
Abstract

Keywords
To the Editor:
A 74-year-old male tobacco smoker underwent two stages of Mohs micrographic surgery (MMS) for basal cell carcinoma (BCC) of the right nasal ala with the final defect measuring 1.2 cm x 0.8 cm (Figure 1a). The patient had history of keratinocyte carcinomas, including right nasal sidewall BCC treated with MMS and repaired with V-Y advancement flap 4 years prior. We present this case to highlight clinical pearls and to discuss a novel approach to nasal alar reconstruction utilizing a nasal sidewall-ala interpolation flap (NSAIF).
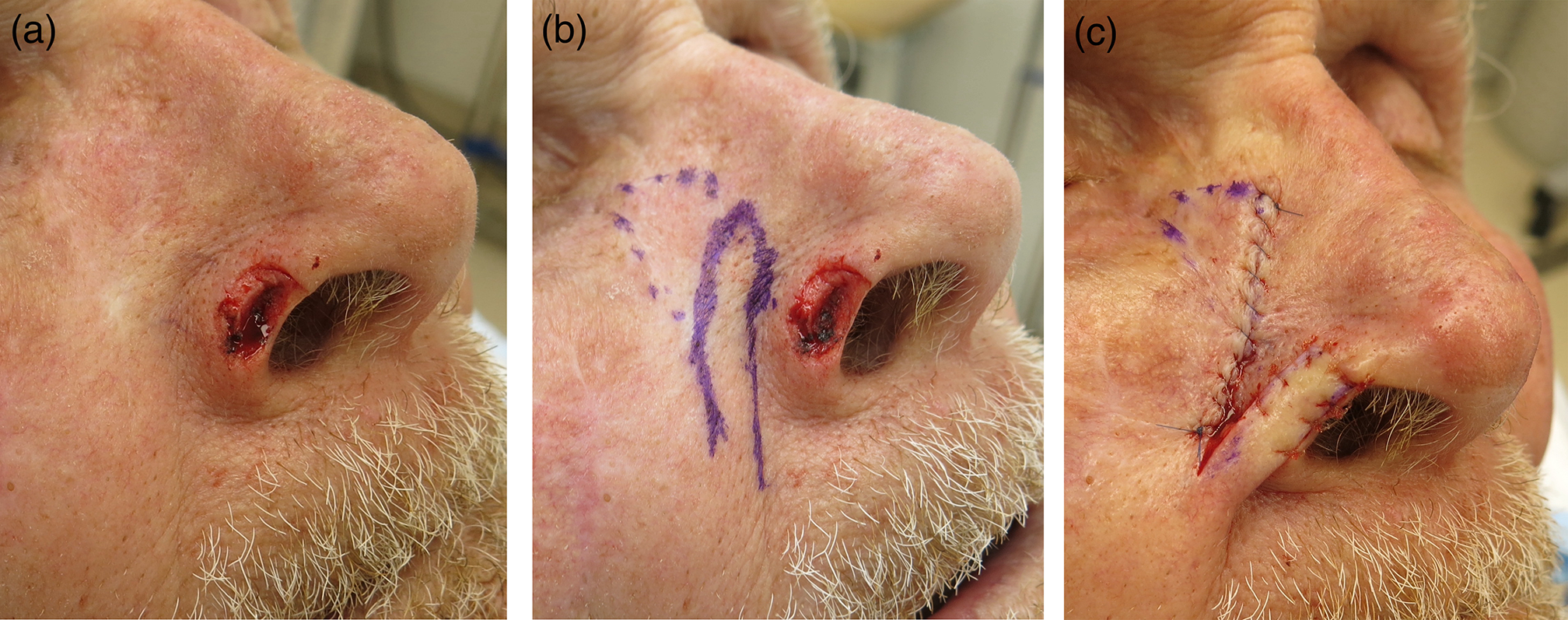
(
Surgical repair of nasal alar defects should maintain an adequate airway (function) and preserve contour and symmetry to the contralateral ala (form). Accomplishing these goals is complicated by insufficient adjacent tissue reservoir. 1 In our patient, additional factors included depth (deep fibrofatty tissue) and location (alar rim margin). Multiple repair options were considered. Secondary intention, while simplest, may cause alar retraction, constriction of the external nasal valve, and a hypopigmented, atrophic scar. Full thickness skin graft repair may cause ecnasion and suboptimal color and contour match. Free cartilage batten grafts have been used in defects near, but not often involving, the alar rim. 2 Composite grafts are typically considered for defects less than 1 cm. Furthermore, all graft repair options may be inferior choices in tobacco smokers. Bilobed transposition flaps have been used for smaller alar rim defects. 3
Interpolation flap repairs reliably preserve alar position and function. However, melolabial interpolation flaps may result in cheek asymmetry or introduce terminal hair from the donor site. 4 Paranasal interpolation flaps avoid these drawbacks, and given their smaller footprint, are easier for patients to manage while awaiting the second stage of reconstruction. 4 However, our patient’s prior MMS V-Y advancement flap scar encompassed the conventional paranasal flap donor site over the medial cheek and nasofacial sulcus. Our reconstructive solution was an NSAIF, which uses the nasal sidewall as a donor site instead of the medial cheek. This approach maintained nasal form and function, minimized cosmetic penalty at the donor site, and utilized a nasal sidewall flap pedicle that did not contain the previous surgical scar.
An NSAIF was designed on the nasal sidewall, immediately medial to the patient’s previous V-Y advancement flap scar (Figure 1b). The flap was incised down to the subcutaneous fat. The flap donor site was undermined in the deep subcutaneous level and the secondary defect was closed in a layered fashion. The flap was inset into the nasal alar defect under mild tension, helping to stent open the nostril, with interrupted cutaneous sutures. (Figure 1c).
NSAIF takedown was performed 3 weeks later. The flap pedicle was divided, the distal nasal ala portion was thinned and inset under tension with epidermal sutures, and the proximal pedicle base was excised elliptically and closed in a layered fashion. At 6-month follow-up, the surgical site demonstrated an excellent cosmetic outcome with preservation of alar bulk and contour and maintenance of the external nasal valve (Figure 2). The flap donor site was well camouflaged in the scar line of the previous V-Y advancement flap.

Clinical appearance at 6-month follow-up visit.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.