
Abstract
Background
Accelerators in medical gloves are a common cause of allergic contact dermatitis among healthcare workers.
Objective
A systematic review of medical and nursing literature, patch testing reports, and chemical analyses of gloves was conducted to assess accelerator contents reported in the literature and to identify accelerator-free gloves.
Methods
A systematic literature search was performed in OVID Medline and OVID EMBASE. Hand-searching of reference lists of articles in the field and author input generated the remainder of articles assessed.
Results
We present an inventory of accelerator contents of gloves and accelerator-free glove options as reported in the literature as a clinical reference tool to assist allergen-free glove selection for individuals suffering from allergic contact dermatitis due to rubber accelerators.
Limitations
Pertinent limitations of our review include lack of predefined study exclusion criteria and screening of the studies identified in the search by 1 review author only.
Conclusion
The glove inventory we provide summarizes the available literature regarding medical and surgical glove accelerator content, describing gloves both by brand and manufacturer as well as by accelerators.
Introduction
Hand dermatitis has a lifetime prevalence of 20% and commonly affects healthcare workers (HCWs), laboratory workers, cleaning personnel, food service workers, hairdressers, tradespeople, construction workers, and homemakers. Allergic contact dermatitis (ACD) is a common occupational skin disease, which affects approximately 1% to 3% of the population and is associated with considerable financial cost and negative impact on quality of life. 1 In HCWs, ACD is commonly seen in the context of hand dermatitis due to rubber accelerators used in the manufacture of medical and surgical gloves. Rubber accelerators are catalysts used in rubber vulcanization, also adding durability and strength to rubber. 2
Contact dermatitis is the most common cause of occupational skin disease, accounting for 90% to 95% of cases. 3 The hands are the most frequently affected site, seen in 80% to 90% of contact dermatitis cases. 4 Unfortunately, contact dermatitis is particularly prevalent among HCWs and is often seen in association with the use of protective medical gloves. Medical gloves are class II medical devices used to prevent the transmission of diseases both to patients from HCWs and from patients to HCWs. 5 For many HCWs, they are a daily necessity.
Allergic contact dermatitis is a type IV hypersensitivity reaction. 6 This type of hypersensitivity reaction involves a T-cell response aimed at the allergen. 7 Allergic contact dermatitis presents as a delayed reaction occurring after the skin has been sensitized to the allergen, and develops over the course of 12 to 72 hours. It differs from irritant contact dermatitis, which is related to the direct toxicity of agents to skin and can develop rapidly without prior sensitization. 7 After sensitization to the allergen, further exposures re-activate the cell-mediated immune response and can present as erythema, pruritus, vesicles, fissures, or scaling. Allergic contact dermatitis accounts for approximately 20% of occupational contact dermatitis, while irritant contact dermatitis accounts for about 80%. 4 In 1 study, up to 24% of HCWs reported glove-induced symptoms, with 10.5% testing positive for allergic contact dermatitis to rubber allergens on patch test. 8
The cost burden associated with contact dermatitis is considerable. According to the American Academy of Dermatology, the total medical costs associated with contact dermatitis were estimated in 2017 to be over $1.5 billion USD and lost productivity was estimated to cost $699 million USD. 9 Aside from the monetary costs associated with contact dermatitis, the burden of the disease on affected individuals may also be considerable. The modified Skindex-16 quality of life assessment tool has been used to study the impact of ACD on patients. 10 The 4 scales in the assessment include emotions, symptoms, functioning, and occupational impact. Allergic contact dermatitis was found to have the greatest impact on the emotions scale, with individuals feeling frustrated and annoyed by their condition. In terms of symptoms, individuals with ACD reported being bothered most by itching, skin irritation, and disease persistence or recurrence. People with hand dermatitis had significantly worse scores on the occupational impact scale. In terms of functioning, individuals reported that it was significantly harder to work or do what they enjoy. 10
Functional limitation is understandable in those with occupational hand ACD given the common clinical presentation as an eczematous eruption of erythematous papules or plaques, which may have secondary lichenification, fissures, and scaling. Glove-related ACD is often sharply demarcated at the wrists and confined to the area of exposure.
In glove-related contact dermatitis, rubber accelerators are the main culprits. 11 Natural rubber latex does not cause ACD, however latex-based gloves may contain rubber accelerators. It is important to note that the rubber accelerants, not the latex base, cause ACD. The most common causative agents include thiurams, carbamates, and mercaptobenzothiazoles. 12 Other causes of glove-related ACD include antioxidants, such as black rubber mix chemicals, which prevent degradation of glove material. 11 Thiurams and carbamates are often found together in gloves as these 2 types of organic compounds form a redox pair. Allergic contact dermatitis to carbamates has increased in recent years as thiurams were replaced with carbamates in rubber vulcanization, 2 a process used to improve rubber elasticity and strength. Benzothiazoles, such as mercaptobenzothiazole, are heterocyclic aromatic compounds and are a common cause of hand or foot dermatitis. 2 Another accelerator implicated in glove ACD is diphenylguanidine, an organic compound with similar molecular structure to dithiocarbamates. Structural similarity has led to diphenylguanidine being included in the testing reagent for dithiocarbamate ACD in carba mix. Thus, positive patch test reactions to carba mix may have led to underdiagnosis of true diphenylguanidine ACD. 2 Dithiodimorpholine (DTDM) is another vulcanizing agent and is used in rubber tire, inner tube, footwear, and glove production. The majority of DTDM ACD cases are secondary to hand dermatitis. Since DTDM is not found on commonly used patch testing series, ACD to this allergen is likely underdiagnosed and it could be the culprit allergen in cases of hand dermatitis where other tested allergens were negative. 13
Studies have shown trends of decreasing thiuram and mercaptobenzothiazole ACD, while the incidence of reactions caused by carba mix (including 1,3-diphenylguanidine [DPG], zinc dibutyldithiocarbamate [ZDBC], and zinc diethyldithiocarbamate [ZDEC]) has significantly increased. 14 Changing trends may be related to developments in glove manufacturing, including movement toward powder-free gloves. The accelerator content in powder-free gloves is significantly lower than in powdered gloves. 12
The identification of the specific causative allergens is very difficult without patch testing. In their study, Siegel et al found that only 51% of subjects were able to correctly identify the gloves responsible for their ACD. The ability of individuals to identify the specific gloves responsible for eliciting their ACD may be complicated by the number of different glove brands used and the severity of the reaction. Furthermore, as ACD is a delayed reaction, it may be difficult for people to associate their symptoms with exposures to particular gloves. 12
Allergen avoidance, following identification via patch testing, is the mainstay of ACD treatment and prevention. Identifying gloves that are free of particular accelerators can be challenging because accelerator contents can differ within a single manufacturer. Moreover, glove brands named similarly can have different accelerator contents. As well, there are no reporting requirements regarding rubber accelerators present in a given glove brand. This can make glove decisions difficult even for individuals with an identified accelerator ACD. 15 In an effort to facilitate the appropriate selection of medical and surgical gloves for individuals suffering from accelerator ACD, we performed a systematic review and created an inventory of gloves described as accelerator-free as well as accelerator contents of gloves reported in the literature.
Materials and Methods
Data Source
A systematic literature search in OVID Medline and OVID EMBASE was conducted from database inception to August 2018. We included studies that identified the rubber accelerator content in medical and/or surgical gloves, that described the methodology used to identify the accelerator content, and that were written in the English language. Further exclusion criteria, defined after the search stage, include glove brands with discrepancies between references regarding the accelerator contents and glove brands with more than 1 manufacturer. The database literature search did not undergo additional updates after August 2018. The terms searched in OVID Medline were “gloves, protective/ OR (protective gloves OR medical gloves OR examination gloves OR surgical gloves).kf,tw AND (hypersensitivity/ OR hypersensitivity, delayed/ OR hypersensitivity, immediate/ OR latex hypersensitivity/ OR dermatitis, allergic contact/ OR (contact dermatitis or allerg*).kf.tw”
The terms searched in OVID EMBASE were
“protective glove/ OR (protective gloves OR medical gloves OR examination gloves OR surgical gloves).kw.tw AND hypersensitivity/ OR allergic reaction/ OR delayed hypersensitivity/ OR occupational allergy/ OR skin allergy/ OR tissue reaction/ OR latex allergy/ OR (contact dermatitis or allerg*).kw.tw”
These search results were transferred to EndNote X8 software (Clarivate Analytics, Philadelphia, United States) for data management. Additional studies were identified through a manual search of reference lists of articles in the field and through suggestion by authors of this review.
Results are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 16 We did not register a protocol for this systematic review.
Study Selection
After search results were generated, all references were deduplicated using EndNote X8 data management software. Full text access was obtained through University of Calgary Libraries online access, Pubmed free full text access, and Google Scholar free full text access. Reference titles and abstracts were screened for relevancy to the topic of “glove allergic contact dermatitis” and “rubber accelerators” by one of the authors (KL). Remaining references were read in full by one of the authors to identify those that reported testing accelerator contents of glove brands (KL).
To improve the accuracy of the screening and inventory compilation, all references were screened twice by the first author (KL). Intra-observer reliability was not statistically assessed during this study. The other authors of this review identified further studies for assessment.
Quality and Validity
Study quality (risk of bias) and validity were not formally assessed. In order to be included in qualitative synthesis, studies were required to describe a methodology for identifying the accelerator content. Since the aim of this study is to delineate glove purchasing decisions for HCWs with rubber accelerator ACD, other types of gloves including industrial, chemical, and household glove brands were excluded for the lack of external validity. Exclusion criteria were determined at the search result stage because of aspects we did not anticipate when designing our search strategy.
Information Synthesis
Information was synthesized through the creation of a glove inventory categorizing gloves by glove brand and manufacturer and reported accelerator contents per article description. In cases of discrepancies between references regarding the accelerator contents of the same glove brand, the brand was excluded because of ambiguity and this is further elaborated in the discussion section. In cases where more than 1 glove manufacturer was attributed to the same glove brand, the glove brand was likewise excluded from the study. Glove manufacturers were not contacted. Meta-analysis was not deemed suitable for the data we had identified.
Results
Search Results
Our search of OVID Medline yielded 1218 hits, while the OVID EMBASE search yielded 419 hits. Another 200 potentially relevant articles were identified through other sources. Excluding duplicates, 1613 potentially eligible references were screened for relevancy to the topic of allergic contact dermatitis and information regarding glove accelerators. After screening, 1454 references were excluded due to lack of relevancy to the intended topic. After title and abstract screening, 159 full text articles were assessed for eligibility and 9 references were included in qualitative synthesis. 1,11,15,17 -22 A PRISMA diagram outlining our study selection is given in Figure 1.
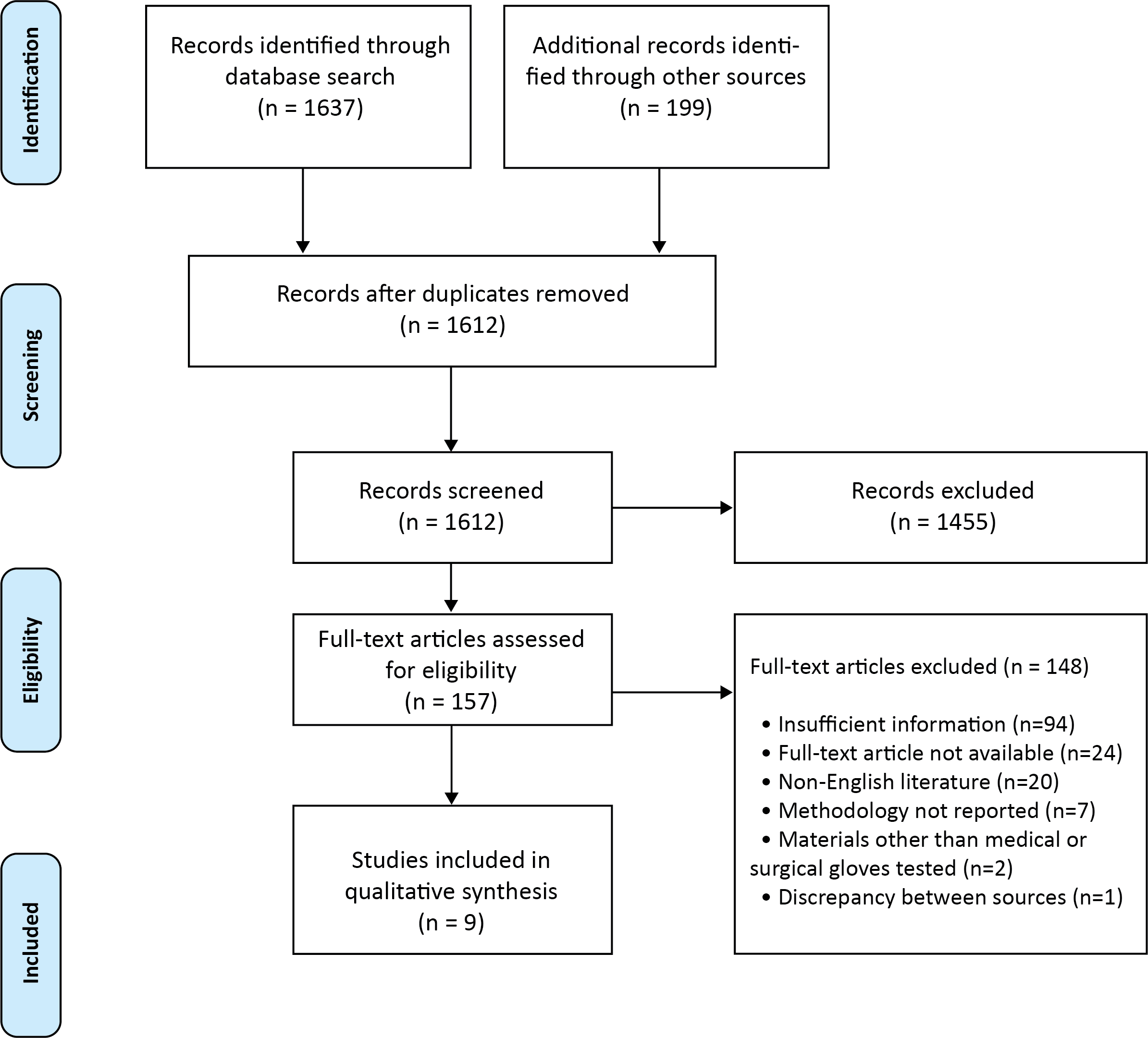
Study selection.
The most common reason for exclusion was articles that did not test for accelerators or had insufficient glove manufacturer and brand information (n = 94). 8,12,13,23 -113 In cases where full text articles were not available, these studies were excluded (n = 24). 114 -137 All non-English language literature was excluded from qualitative synthesis (n = 20). 138 -157 Articles that reported accelerator contents without providing a methodology to support their claims were also excluded from qualitative synthesis (n = 7). 2,158 -163 It has been decided to exclude articles that did not provide a description of the methodology for the determination of glove accelerator contents to ensure that the references provided in the glove inventory employed adequate methods. Studies that tested accelerator contents in materials other than medical and surgical gloves were excluded (n = 2) 164,165 as were studies with results that showed discrepancy compared to multiple other sources (n = 1). 166 A detailed list of excluded studies with the reasons for exclusion is provided in Supplemental Table 3.
The 9 1,11,15,17 -22 included articles were used to create the glove inventory presented in Table 1. In addition to this inventory of gloves containing the fewest number of accelerators, we provide a full inventory of all gloves included in our review as reported in the literature in Supplemental Table 2.
Inventory of Glove Brands with Minimal Accelerator Content.
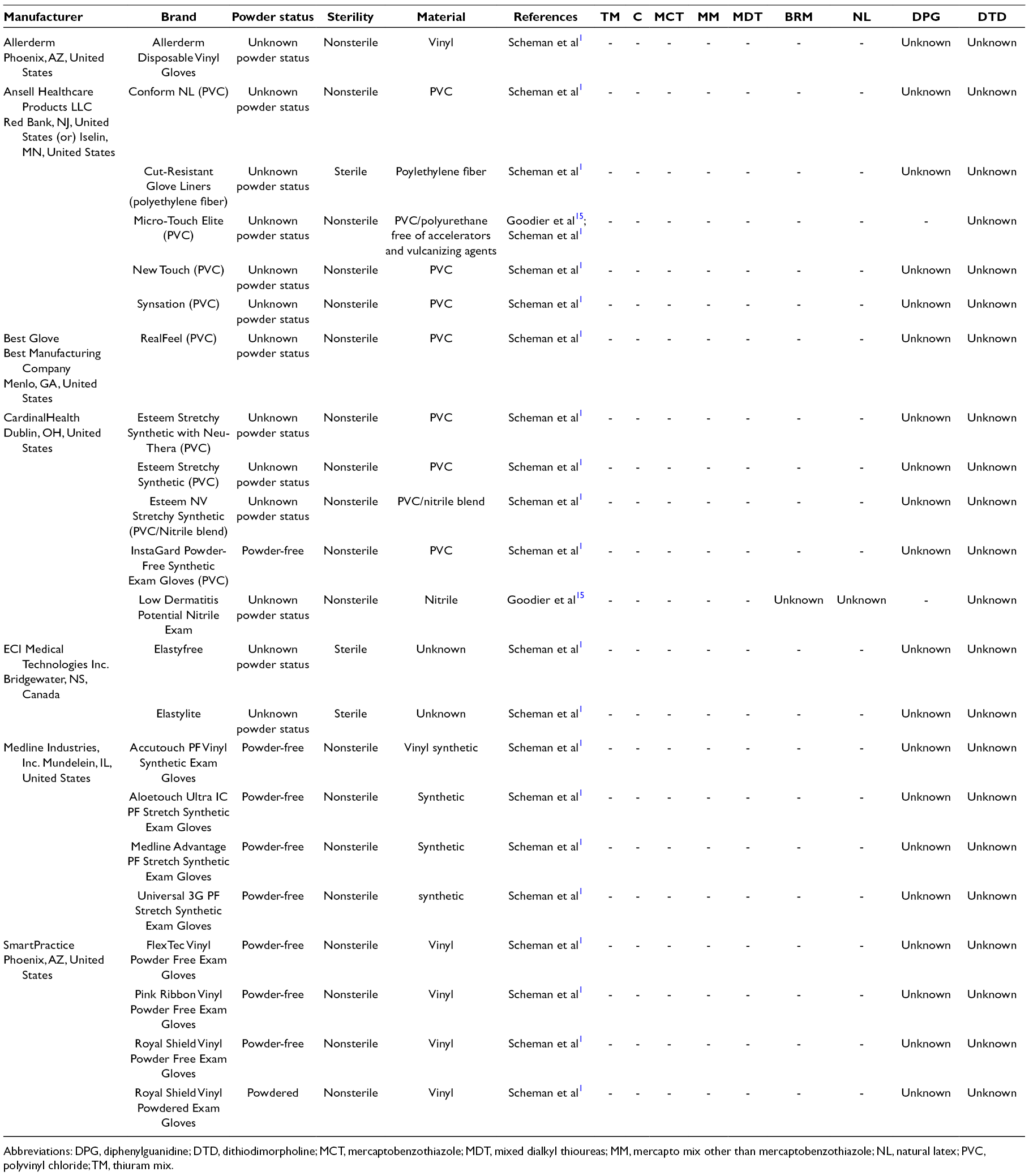
Abbreviations: DPG, diphenylguanidine; DTD, dithiodimorpholine; MCT, mercaptobenzothiazole; MDT, mixed dialkyl thioureas; MM, mercapto mix other than mercaptobenzothiazole; NL, natural latex; PVC, polyvinyl chloride; TM, thiuram mix.
Included studies differed in the methodology used to test accelerators and in the accelerators tested by each study. References included in qualitative synthesis employed various methodologies such as UV or mass spectrometry and high performance liquid chromatography (HPLC) analyses, 11,17,19 or accelerator analysis reports from glove manufacturers. 15,20 A detailed list of included studies with the study methodology is provided in Table 2. Contact information for glove manufacturers as listed in the reviewed literature is provided in Supplemental Table 3 to facilitate glove acquisition.
List of Included Studies, Year of Publication, Country of Study, and Methodology.
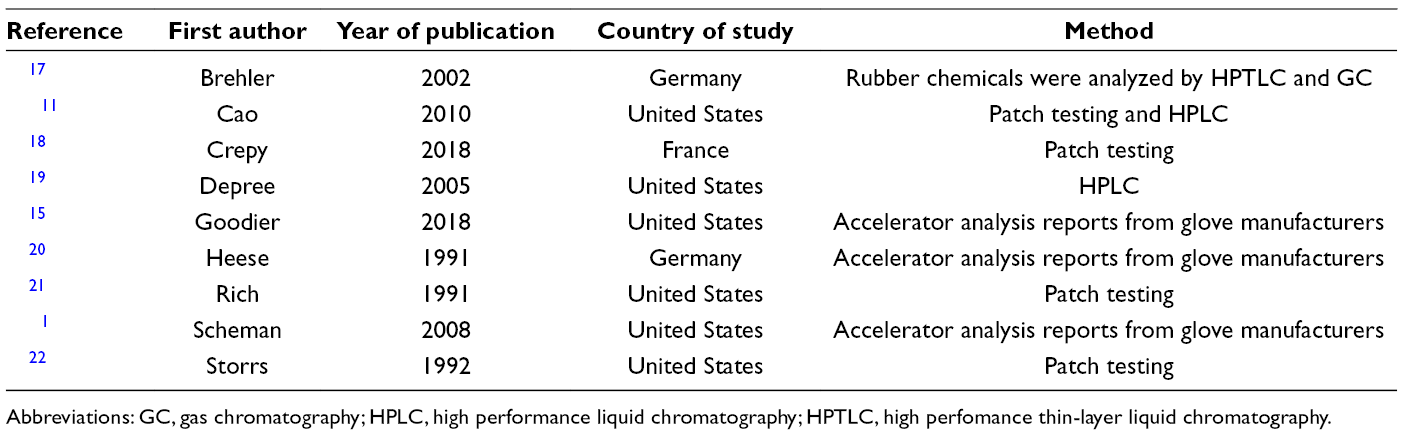
Abbreviations: GC, gas chromatography; HPLC, high performance liquid chromatography; HPTLC, high perfomance thin-layer liquid chromatography.
Discussion
The selection of appropriate gloves for the management of ACD, in terms of both function and accelerator contents, can be challenging for healthcare providers. Different materials, manufacturers, and brands of medical gloves demonstrate a wide range of accelerator contents. Medical gloves are available in various materials such as latex, nitrile, polyvinyl chloride (PVC), neoprene, as well as other less common elastomer materials such as polyisoprene, sensoprene, or polychloroprene. These materials have distinct functional differences and characteristic accelerator content profiles. For example, most nitrile gloves reported in the literature contain carbamates. 1,15 Other authors suggest that PVC gloves are the only gloves consistently free of all rubber accelerators. 20 However, our inventory provides evidence that other materials can be used to make accelerator-free gloves including nitrile and neoprene. 1,15 Our inventory displays accelerator contents of gloves reported in the literature to facilitate glove choice for individuals who are sensitive to one or more accelerators but do not require their gloves to be free of all accelerators (Table 1; Supplemental Table 2). 1,11,15,17 -22
While compiling this glove inventory, it was interesting to note that studies showed vast differences in the accelerators tested. For example, thiurams, 1,11,15,17,18,21,22 carbamates, 1,11,15,17,19 -22 and mercaptobenzothiazoles 1,11,15,17,19 -22 were tested by most studies; whereas thioureas, 1,11,15,20 diphenylguanidine, 11,15,18 and dithiodimorpholine 11 were less often tested. Another aspect of accelerator reporting that was heterogeneous between studies is the amount of manufacturer information provided. Some studies did not provide the manufacturer of the glove brands and were therefore excluded from qualitative synthesis for lack of reported detail. In other cases, references provided inconsistent information in regard to glove manufacturer contact information.
The articles included in qualitative synthesis were limited to English language literature. As well, references were required to describe glove brands by their accelerator content, list the corresponding manufacturer, and provide some description of how the accelerator content was assessed. The requirement for such a methodological description may have limited the number of included studies in our review because references that did not describe their methodology may still have reported glove accelerator content correctly. However, without described methods, it is unclear whether the reported glove accelerator contents are reliable.
To our knowledge, this review and glove inventory provides the most comprehensive and current list of glove options for those with rubber accelerator-induced ACD. We have included all rubber accelerators reported in the references used in the glove inventory to provide detailed information for glove purchasing decisions. We also have included other patch test allergens including latex and black rubber mix which are less commonly associated with glove-related ACD but are common medical and surgical glove components. Our glove inventory is limited by the amount of detail provided in the included studies, and because not all common rubber accelerators are reported by each study, our glove inventory is unable to display all accelerators for each glove brand. However, it provides what we believe is the best summary of the available literature at present. There are 389 glove brands outlined in our inventory, representing glove ACD literature published as early as 1991.
This review is subject to a number of limitations. First, our workflow deviated from the standard methodology for a systematic review in that only 1 author screened the potentially eligible studies and we did not register a protocol for this systematic review. Second, we did not have predefined study exclusion criteria. Furthermore, some readers may view the lack of prior registration of our review as a limitation. Moreover, most of the information on gloves included in this inventory were provided by 2 main sources 1,15 ; therefore, errors in methodology or data of the sources could impact the overall accuracy of this review. Finally, some of the studies included in our glove inventory were published many years prior to our review, with the oldest references published in 1991. 20,21 This could mean that the glove brands described by these sources are no longer available for ordering or that the accelerator contents of some glove brands have changed since the time that the study in question was published.
Finally, when compiling this review, we identified examples of gloves where 2 manufacturers appear to produce gloves of the same or a similar brand name although the accelerator contents may differ. It is unclear why different glove manufacturers may share a glove brand name as we did not contact these glove manufacturers. For example, “TriFlex” and “Triflex” glove brands are marketed by Baxter Pharmaseal 21 and CardinalHealth, 15,20 respectively, and differ in both glove material and accelerator content. As well, in the case of “Triflex,” Heese et al 20 report this brand as PVC accelerator-free gloves, whereas Goodier et al 15 report this brand as latex gloves containing carbamates. These 2 examples of discrepancies between seemingly identical products could cause danger to consumers who order this glove brand without knowing about the inconsistency in the literature. This risk for ordering error is the main reason that glove brands with discrepancies in accelerator content or material were excluded from our glove inventory. On the one hand, the complexity of glove options gives consumers more choice based on function and sensitivity to accelerators. However, on the other hand, the intricacies of glove brands and accelerator contents can lead to inadvertent exposure to accelerator allergens if users are not able to obtain the necessary information for safe glove purchasing decisions.
Conclusion
Glove-induced allergic contact dermatitis is a common occupational disease often caused by rubber accelerators. The selection of gloves free of offending agents can be difficult due to the wide variety of accelerators used in glove materials, challenges in obtaining accelerator content from manufacturers, and changes in brand accelerator contents over time. To our knowledge, our review represents the most comprehensive and current inventory in the literature. With our inventory of glove accelerator contents and accelerator-free glove options, we hope to facilitate safer and smarter glove purchasing decisions for those who have delayed-type hypersensitivity to rubber accelerators. While we attempted to be accurate and complete in our description of glove accelerator content, we cannot guarantee the accuracy and completeness of the data presented. Readers should do their own due diligence and verify the information on glove accelerator content before making clinical or glove purchasing decisions.
Supplemental Material
Supplemental material - Supplemental material for Making Glove Decision Less of a White Knuckling Experience: A Systematic Review and Inventory of Glove Accelerator Contents
Supplemental material, Supplementary material, for Making Glove Decision Less of a White Knuckling Experience: A Systematic Review and Inventory of Glove Accelerator Contents by Kaitlyn M. Lopushinsky, Navjeet Gill, Whitney K. Shea, John F. Elliott, Sebastian Straube and Marlene T. Dytoc in Journal of Cutaneous Medicine and Surgery
Footnotes
Authors’ Note
The authors Navjeet Gill and Whitney K. Shea share second authorship.
The authors Sebastian Straube and Marlene T. Dytoc share senior authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.