
Abstract
Objectives
We aimed to assess the perception of psychodermatology, practice patterns, and challenges reported by Canadian dermatologists.
Methods
We designed an online questionnaire based on previous literature, including questions about practitioners’ perceptions, practice patterns, training, and challenges in psychodermatology. We solicited their opinions on desired training, research needs, and clinical approach recommendations. Our survey was distributed nationally by the Canadian Dermatology Association (CDA).
Results
Of the total of 78 participating dermatologists, >75% reported treating patients with psychodermatological conditions, with higher frequencies of secondary than primary psychodermatological conditions. While practitioners had some confidence in their understanding of psychodermatology (median = 4 on a 5-point scale), their comfort levels to approach these patients were lower (median = 3), and their confidence in prescribing psychotropic medication was markedly low (median = 2). A total of 50% reported that a “multidisciplinary approach” would be best for these patients. Poor access to psychiatry was the most reported (26.9%) challenge, together with time constraints, lack of training, poor communication with patients, and lack of patient insight and resources. While 46.2% reported having never participated in psychodermatology training, 55.1% expressed interest in doing so.
Conclusion
We identified several challenges with knowledge, awareness, and healthcare delivery in psychodermatological practice in Canada. Increasing dermatologists’ access to psychiatric consultations/services, a multidisciplinary approach with dermatologists and psychiatrists co-providing care, and more specialized training in this area are recommended to narrow the identified gaps.
Introduction
Psychodermatology focuses on mind-skin interactions and the disorders that result from their disturbance. These conditions are common in dermatological practice. It is estimated that every third patient in a dermatology clinic needs assessment for mental health symptoms. 1 -3 In addition, compared with the general population, patients with skin diseases have a higher prevalence of comorbid psychiatric disorders. 4 Patients with psychiatric diagnoses are also more likely to be affected by skin conditions. Currently, there is no universal consensus on the clinical categorization of these conditions, but they are often grouped into 4 broader categories: (1) primary psychodermatological disorders, (2) secondary psychodermatological disorders, (3) psychophysiological disorders, and (4) psychogenic pruritus. 5 Alternative classifications categorize conditions based on their assumed psychiatric etiology and pathophysiology (ie, psychocutaneous conditions due to psychotic, depressive, anxiety-related, or obsessive-compulsive symptoms). 5 The estimated high frequency of these diseases, combined with a lack of consensus on classification and clinical approach, highlights the clinical reality of concurrent mental health and dermatological conditions. This suggests the importance of establishing well-informed psychodermatology practice in medicine.
Healthcare delivery in psychodermatology can be difficult and unsatisfying for practitioners, as well as patients and their families. Despite the presence of an overarching psychiatric pathology in most psychodermatologic conditions, these patients tend to present more readily and in earlier phase to dermatologists, not psychiatrists. 4,6 Several studies reported challenges that limit providing optimal care to patients with psychodermatological conditions in dermatology practice. These include physicians’ under-recognition of psychodermatological disorders, patients’ poor insight into these conditions, and lack of specialized clinics to treat these disorders. 6,7 In addition, dermatologists’ lack of confidence and/or training to initiate psychotropic therapy can be a barrier to successfully treating psychodermatology patients. A US-based survey of dermatologists found that only 3% of respondents reported they had confidence in prescribing these medications. 8 Understanding pharmacological prescription practice in dermatology will help identify and address potential gaps and, consequently, improve the quality of care for patients with psychodermatological conditions. In Canada, psychodermatology services are limited. Furthermore, the epidemiological characteristics, clinical experiences, and challenges in psychodermatology in Canada have not been systematically reviewed. 9 In addition, no previous relevant study from other geographical locations 7,10,11 differentiated between primary and secondary psychodermatological conditions. However, the latter have significantly different clinical implications and should be separated, as the course of treatment of these conditions differs as well. Hence, the overall lack of knowledge of the challenges and the current status of psychodermatology treatment in Canada may hinder improving the quality of care. In the current study, we aimed to assess the perception of psychodermatology, practice patterns, and challenges reported by Canadian dermatologists in an attempt to highlight important aspects, bridge gaps in knowledge, and detect potential shortfalls that should be addressed.
Methods
Survey
We developed a questionnaire based on a literature review of articles addressing psychodermatology. 7,8,10 -12 We included questions to assess practitioners’ subjective knowledge of psychodermatology, relevant practice patterns, and perceived challenges, as well as past and desired training and education, attitudes toward research, and future recommendations. In addition to previous studies in this area, we asked questions about psychotropic medication prescription patterns and differentiated primary from secondary psychodermatological conditions. Questions on demographic and other background characteristics of the participants were also included.
In order to explain primary and secondary psychodermatological conditions, at the beginning of the survey, we introduced primary psychodermatological conditions as “conditions in which the patient has no primary skin disease and all of the cutaneous findings are self-induced (eg, delusions of parasitosis, excoriation disorder, trichotillomania).” Secondary psychodermatological conditions were described as “conditions that involve the development of psychological problems as the results of a skin disease or the exacerbation of a skin disease due to psychological factors (eg, anxiety and depression in patients with psoriasis or atopic dermatitis).”
Answer formats included yes/no, 5-point Likert-scales, multiple choice, and free text, for a total of 29 questions. The survey was administered through Google Forms, and participants could choose to fill out an English or a French version.
Data Collection
Our online survey was distributed nationally by the Canadian Dermatology Association (CDA) in October 2019. All CDA members (approximately 700 dermatologists and dermatology residents in Canada) were contacted through email with 1 reminder sent 4 weeks after initial contact. A consent form was included in the information sheet at the beginning of the survey. The study was approved by the University of Alberta Research Ethics Board (Pro00092486).
Statistical Analysis
Survey data were saved automatically in Google sheets. After cleaning typographical errors, repeated entries, and partial survey responses, all data were imported into the Statistical Package for the Social Sciences version 26.0 (IBM SPSS Statistics for Windows, version 26.0; IBM Corp., Armonk, NY, USA) for further analysis. Descriptive statistics included frequency counts and percentages out of the total number of participants who answered the corresponding question, as well as medians and ranges for the Likert scales.
Results
Participants
Overall, a total of 78 dermatologists and dermatology residents filled-out our survey, amounting to an approximate response rate of 11.1% (out of 700). As detailed in Table 1, the majority of participants were female, practicing in private-solo practice in urban areas.
Participants’ Characteristics and Frequency of Psychodermatology (PD) Cases.
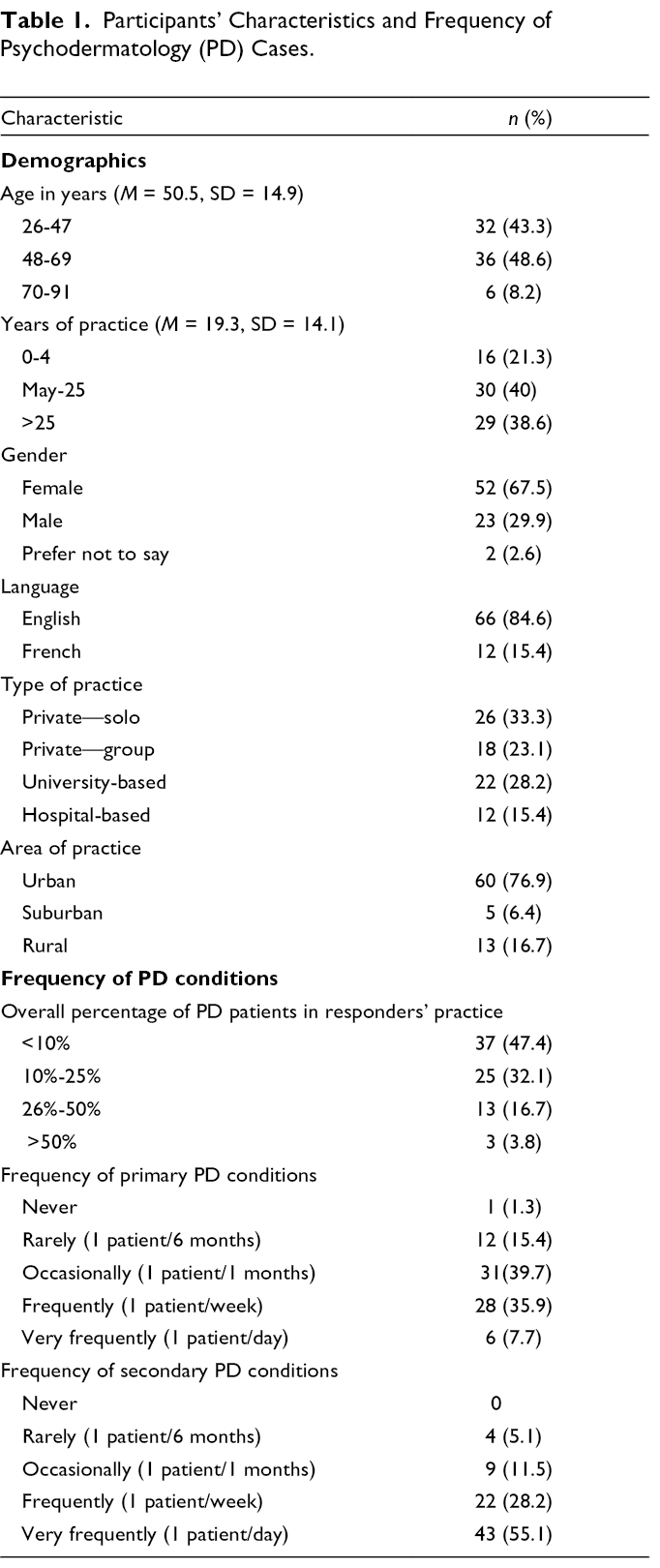
Psychodermatology-Perceived Frequencies
Table 1 details the perceived frequencies of psychodermatological conditions in the practices of our responders. The largest proportion of participants (47.4%) reported that psychodermatological conditions consist of less than 10% of their practice, but almost one-third (32.1%) reported psychodermatological conditions to make up between 10% and 25% of their patients. Of the total of 78 participating dermatologists, >75% reported treating patients with psychodermatological conditions, with higher frequencies of secondary than primary psychodermatological conditions. For primary psychodermatological conditions, we had similar percentages of physicians who see 1 patient/month and 1 patient/week (39.7% and 35.9%, respectively), while for secondary psychodermatological conditions 83.3% of physicians reported seeing a minimum of 1 patient per week (55.1%, 1 patient/day and 28.2%, 1 patient/week).
Psychodermatology Practice
Figure 1 summarizes responses related to practitioners’ perceived understanding of psychodermatology and comfort levels with psychodermatological patients. The respondents had some confidence in their understanding of psychodermatology (median = 4 on a 5-point scale). However, their comfort-levels to approach these patients were lower (median = 3 L range = 4). Less than half of the participants (44.9%) reported having a comfort level >3 on a 1-5 Likert scale.
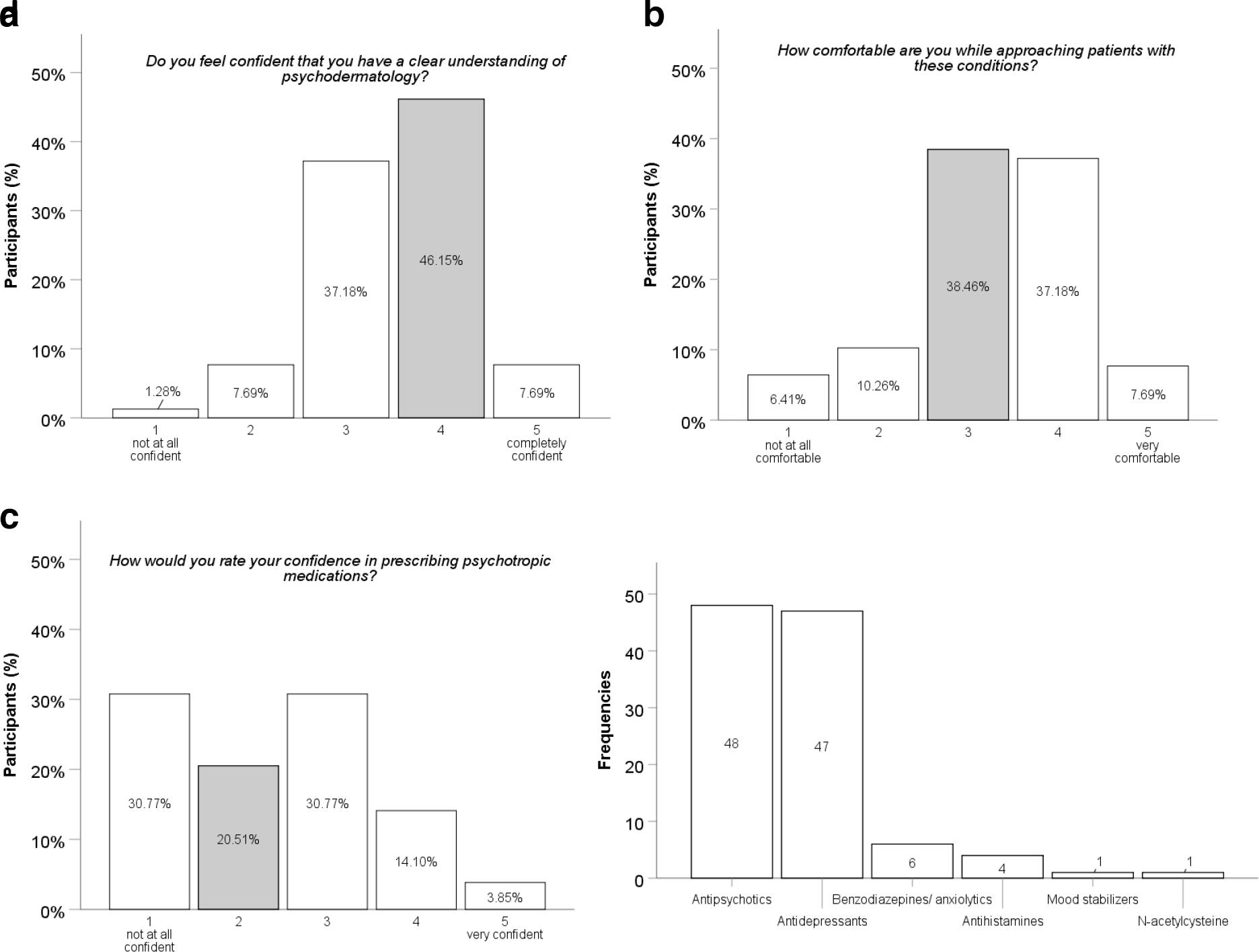
Participants’ responses. (
Regarding practice patterns (Table 2), a minority of participants (6.4%) reported managing primary psychodermatological conditions themselves, while 23.1% reported doing so for secondary psychodermatological conditions. About one-third (32.1%) of dermatologists who manage patients themselves have never been prescribed a psychotropic medication. Of the practitioners who reported having prescribed psychotropic medications, 45% reported prescribing psychotropic medications on an “occasional basis,” while 35% reported using them only for severe cases (Table 2). The vast majority of the participants (82.1%) reported their confidence in prescribing psychiatric drugs to be ≤3 on a 1-5 Likert scale (median = 2; range = 4). Most commonly prescribed psychotropic medication classes included antipsychotics, antidepressants, and benzodiazepines (Figure 1D) with risperidone as the most frequently reported drug, followed by the antidepressants doxepin and amitriptyline, as well as the antipsychotic pimozide. When asked about the best approach to psychodermatology, a “multidisciplinary approach” was endorsed by the largest proportion of responders (50%).
Practice Patterns in Psychodermatology (PD).
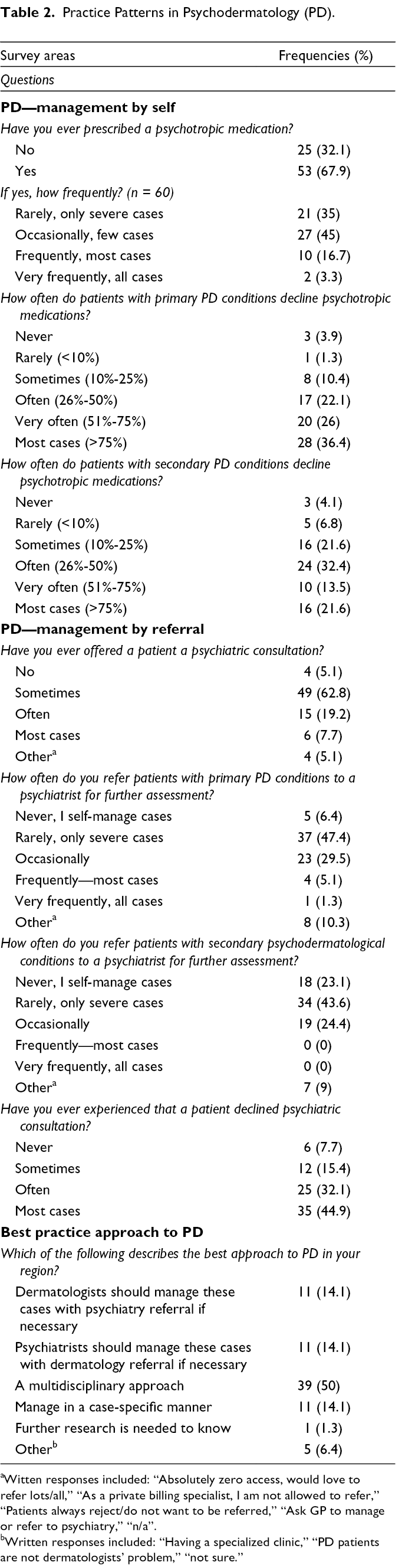
aWitten responses included: “Absolutely zero access, would love to refer lots/all,” “As a private billing specialist, I am not allowed to refer,” “Patients always reject/do not want to be referred,” “Ask GP to manage or refer to psychiatry,” “n/a”.
bWritten responses included: “Having a specialized clinic,” “PD patients are not dermatologists’ problem,” “not sure.”
Most participants reported referring psychodermatology patients to a psychiatrist, depending on the severity of the symptoms (Table 2). The majority answered that they refer to severe cases, 47.4% and 43.6% for primary and secondary psychodermatological conditions, respectively. Four out of 78 dermatologists reported referring to general practitioners instead of referring patients to psychiatry, with equal rates for primary and secondary psychodermatological conditions. A total of 61 participants provided responses to the open-ended question asking them to describe the referral process. Twenty-one of them (34.4%) reported accessibility issues to psychiatrists and/or psychologists. Eleven (18%) used negative expressions such as “poor,” “slow,” “difficult,” “dreadful,” and “horrible” to describe the referral process. Three (4.9%) reported frustration with a vague or malfunctioning process (eg, “I cannot think of one example of a successful referral,” “No one wants to see these patients,” and “There is no specific process to do it”). Most practitioners (62.8%) reported that they “sometimes” offer referral to psychiatry. Almost half (44.9%) responded that patients decline referral in most cases. In addition, 36.4% of dermatologists reported that >75% of patients with primary psychodermatological conditions and 21.6% of patients with secondary conditions declined treatment.
Challenges in Psychodermatological Practice
A total of 67 dermatologists responded to an open-ended question asking about the challenges in psychodermatology. In our survey, 26.9% of participants reported poor accessibility to psychiatrists and psychologists; 13.4% stated patients’ poor insight into their condition, with 32.8% reporting patients’ rejection of their diagnosis and treatment as the primary challenge. Other reported challenges included time constraints (16.4%), lack of training (16.4%), and poor communication with the patients (4.5%). In addition, 87.2% reported a lack of awareness of patient and family resources for these conditions.
Education and Training
Of all participants, 46.2% reported having never participated in a psychodermatology training (Table 3). Of the 42 physicians who reported some form of training in psychodermatology, 33.3% reported they received their training during residency, and 31% reported training through conferences. However, 68.9% reported that training in psychodermatology during residency was “poor” or “inadequate.” Of our participants, 55.1% expressed an interest in some psychodermatology training, with preferred formats being workshops and seminars.
Training in Psychodermatology (PD).
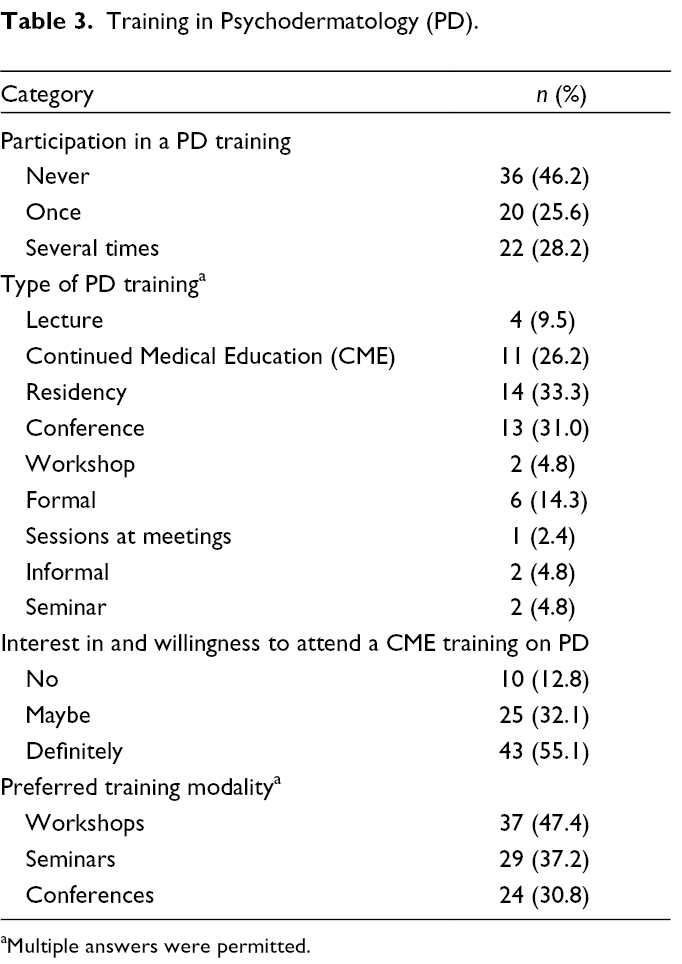
aMultiple answers were permitted.
Research and Future Development
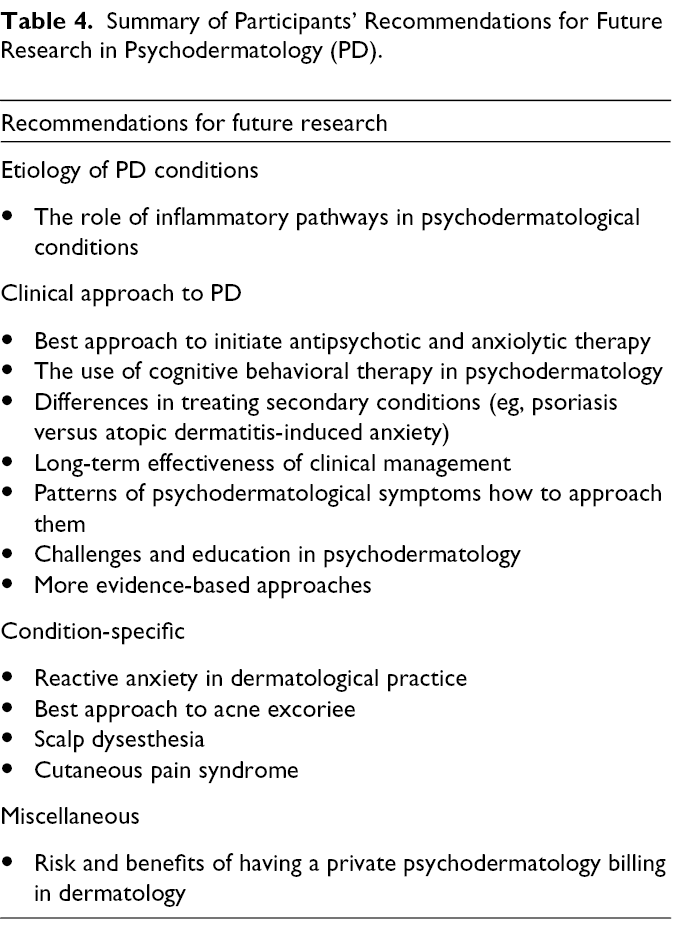
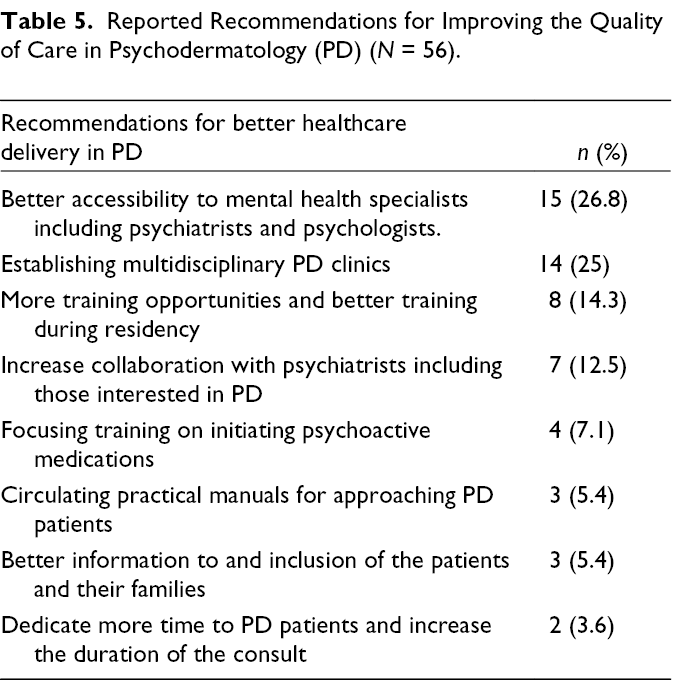
Only 2 of the queried physicians (2.6%) reported that research is adequate in the field of psychodermatology. Table 4 summarizes the responses we obtained on recommendations for future research. When asked about suggestions for future improvement in psychodermatology, 15 physicians (26.8%) emphasized the need for more collaboration with and accessibility to psychiatrists and psychologists. Fourteen physicians (25%) highlighted the importance of establishing specialized psychodermatology clinics. All other responses relating to recommendations for improving psychodermatology practice in the future are listed in Table 5.
Summary of Participants’ Recommendations for Future Research in Psychodermatology (PD).
Reported Recommendations for Improving the Quality of Care in Psychodermatology (PD) (N = 56).
Discussion
Our results highlight several challenges with knowledge, awareness, and healthcare delivery in psychodermatological practice in Canada. In line with several studies from locations outside Canada, 7,10,11 most of our participants’ perceived understanding and knowledge of psychodermatology is not optimal. Clinically, in a survey of 102 dermatologists in Chile, 12 less than half of the participants (41%) reported being comfortable to manage patients with psychodermatological conditions, which was similar in Turkey (specialists 40.4%, n = 70; residents 18%, n = 45). 11 Outcomes from a US-based survey study suggested that practitioners’ comfort level in treating these disorders vary by condition. While 83% of the 40 responders reported being comfortable in the diagnosis of trichotillomania, fewer (57%) were comfortable to diagnose underlying major depression and only 10% reported being comfortable to diagnose psychotic disorders and borderline personality disorder. 8
The frequency of psychodermatological conditions in dermatology practice is generally estimated to be 30%-40%. 1,3,4 However, few studies have reviewed the epidemiological characteristics of these conditions and most survey-based studies estimate the frequency based on dermatologists’ perception and practice patterns. Similar rates were observed in different studies where the majority of participants in all studies reported that psychodermatological conditions represent 10%-25% of their practice. 7,10,11 However, it is noteworthy that in our Canadian population, 20.5% of the dermatologists reported that more than 25% of their cases might be psychodermatological in nature. In Turkey, 40.3% of specialists (n = 70) and 46.5% of residents (n = 45) reported similarly high rates above 25% 11 ; in a Middle Eastern study, 18% (n = 57) of dermatologists reported a similar rate. 10 The reported frequencies of encounters with these patients, especially considering the practitioners’ relatively low comfort levels approaching these conditions, were striking and emphasize the need for more efforts to enhance the training and quality of care in psychodermatology. Validating the numbers in survey studies with more objective, population-based measures will achieve a more accurate estimate of the frequency of psychodermatological conditions in Canada. This remains crucial to understand and optimize current and future interventions.
Therapeutic approaches to psychodermatological conditions include a wide spectrum of interventions that can be pharmacological, psychological, or combined. Our results highlight the discrepancy between the high demand for psychodermatological services, difficulties in the referral process to psychiatry, and the high rates of patients who will not accept referrals to psychiatry. There are also low rates of dermatologists who reported being confident in managing and initiating psychopharmacological therapy themselves. All of these factors are implicated in possible shortfalls in healthcare delivery for psychodermatology patients and highlight the need for a multidisciplinary approach, which was reported by the majority of our dermatologists as the best way to tackle psychodermatology. This is also emphasized in a recent review of 23 psychodermatology clinical models where the authors concluded that these clinics can improve the quality of care, reduce the costs, and provide training opportunities. 13,14 In addition, in our survey, the top recommendation made by dermatologists to improve the quality of care to these patients was increasing access to mental health specialists. Furthermore, evidently, medico-legal consequences of inappropriate treatment and misdiagnoses should be avoided at all cost and—again—emphasize the importance of multidisciplinary approaches and the need to increase access, utilization, and acceptance of psychiatric consultations.
Regarding psychotropic prescription practices, antipsychotic and antidepressant medications were the most commonly reported drugs for the treatment of psychodermatological conditions. In dermatology, antipsychotics are mainly prescribed to treat patients with primary psychodermatological conditions such as delusions of parasitosis or other conditions in which the skin symptoms are thought to be driven by psychosis. 15 In our survey, the most commonly reported antipsychotic agent was risperidone, followed by pimozide. The latter is a high potency typical antipsychotic medication that traditionally was the drug of choice for treatment of delusions of parasitosis. 16 However, due to common and partly irreversible side-effects such as extrapyramidal symptoms (ie, acute dyskinesias and dystonic reactions), atypical antipsychotic medications such as risperidone are generally preferred today as they are associated with fewer adverse effects. 17 The relatively high numbers of pimozide use in our cohort raise the opportunity to promote the use of newer antipsychotic medications in dermatological practice, including for the treatment of delusional parasitosis. The most commonly prescribed antidepressant was doxepin. There is no preferred class of antidepressants in psychodermatology according to a comprehensive review on the use of these drugs in dermatology. 18 The first-line treatment of mood disorders in psychiatry would typically involve medications other than older tricyclic antidepressants like doxepin (eg, selective serotonin/noradrenaline reuptake inhibitors). Doxepin is frequently used for the treatment of pruritus in dermatology. The use of antidepressants in psychodermatology needs to be investigated further. To our knowledge, no previous study has queried dermatologists regarding their prescription patterns for psychoactive medications. More detailed investigations on the current use of specific psychotropic medications would be helpful to establish evidence-based guidelines for the use of these drugs in psychodermatology.
Several issues have been previously highlighted in dermatology training in Canada. An important example is a discrepancy in residents’ exposure to different areas of dermatology. 19 Our results emphasize the need for more training in psychodermatology. Sixty-eight percent of our participants rated psychodermatology training during residency as “poor” or “inadequate.” Similar to other studies, 7,10,11 we call for more training opportunities for residents and specialists, especially as 55.1% of the dermatologists in our survey indicate definite interest in such training.
This study has several strengths and limitations. To our knowledge, it is the first study to investigate psychotropic prescription rates of practicing dermatologists when they treat psychodermatological conditions. It is the first to investigate Canadian dermatologists’ perceived knowledge, awareness, and practice patterns surrounding psychodermatological conditions. The online nature of the survey may have affected our response rate and likely limited our reach to some dermatologists (ie, those who were unable or unwilling to provide information online as opposed to a paper format). As in any voluntary survey, we were only able to collect responses from interested participants. A less self-selected cohort would be more representative of all dermatologists. In addition, as our survey was an ad-hoc tool created by the authors, the wording of some questions might have been suboptimal. More efforts are recommended in future studies to validate and optimize the used surveys for more meaningful participation and, possibly, a better response rate.
Conclusion
We identified several challenges with knowledge, awareness, and healthcare delivery in psychodermatological practice in Dermatology in Canada. Increasing dermatologists’ access to psychiatric consultations/services, a multidisciplinary approach with dermatologists and psychiatrists co-providing care, and more specialized training in this area are recommended to narrow the identified gaps.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.