), BC, QC, and NS had significantly higher incidences than the national average, while Saskatchewan (SK), AB, Nunavut (NU), Ontario (ON), Northwest Territories (NT), and NL had lower rates (Table 1). Crude values for SCC incidences were then adjusted for age for every province. Indirect standardization was performed using Canada’s 1992-2010 average population structure as a standard (Table 1).
Oral Cavity and Oropharyngeal Squamous Cell Carcinoma Crude Incidence Rates by Province.
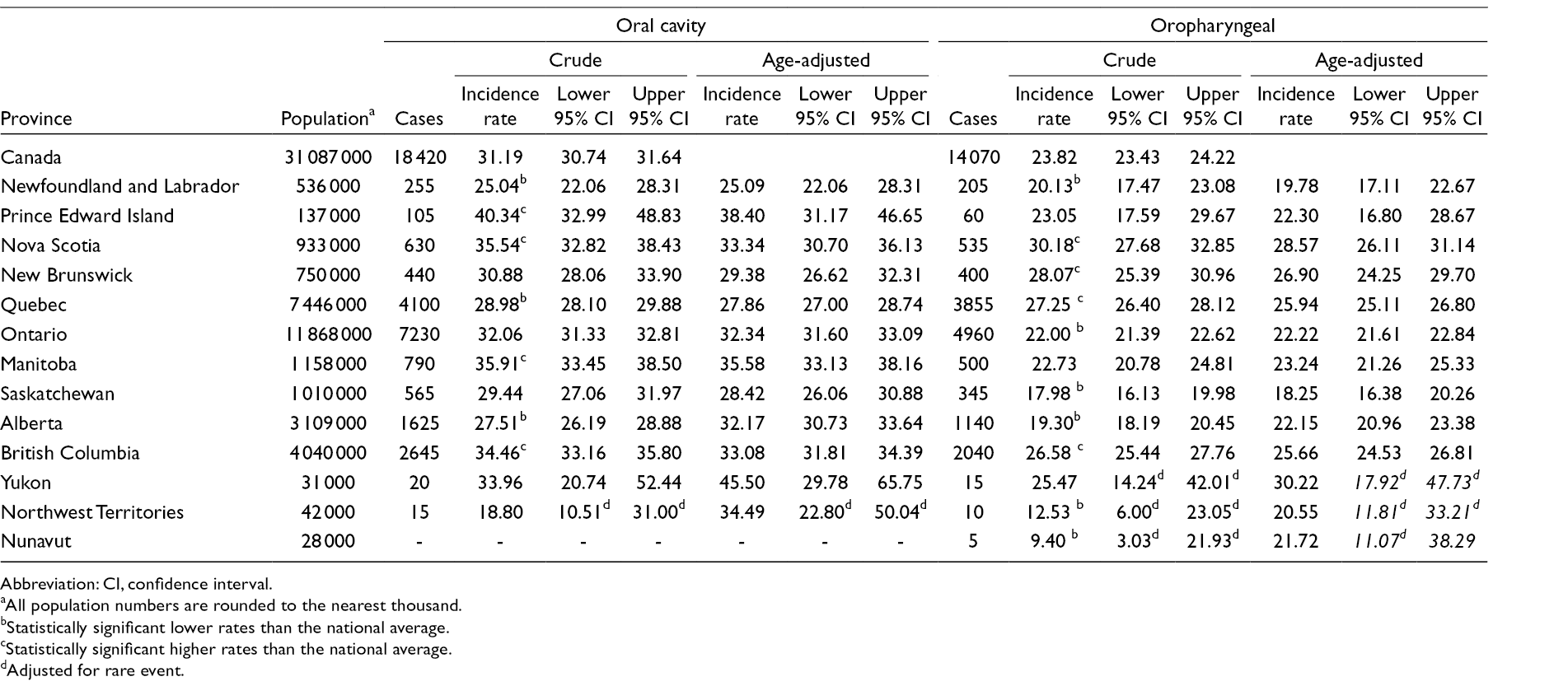
Abbreviation: CI, confidence interval.
aAll population numbers are rounded to the nearest thousand.
bStatistically significant lower rates than the national average.
cStatistically significant higher rates than the national average.
dAdjusted for rare event.
Geographic Distribution of SCC Cases by City Across Canada
For oral cavity SCC, most high incidence cities were located in BC, a high incidence province (Supplemental Table S3). Ontario’s oral cavity SCC incidence rate was similar to the Canadian average, likely owing to the fact that it houses a balance of both high and low incidence cities. Other provinces containing high oral cavity incidence cities included NB (Saint John) and MB (Winnipeg).
For oropharyngeal SCC, once again, most high incidence cities were in BC, a high incidence province (Supplemental Table S4). Other high incidence cities were found in QC (Granby), ON (Sault Ste. Marie, Thunder Bay), NB (Moncton, Saint John), and NS (Cape Breton).
Geographic Distribution of SCC Cases by FSA Across Canada
The highest crude incidence rate for oral cavity SCC was 95.69 cases per million, in T2G and E2L, located in Calgary, AB, and Saint John, NB, respectively. The lowest crude incidence rate for oral cavity SCC was 7.97 cases per million individuals per year, in L6P, Brampton, ON.
The highest crude incidence rate for oropharyngeal SCC was 119.62 cases per million, in T2G, Calgary, AB, which was also a high incidence oral cavity SCC FSA. The lowest crude incidence rate for oropharyngeal SCC was 4.54 cases per million, in E0B, Bathurst, NB. (Complete FSA results are presented in Supplemental Tables S5, S6 and Supplemental Figures S1 and S2.)
Mortality Analyses From Malignancies Arising in Oral Cavity and Oropharynx
The national mortality rates for OCC and OPC between 1992 and 2010 were 13.35 and 5.84 deaths per million individuals per year, respectively. Of note, since ICD-9 and ICD-10 codes do not differentiate between the morphologies of cancers, the incidence rates at the specified sites are not limited to SCC. The increase in oral cavity SCC incidence rates with age was reflected in the corresponding increase in mortality rates. Oropharyngeal cancers demonstrated the steepest increase in mortality rate for the 60- to 69-year-old age group. Although mortality rates fluctuated mildly over time, the general trend was a decrease in oral cavity malignancy-associated deaths (from 14.10 to 13.67 deaths per million) and an increase in oropharynx malignancy-associated deaths (from 5.46 to 6.91 deaths per million) (Supplemental Figures S3 and S4).
Crude OCC mortality rates did not reveal any provinces with significantly higher rates. However, when rates were adjusted for sex, NL, AB, NB, SK, MB, NS, BC, ON, and QC became significantly high. With age standardization, PE and Yukon also showed significantly higher mortality rates. This result further corroborated our incidence finding. Provinces/territories with significantly low oral cavity mortality rates included AB, NL, NT, and NU. This finding remains unchanged when adjusted for age, but when adjusted for sex, the results were reduced to only NT having significantly low mortality rates.
The only province with significantly high OPC mortality was QC, regardless of standardization by sex or age. Oropharyngeal cancer mortality was significantly lower in PE, SK, AB, BC, NL, and NT, regardless of standardization by sex or age (Supplemental Table S7).
Most cities with a significantly high oral cavity cancer mortality rates were also cities that had high SCC incidences, and most cities with significantly low oral cavity cancer mortality rates correspondingly had low SCC incidences. Exceptions to this trend were found in Saint John, NB and St. Catharines, ON cities, where high oral cavity SCC incidences were associated with lower oral cavity cancer mortality rates. Conversely, QC, Sherbrooke, Sudbury, Drummondville, Montreal, and Saint-Jerome cities had lower oral cavity SCC incidences, but high oral cavity cancer mortality rates. It is interesting to note that many of these cities are located in the province of QC. This inverse trend was not observed with oropharyngeal carcinoma (i.e., no cities with significantly high oropharyngeal SCC incidences had significantly low oropharyngeal mortalities and vice versa) (Supplemental Tables S8 and S9).
Discussion
Oral cavity and oropharyngeal cancer incidence and prevalence vary markedly based on geographic localization. 35 This study presents the first comprehensive analysis of oral cavity and oropharyngeal SCC incidence and mortality in Canada during 1992-2010.
Combining oral cavity and oropharyngeal cancers, a total of 37 650 cases were detected in the Canadian population-based registries from 1992 to 2010, resulting in an incidence rate of 6.37 per 100 000 individuals. This value is strikingly lower than the average incidence rate of 11.2 per 100 000 in the United States, reported by the Surveillance, Epidemiology, and End Results database over the same time period. 36 However, such a significant difference may be expected—at least in part—considering that based on the 2010 study, the United States had more current smokers than Canada (39.4%, 25.9%). 37 In fact, the United States had ~1.52 times more than in Canada of current smokers (based on the 2010 study), which reasonably correlated with 1.76 times higher rate of combined oral and oropharyngeal cancers.
Studies from population-based registries in the United States have shown an increase in oropharyngeal cancers from 1997 to 2012, 7,38 consistent with the increase in oropharyngeal cancers detected in our Canadian population. Hence, while absolute values may differ between the United States and Canada, the trends over time were similar. Such epidemiologic trends have also been observed in numerous other developed nations such as Portugal, the Netherlands, Korea, and Australia. 1 Oral cavity SCC incidence in Canada has stabilized, which differed slightly from the decline that was seen in the United States in recent years. 38
A distinct difference in incidence was noted based on the age of diagnosis for oral cavity cancers compared to oropharyngeal cancers. The higher incidence of oropharyngeal cancers in younger age groups is consistent with the previous research. 7 Using sex-standardized rate ratios, our analysis shows a 1.69:1 male-to-female predominance for oral cavity and a 3.26:1 male-to-female predominance for oropharyngeal SCC, which is comparable to data in the United States showing 1.55:1 and 3.41 male-to-female ratio for oral cavity and oropharyngeal cancers, respectively. 7 These gender disparities have been attributed to both behavioral and biological differences and are reviewed in detail in Woods et al. 39
The greatest risk factors for the development of oral cavity malignancies in the Western world are the consumption of tobacco and alcohol, with synergistic effects when their use is combined. 3 -5 With the increase in public awareness of the dangers of smoking and the institution of smoke-free legislation and tobacco taxes over the past several decades, smoking rates have declined in Canada. In addition, Canada’s consumption of alcoholic beverages increased until the 1980s, when it stabilized and began to decline. 40,41 Since the occurrence of oral cavity cancer is usually observed after a latency period of 25 years, 8 the stabilization in oral cavity SCC occurrences reflects the positive impact of provincial and federal efforts to decrease smoking and alcohol consumption. 42
In the United States, states with the highest smoking rates such as West Virginia, Kentucky, and Arkansas 43,44 also have high rates of oral cavity and oropharyngeal cancers. 45 In addition, smoking rates among adults are highest in rural areas, with urban areas, small metropolitan areas, and large metropolitan areas exhibiting progressively lower rates. 46 Our study corroborates the latter findings, with the overwhelming majority of low SCC incidence cities being in metropolitan areas with population of over 100 000. Interestingly, smoking rates in ON remained below the national average from 1950 to 2011, 47 with the associated favorable oral cavity and oropharyngeal SCC incidence profile despite the longstanding dominance of the ON tobacco belt. This may point to the importance of public health measures put in place to counteract the province’s large tobacco presence.
Due to the co-existence of other risk factors, it is difficult to directly correlate smoking trends across provinces to SCC incidence. Socioeconomic inequality has been demonstrated to result in differences in head and neck cancer incidence in the United States, Europe, and Canada, with disadvantaged areas consistently exhibiting higher rates of cancer than more prosperous areas. 48,49 Rural populations are thought to be less exposed to antitobacco messages in the media and youth are more likely to have role models who are tobacco users. 50
In the last two decades, HPV has gained its position as the main causal agent for oropharyngeal carcinoma, especially in North America. 6,51 -53 Similar to how genital HPV infection is predominantly transmitted via sexual behaviors, increasing number of genital and oral sex partners is positively associated with the head and neck SCC. 54,55 While HPV contributes to a large percentage of oropharyngeal cancers, its role remains limited for oral cavity and laryngeal cancers. 51 Systematic testing of oral and oropharyngeal cancers for HPV status was not performed in the past during the period 1992-2010, and therefore, specific data are not available. However, testing of all SCCs for HPV status using the surrogate marker p16 is the current standard of care, as per the existing protocols and guidelines. 56 The observed increase in oropharyngeal SCC incidence in Canada is also mirrored by similar trends in other economically developed countries such as Japan, Australia, Denmark, the Netherlands, Slovakia, United Kingdom, United States, and Brazil. 54
Over the last decade, all provinces and territories have instituted HPV vaccination programs, 57 albeit with differences in coverage. 58 Since HPV infection usually takes more than 10 years to progress from infection to malignancy, it remains too early to examine the effects of such vaccination campaigns on oropharyngeal SCC rates. However, a much higher incidence of oropharyngeal cancer in males compared to females points to the need to further target this population with public health initiatives. Incentivization and funding of HPV vaccines in this population that may be more susceptible to such infections may help stabilize this continuous increase in oropharyngeal cancer incidence.
We acknowledge several limitations of our study. The study is based on the evaluation of retrospective data from a national cancer registry with limitations that include misclassification bias and that not all relevant risk factors may have been identified and recorded in the registry. Further, information on individual case exposure to identified risk factors such as tobacco and alcohol consumption, HPV status of the cancer, and race of patients was not available. However, the 2018 update of the ICD-O-3 included new codes for HPV-positive and HPV-negative SCC, respectively. This update in the ICD-O-3 coding will enable future epidemiological studies to more accurately evaluate the role of HPV status of the cancer and the development of SCC and identify geographical clustering of HPV+ SCC cases and to confirm causality. Further, multiple Canadian provinces have a largely multicultural population, and the variation in oral/head and neck cancer occurrences around the world highlights the importance of examining ethnic differences. Socioeconomic status has also been linked to HPV+ head and neck cancers, and thus having such information could help to better characterize risk factors for these diseases. 59 Despite these limitations, this large registry-based study allowed for the detailed characterization of important epidemiologic trends in Canada.
Finally, it is important to highlight that as Canada’s healthcare system is a single-tier (payer), which is funded and operated by the government, the data are collected with consistency, where each provincial and territorial cancer registry identifies tumors in its population by combining information from sources such as cancer clinic files, radiotherapy and hematology reports, records from inpatient hospital stays, outpatient clinics, pathology and other laboratory/autopsy reports, radiology and screening program reports, medical billing and hospital discharge administrative databases. The CCR/LRQC performs multiple rigorous processes to ensure accuracy including an internal record linkage to identify possible duplicate records. These measures allow for high rates of detection and diagnostic accuracy of incidence data recorded by the registries.
Indeed, several studies investigated the detection rates and accuracy of diagnostic data in the largest provincial branch of the CCR: the Ontario Cancer Registry (OCR) which collects data from the most populous province. In fact, a case ascertainment of ~99%, a detection rate (detecting and accurately assigning index tumor site) of 81.4% to 96%, and a confirmation rate (correctly assigning tumor site) of 90.9% were documented by several studies, 60 -62 which confirms a high quality of data and detection rates in the Ontario registry. According to the CCR, the process of data acquisition is consistent across all provincial and territorial registries and, therefore, we expect a high catchment rate and accuracy in the other registries, although this was not confirmed by studies, as in the Ontario registry.
In conclusion, this study identified and confirmed important epidemiological trends, allowing us to gain a more comprehensive understanding of oral cavity and oropharyngeal malignancies in Canada. Understanding the landscape of head and neck malignancies in Canada is crucial for informing the allocation of medical resources for the prevention, diagnosis, and management of these cancers.
Supplemental Material
Figure S1 - Supplemental material for Epidemiology and Patient Distribution of Oral Cavity and Oropharyngeal SCC in Canada
Supplemental material, Figure S1, for Epidemiology and Patient Distribution of Oral Cavity and Oropharyngeal SCC in Canada by Feras M. Ghazawi, Jessica Lu, Evgeny Savin, Andrei Zubarev, Peter Chauvin, Denis Sasseville, Anthony Zeitouni and Ivan V. Litvinov in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cole Foundation Grant, Canadian Dermatology Foundation research grants, and Fonds de recherche du Québec – Santé (FRSQ# 34753 and 36769) research grants to Dr Litvinov.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.