
Abstract
Verrucous carcinoma (VC) is a relatively rare locally aggressive, slow-growing, well-differentiated squamous cell carcinoma with minimal metastatic potential and is most frequent in the mucosa. Although rarely reported on the skin, cutaneous verrucous carcinomas (CVC) can appear anywhere, most commonly on the feet. However, clinical and pathologic diagnosis of CVC has been confusing and challenging. It can easily be mistaken for benign or more malignant conditions such as giant condyloma acuminata, keratoacanthoma, and pseudoepithelioma-like hyperplasia or squamous cell carcinoma, resulting in inappropriate management. In this review, we describe the different aspects associated with CVC, including its pathogenesis and clinicopathologic features. The available evidence for the differential diagnosis and treatment of CVC is discussed, and specific management recommendations are made. After the treatment, careful follow-up examinations of the excised area should be performed at regular intervals.
Introduction
Verrucous carcinoma (VC) is a rare and specialized form of well-differentiated squamous cell carcinoma (SCC) that usually involves the oral cavity, pharynx, esophagus, and skin. 1,2 Oral verrucous carcinoma, also known as Ackermann tumor, was first described by Ackermann in 1948 as a distinct low-grade malignancy. 3 However, later studies found that lesions can occur on any epithelial or mucosal structure. 4 Cutaneous verrucous carcinoma (CVC) can appear anywhere on the skin, most commonly on the feet and external genitalia, and is rarely reported in other parts of the body, such as the scalp, head and neck, axillae, arms, hands, shoulders, back, buttocks and thighs. 5 -11 Verrucous carcinoma has been known by many other names throughout history depending on the anatomical site, such as the Buschke-Lowenstein tumor for the genitourinary tract and epithelioma cuniculatum for the foot. 12 -14 Schwartz believes that these names have no particular academic value beyond respecting historical precedent and that a uniform diagnosis of verrucous carcinoma in a specific location would be more appropriate. 12 The clinical and pathologic diagnosis of CVC has been confusing and challenging. One of the major challenges in diagnosing CVC is the lack of repeatable criteria to distinguish this lesion from its mimics. 15 To raise awareness of the disease, we attempt to shed light on the etiology, pathogenesis, clinical features, histopathology, diagnosis, treatment, and prognosis of CVC in this review.
Etiology and Pathogenesis
The pathogenesis of VC remains unclear and there is an ongoing debate about the etiology and causative factors. It has long been believed that verrucous carcinoma is a malignant transformation of human papillomavirus (HPV) infection. 16 HPV types 6 and 11, 16 and 18, and 16 have been reported to be strongly associated with VC in the oral cavity, genital region, and foot, respectively. 17 -19 Most previous literature suggests that VC is thought to evolve from persistent irritated warts due to overlapping histologic features, and thus VC and giant condyloma acuminata (GCA) are on the spectrum of the same process. 20 However, Majewski et al. did not detect HPV types 16 and 18 in any of the 30 cases of penile VC. 21 In contrast to GCA, Pino et al. found that most of the cases of genital and anal VC diagnosed by strict histopathological criteria were negative for HPV testing. 20 Therefore, further studies remain to be performed to confirm whether HPV has a causal relationship with the development of VC.
The literature reports that chronic inflammation plays an important role in the development of CVC. Pătrașcu et al. reported that CVC is associated with abscesses and sinus tracts and that tumors can develop over osteomyelitis fistulas and chronic ulcers. 1 McArdle also reported another 49-year-old woman who presented with a nonhealing perianal abscess after years of chronic sacrococcygeal abscess and septic dermatitis, diagnosed as CVC. 22 In addition, pathologically, almost all cases of CVC show exudates and crusts, as well as inflammatory cell infiltration in the superficial dermis. Besides, CVC can occur secondary to a variety of chronic skin conditions such as lupus vulgaris, lichen planus, sclerosing lichen planus, lichen simplex chronicus, lupus erythematosus, erythema elevatum diutinum, actinic keratosis, scars, ulcers, hidradenitis suppurativa, and pilonidal sinus. 15,23 -34 These also further suggest the role of chronic inflammation may be involved in the pathogenesis.
Trauma, such as chronic mechanical and chemical injury to the skin, may also be considered a possible factor in the development of CVC, which is mainly related to the site of the tumor. 35 Penera et al. reported that CVC usually occurs in weight-bearing areas (e.g., plantar and sacropelvic areas), and thus the possibility of pressure damage as an etiology is increased. 4 In addition, the patient’s immune status, such as chronic underlying disease, use of immunosuppressive drugs, and HIV infection, may also be associated with disease progression. 1,36,37
Clinical Presentation
The incidence of CVC is uncertain due to the rarity of the disease. VC has been reported to account for 5% to 24% of the incidence of penile cancer, 1 with an estimated incidence of 0.75 to 3 for every million people in the general population. 19,38 VC is most often seen in middle-aged male patients, but vulvar VC has been reported to be more common in menopausal women. 39 CVC predominates in middle-aged to elderly people, with an average age of 50-60 years. 35,40 In contrast to typical SCC, CVC is rare at exposed sites and rarely occurs on the scalp and face. 41 In most cases, there is a history of 1 to 8 years of treatment before a definitive diagnosis, with a median disease duration of 5 years before the biopsy. 36 The tumor is insidious and grows slowly. 35 Initially an exophytic verrucous lesion, CVC gradually increases in size and invades deeper tissues as the disease progresses, and subsequently develops endophytically. 1 And it gradually causes extensive compression of the underlying soft tissues, producing globular, flocculent, and sometimes foul-smelling material. 27 Most lesions are solitary, but multiple lesions have been reported. 42,43
CVC can be found anywhere on the skin, with clinical features varying by site. CVC was most often found in the foot, including the balls of the foot (53%), toe (21%) or heel (16%). 35 CVC on the feet is often misdiagnosed as an ulcer or wart, is highly resistant to treatment, and requires vigilance for skeletal involvement. 35,36 The genitals are also frequently involved, with the most common site of involvement being the glans. 1 It often shows clinical features similar to those of GCA. However, the lesions of CVC tend to be more keratinized, hard, rough, and irregular. 44 In addition, it may invade surrounding organs, such as the urethra and pelvic organs, resulting in anterior urethral perforation or urethral fistula, as well as pelvic infiltration. 1,45 Inverted growth can also be observed in other skin sites, such as the buttocks, where the tumor presents as an invasive mass with a sinusoidal opening on the surface. 46 It may be more pronounced in men when hair follicles are involved. CVC in the buttocks is more likely to show sinus and purulence than in other areas (Figure 1).

CVC in the buttock clinically manifested as sinus and purulence.
Histologic Evaluation
The overall presentation of CVC is a prominent exo-endophytic growth pattern with blunt reticular ridges and pushing edges. 47 The epidermis shows prominent hyperkeratosis, parakeratosis, and papillary hyperplasia, with tight hyperkeratosis usually filling the interstices of the verrucous protrusions. 48 Irregular epidermal hyperplasia is composed mainly of well-differentiated eosinophilic keratinocytes that are large, with abundant cytoplasm, little nuclear atypia, and mixed with a minority of clear cells. 49 In the deeper layers, well-differentiated squamous cells and keratin-filled crypts are present and invade the dermis in a “pushing” “way” (Figure 2). Keratin-filled crypts can sometimes penetrate deep into the muscle and destroy surrounding bone. 50 Sometimes intraepidermal micro abscesses can be noted, which may be a clue to the diagnosis CVC. 51 Mitosis is rare and confined to the 1 or 2 layers of the tumor base. 36 There is no intercellular degeneration or mitotic activity except at the tumor margins, and very occasional cases of lesions may be found with frequent nuclei mitotic activity. 52,53 Moderate to severe chronic inflammatory infiltration, including lymphocytes, histiocytes, eosinophils, and plasma cells, are found in the dermis. 35 The fibrovascular core of the dermis is usually thin. 54 Reactive hyperplasia can be observed on the sides of the non-invasive epithelium adjacent to the tumor, manifesting as irregular acanthosis. 47 CVC sometimes shows abnormal maturation, cellular and nuclear atypia, and increased mitotic activity when growth is disturbed by factors such as pressure, and these cells easily penetrate the basement membrane. 49,55 This is particularly seen in CVC of the foot, which usually presents an endophytic growth pattern pathologically with thickening of the epidermis with elongation of rete ridges and sinus formation.
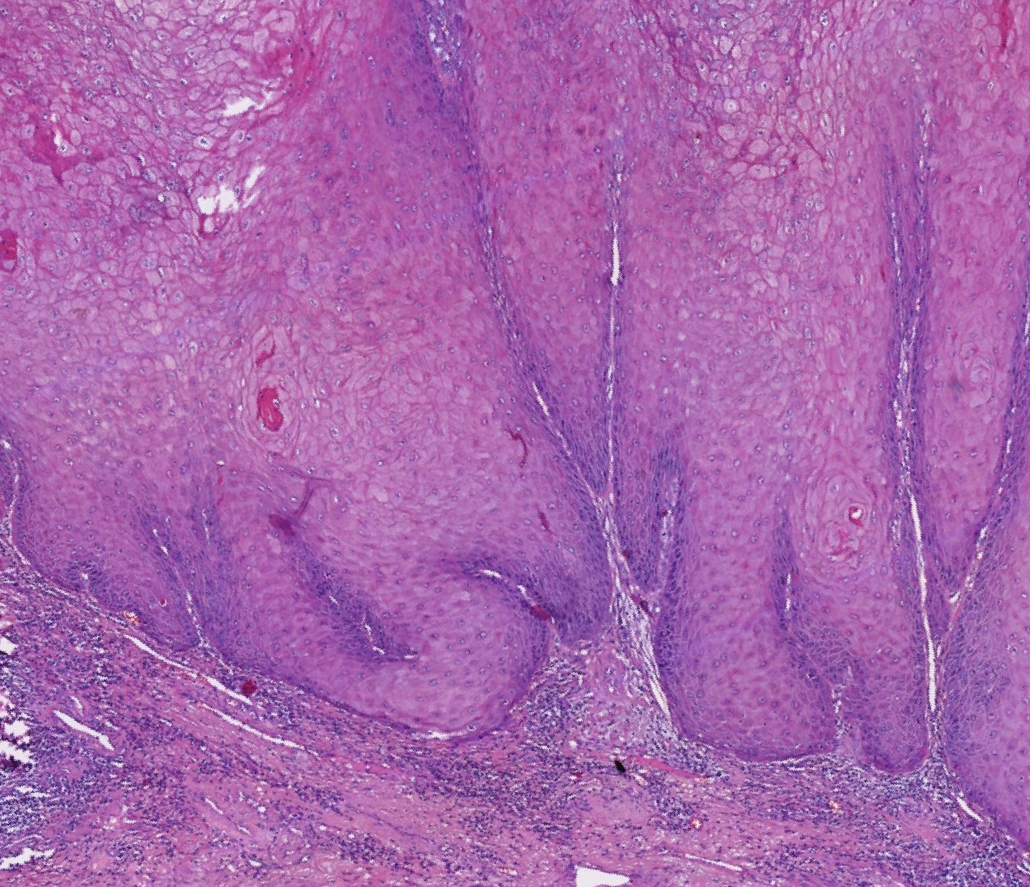
Histopathological characteristics of CVC showed blunted rete ridge with pushing margins. (HE × 40).
To date, there are still no definite and reliable markers, but there are some markers that help distinguish VC from its mimics. The p53 and Ki-67 proteins are expressed in all VC, especially at the basal cell layer and invasive areas. 9,56 In the basal layer of the VC, the ratio of p53-positive cells to p53-negative cells ranged from 43% to 58.3%. 57 It has been reported that there is a statistically significant difference in p53 between VC and pseudo-epitheliomatous hyperplasia (PEH). 9 In PEH, p53 and Ki-67 were detected only in the basal layer of the epidermis. In contrast, in CVC, they were detected in the lower third of the tumor island, while SCC show positive p53 expression throughout the tumor island. 57,58 Furthermore, expression differences in signal transduction mediators (c-erb, ERK-1 and 2, and RAF-1) and a range of cell cycle proteins, as well as the cell proliferation marker MIB-1 have been demonstrated in VC and typical SCC. 5,59 In VC, the expression of these molecules is confined to the basal layer, whereas in SCC they are patchily distributed throughout the tumor with a loss of polarity. 5
Differential Diagnosis
The lack of distinct malignant features of CVC emphasizes the need to distinguish it from its mimics. Differential diagnosis includes verruca vulgaris and GCA, keratoacanthoma (KA), PEH and SCC. 2,47,49 Verruca vulgaris presents as papillae growing outward from a central lesion projecting above the plane of the epidermis and koilocytes in the stratum granulosum. 60 In comparison to the “firm” appearance of CVC, clinically, GCA has a “soft” appearance, and pathologically, it shows koilocytes in the stratum granulosum without any endophytic growth pattern. 47 KA is characterized by a rapid self-limiting and self-healing process, and it proliferates in a nodular rather than a papillary pattern, lacking significant mitosis. 61 PEH is usually epidermal hyperplasia in response to a causative factor that disappears with the loss of the causative factor. 12,62 Histopathology of PEH mostly presents as downward basophilic acanthosis accompanied by sharp or irregular margins, with more prominent inflammatory infiltration. 47 In addition, cellular atypia and mitotic activity are sometimes common, but the nuclear polarity is preserved with little or no anaplasia. 63 In contrast to conventional SCC, cellular atypia in CVC is absent or rare, and mitotic figures are usually rare and focal. 35,64 The destruction of the basement membrane and the invasion of tumor cells into the dermis at different depths are diagnostic clues for SCC rather than CVC. 65
Treatment
The locally aggressive and metastatic nature of CVC leads to surgical excision as the recommended treatment. 66 The management of each case should be individualized, with histological margin control as the preferred surgical treatment option. 67,68 Mohs microsurgery maximizes the preservation of healthy tissue and helps maintain function and aesthetics. 69 The local recurrence rate after Mohs surgery was reported to be 16%, with a 3% incidence of nodal metastases and an absence of cases of distant metastases. 70 Reconstructive surgery and cosmetic surgery may be required when there is a large skin defect. 2
The contribution of radiotherapy has been controversial over the past decade due to the risk of anaplastic transformation. 1 Previous study proposed that anaplastic transformation was documented after radiotherapy. 71 However, data in the later literature showed that there is only a minimal chance of anaplastic transformation, on the contrary, it controls the local disease progression very well. Therefore, it can be considered as a separate treatment or in combination with surgery. 71,72 Radiotherapy should only be applied in carefully defined situations and minimizing the possibility of mutations is the initial choice for radiotherapy.
Photodynamic therapy can be therapeutic or used as a means of reducing the extent of surgical resection. 73 CO2 laser treatment offers good long-term results, especially in painless genital VC. 74 Local application of imiquimod in combination with CO2 laser has also been successful in some cases. 75 Intra-arterial methotrexate injections have been reported to be excellent in preserving the cosmetic and functional integrity of the penis, lips, and thumb CVC. 76,77 Kuan et al. reported that patients with multiple CVC were treated with oral retinoids successfully, and there were no recurrences at the 2-year follow-up. 42 Other treatment options include immunotherapy, cryosurgery, local or systemic chemotherapy (bleomycin, 5-fluorouracil, cisplatin, methotrexate), and intralesional recombinant interferon alfa. 12,73,78
A variety of treatments are available for the treatment of CVC, with surgical resection being the first choice. Alternatively, CVC may sometimes coexist with SCC, in which case further lymph node dissection is required after tumor resection. In addition, patients with a history of radiation therapy or multiple recurrences after inappropriate treatment should undergo a lymph node biopsy. 79
Prognosis
VC is classified as a well-differentiated malignancy that grows slowly, and can locally invade and destroy adjacent tissues, but has an exceedingly low metastasis rate and an overall good prognosis. 49 It has been reported that VC usually has a good prognosis with a 5-year survival rate of more than 75%. 80 Weber et al. believed that VC tends to grow around lymph nodes rather than into them. 81 Malignant transformation of VC to squamous SCC has been reported in 30 to 50% of cases. 82 Haidopoulos et al. found that up to 35% of patients in their study coexisted with SCC and VC. 83
The prognosis for CVC and VC is generally consistent. We reviewed 26 publications with a total of 115 patients with CVC and found that 19 patients recurred with a prevalence of 16.5% and a mean age of 59.6 years (range 38-91), 16 of whom (16/19,84.2%) within 2 years (2, 24 months) after surgery, however, one patient recurred at 26 months after surgery, and two patients were not available. 4 -6,11,12,15,27,30,35,36,42,47,49,62,68,73,74,77,84 -91 Of the recorded data on recurrence, there were 10 cases in men (10/16, 62.5%) and 6 cases in women (6/16, 37.5%). The majority (10/19 patients) of the recurrent cases were located on the foot, one each on the lower leg, axilla, ankle, and hand, in addition to five cases not documented. Metastasis occurred in a few cases (6/115)), including 5 cases with regional lymph node metastasis within 2 years after the operation, and 1 case without a record. Among all patients, only one 71-year-old male with a tumor located in the lower leg died due to CVC metastasis. 68
The long-term prognosis of CVC with definitive treatment is good. 88,92 However, due to the potential for local recurrence and metastasis even at histologically negative free resection margins, careful follow-up examinations and lymph node palpation of the resected area should be performed every 6 months. Furthermore, lymph node ultrasonography can be performed if the patient has a history of radiation. 68
Conclusion
In summary, CVC usually presents as a slow-growing, locally invasive tumor. Identification of the clinicopathologic features is essential to distinguish CVC from its mimics and to make an early diagnosis. The histopathology of CVC is characterized by an endo-exophytic growth pattern and irregular epidermal hyperplasia with well-differentiated keratinization and a “pushing” margin. The initial diagnosis of CVC is difficult to make accurate and often requires repeated histopathologic evaluation. Our review contributes to a better understanding of the disease and aids in early diagnosis and treatment. Also, we encourage early identification of CVC by appropriate deep tissue biopsy.
Footnotes
Acknowledgments
The patients in this manuscript have given written informed consent to publication of their case details.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.