
Abstract
The pathogenesis of psoriasis is complex. Aryl hydrocarbon receptor (AhR) is a transcription factor that can be bound and activated by structurally diverse ligands and plays an important role in a range of biological processes and in the pathogenesis of different diseases. Recently, the role of AhR in psoriasis has attracted attention. AhR has toxicological functions and physiological functions. The overexpression and activation of AhR induced by the environmental pollutant and exogenous AhR agonist 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) can drive the development of psoriasis. This TCDD-mediated toxicological response disrupts the physiological functions of AhR resulting in skin barrier disorders and the release of inflammatory cytokines, 2 of the pivotal factors of psoriasis. In addition, highly upregulated kynureninase in psoriasis decreases endogenous AhR agonists, thereby weakening the physiological functions of AhR. Activating AhR physiological signalling should be useful in the treatment of psoriasis. Studies have demonstrated that physiological activation of AhR can dampen the severity of psoriasis. The oldest and effective treatment for psoriasis coal tar works by activating AhR, and both new anti-psoriasis drugs tapinarof and benvitimod are formulations of AhR agonist, supporting that activation of AhR can be used as a new strategy for the treatment of psoriasis. Preclinical and preliminary clinical studies have revealed the anti-psoriasis effects of a number of AhR agonists, providing potential candidates for the development of new drugs for the treatment of psoriasis.
Introduction
Psoriasis is a common chronic skin disease leading to a substantial burden for patients and society. Its pathogenesis is complex, involving dysregulation of immunological cell function as well as keratinocyte proliferation/differentiation. Th17 cells play a key role and are maintained by interleukin (IL)-23 produced mainly by dendritic cells (DCs). Th17 cells produce various cytokines, including IL-17A, IL-17F, and IL-22. IL-17A and IL-22 induce both keratinocyte proliferation and tumor necrosis factor (TNF)-α. Abnormal keratinocyte proliferation/differentiation leads to the dysfunction of skin barrier. Keratinocytes further promote inflammation. TNF-α accelerates the infiltration of inflammatory cells, including lymphocytes, monocytes, and neutrophils, from the peripheral blood into skin with DC activation. Oxidative stress (OS) plays a pathogenic effect in psoriasis that results in inflammation and impairment of skin barrier function.1 -3
Aryl hydrocarbon receptor (AhR) is a ligand-dependent transcription factor that plays a relevant role in many immune and inflammatory processes. In recent years, the role of AhR in psoriasis has received attention. 2 This review focuses on better understanding the relationship between AhR activation and the pathogenesis and treatment of psoriasis. We describe the evidence supporting AhR activation as a new therapeutic strategy for psoriasis. Finally, we collected data on preclinical or preliminary clinical studies of AhR agonists in the treatment of psoriasis to provide candidates for the development of new drugs for the treatment of psoriasis.
About AhR
AhR is a ligand-activated transcription factor 2 and belongs to the family of basic helix-loop-helix (bHLH)/Per-ARNT-Sim (PAS) proteins (Per: periodic; ARNT: AhR nuclear translocator; Sim: single-minded). 4 Structurally AhR consists of an N-terminal basic bHLH domain, 2 PAS domains (A and B), and a C-terminal transactivation domain. bHLH functions DNA binding, specifically recognizing and interacting with the xenobiotic response element (XRE) consensus sequence; PAS A functions dimerization with ARNT; PAS B functions ligand binding (ligand binding pocket). 4
The ligand-binding pocket of AhR is structurally flexible and can be bound and activated by structurally diverse ligands. 5 The ligands of AhR can be classified into natural and synthetic, 6 or exogenous and endogenous. 7
Inactive AhR is kept in the cytosol, forming complexes with molecular chaperones, including a dimer of 90 kDa heat shock protein. 4 On activation by ligands, the AhR mediates biological processes through genetic and nongenetic signalling pathways. Genomic signalling entails a canonical and a noncanonical pathway.
In the canonical pathway, ligand binding causes a conformational change of AhR which is released from the chaperone complex and in turn translocated into the nucleus to heterodimerize with ARNT. In the nucleus, the AhR/ARNT complex binds to XREs of target genes, regulating their transcription. 4
AhR target genes include those encoding cytochrome P450 superfamily enzymes (CYP1A1, CYP1A2, and CYP1B1) and AhR repressor (AhRR). 4 CYP1A1 can oxygenate AhR ligands, leading to their metabolic clearance, to play a feedback role that reduces the duration of AhR signalling. 8 AhRR suppresses AhR activity by binding to ARNT and XRE to modulate the transcription of AhR-dependent genes. 9
In the noncanonical signalling pathway, activated AhR forms complexes with different transcription factors in the nucleus, such as nuclear factor-κB (NF-κB), leading to its binding to non-XRE DNA elements to regulate expression of target genes. 4
Activation of AhR interacts with signalling networks including transforming growth factor-β/bone morphogenetic protein pathway, the canonical Wnt/β-catenin pathway, tyrosine kinase receptor pathways, including keratinocyte growth factor receptor, vascular endothelial growth factor (VEGF) receptor and epidermal growth factor receptor, and the Notch signalling pathway. 10 AhR is involved in a range of biological processes including xenobiotic metabolism, cell cycle regulation, reproduction, development, cellular and organismal homeostasis, and immune response. 2 AhR modulates the differentiation and function of CD4+ T cells including Th17 cells, Th22 cells, and Tregs, directly or indirectly through its effects on DCs. AhR also has effects on CD8+ T cells and γδT cells. 11 Furthermore, AhR is implicated in the pathogenesis of different diseases. 2
Toxicological and Physiological Functions of AhR
AhR has toxicological functions and physiological functions. Toxicological functions mediate responses to environmental toxicants, with 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) as the prototype agonist, 10 which can cause skin lesions such as chloracne. 12
The physiological functions of AhR maintain homeostasis in different tissues and cell types including skin. They can be activated by a number of endogenous AhR ligands. 10 Physiological activation of AhR ameliorates skin inflammation in mice and humans. 13
AhR and CYP1A1 are Overexpressed and Activated in Psoriasis
AhR is upregulated in the lesional skin of psoriasis,14 -16 in the peripheral blood mononuclear cells (PBMCs) from patients with psoriasis 17 and in the serum of psoriasis patients. 18 The expression of ARNT 14 and CYP1A115,16,19 in psoriasis skin lesions, and the expression of CYP1A1 in the PBMCs 17 and in the serum 18 from psoriatic patients are all upregulated. CYP1A1 is an AhR target gene. High expression of CYP1A1 in patients with psoriasis, coupled with colocalization of AhR and ARNT in the nuclei of lower epidermal keratinocytes 14 suggests activation of the AhR pathway. Increased CYP1A1 enzymatic activity degrades endogenous AhR ligands and impairs physiological AhR signalling, leading to disruption of its anti-inflammatory effects and exacerbating psoriasis inflammation. 20 Most important, AhR and CYP1A1 expression in psoriatic lesions were significantly and positively correlated with mean epidermal thickness and inflammatory cell density. 16 These findings putting together indicate that AhR overexpression and activation may contribute to psoriasis pathogenesis. 16
Activation of AhR by TCDD Drives Pathogenesis of Psoriasis
Air pollution21,22 and smoking 23 may increase the risk of psoriasis. TCDD is a ubiquitous environmental pollutant, 24 and is present in cigarette smoke. 25
AhR is expressed by keratinocytes and skin immune cells. 26 In normal human epidermal keratinocytes (NHEK) and HaCat cells, TCDD treatment increased AhR and CYP1A1 expression. In skin explants, AhR and CYP1A1 were significantly increased in TCDD-treated psoriatic skin biopsies compared with TCDD-treated normal skin. 15 In the course of TCDD-induced chloracne, epidermal hyperplasia and parakeratosis preceded comedones. 27 Parakeratosis, one of the histopathological features of psoriasis, is caused by abnormal keratinocyte differentiation 28 and can lead to skin barrier impairment. These findings suggest that TCDD activates AhR in keratinocytes and causes psoriatic epidermal changes.
TCDD binding also activates immune cells in psoriasis. PBMC and CD4+ T cells from psoriasis patients treated with TCDD showed increased AhR gene levels and significantly increased CYP1A1 expression compared with healthy controls. 17
Activation of the immune cells produces increased pro-inflammatory cytokines. Levels of the psoriasis-related cytokines IL-22 and IL-17 were significantly increased after TCDD treatment of PBMC from psoriasis patients. Treatment with TCDD induced an increase in the production of TNF-α, IFN-γ, IL-17, and IL-22 by CD4+ T cells in patients with psoriasis. 17 In ex vivo culture, proinflammatory cytokines (IL-1β, IL-6, and TNF-α) were significantly increased in TCDD-treated psoriatic skin biopsies compared with TCDD-treated normal skin. 15
Imiqimod (IMQ)-induced psoriasis mouse model experiments showed that TCDD aggravated skin inflammation and increased the expression of AhR, CYP1A1, TNF-α, IL-6, IL-17A, IL-22, IL-23, and NF-κB, supporting the above results of human studies. 29
OS plays an important role in the pathogenesis of psoriasis. 30 Activity of CYP1A1 can lead to intracellular production of reactive oxygen species (ROS) 31 and cause OS. Nuclear factor-erythroid 2-related factor 2 (Nrf2) activates antioxidative response in the epidermis. 32 In IMQ-induced psoriatic mouse model, TCDD inhibits the expression of Nrf2. 29 Nrf2 deficiency may lead to uncontrolled OS and promote the development of psoriasis.
TCDD-activated AhR induces the production of pro-inflammatory cytokines possibly also through inhibition of autophagy. Autophagy is an intracellular degradation and recycling process that participates in the regulation of inflammatory immune responses. 33 Autophagy expression levels are reduced in human psoriasis lesional skin. 14 TCDD-induced AhR activation causes autophagy inhibition in HaCaT cells and NHEK and skin biopsies from psoriasis patients. 15 This autophagy inhibition enhances the production of psoriasis-associated proinflammatory cytokines, IL-1β, IL-6, and TNF-α. 15
AhRR is another AhR target gene. 4 AhRR is overexpressed in the lesional epidermal skin of patients with psoriasis and TCDD increases pro-inflammatory cytokines associated with psoriasis skin tissue through activation of the AhRR/NF-κB signalling pathway. 34
Taken together, TCDD, an exogenous AhR ligand and environmental toxicant, induces AhR activation and drives the pathogenesis of psoriasis. This AhR activation belongs to the toxicological functions of AhR. 10
Physiological Functions of AhR in Skin
AhR mediates physiological functions that are dissociable from TCDD-induced toxicological functions. 10
Physiological AhR functions in skin are maintained and activated by endogenous AhR ligands. 35 Endogenous AhR agonists are readily metabolized and deleted by CYP1A1, resulting in transient AhR activation and thus physiological function. 36 In contrast, TCDD is a poor substrate of CYP1A1 and is metabolically stable, leading to sustained activation of the AhR and thus toxicological functions. 36 It is currently believed that TCDD-mediated toxicity actually represents an adaptive mechanism that overlaps with its physiologically conserved role and may disrupt physiological AhR signalling (see Figure 1).37,38
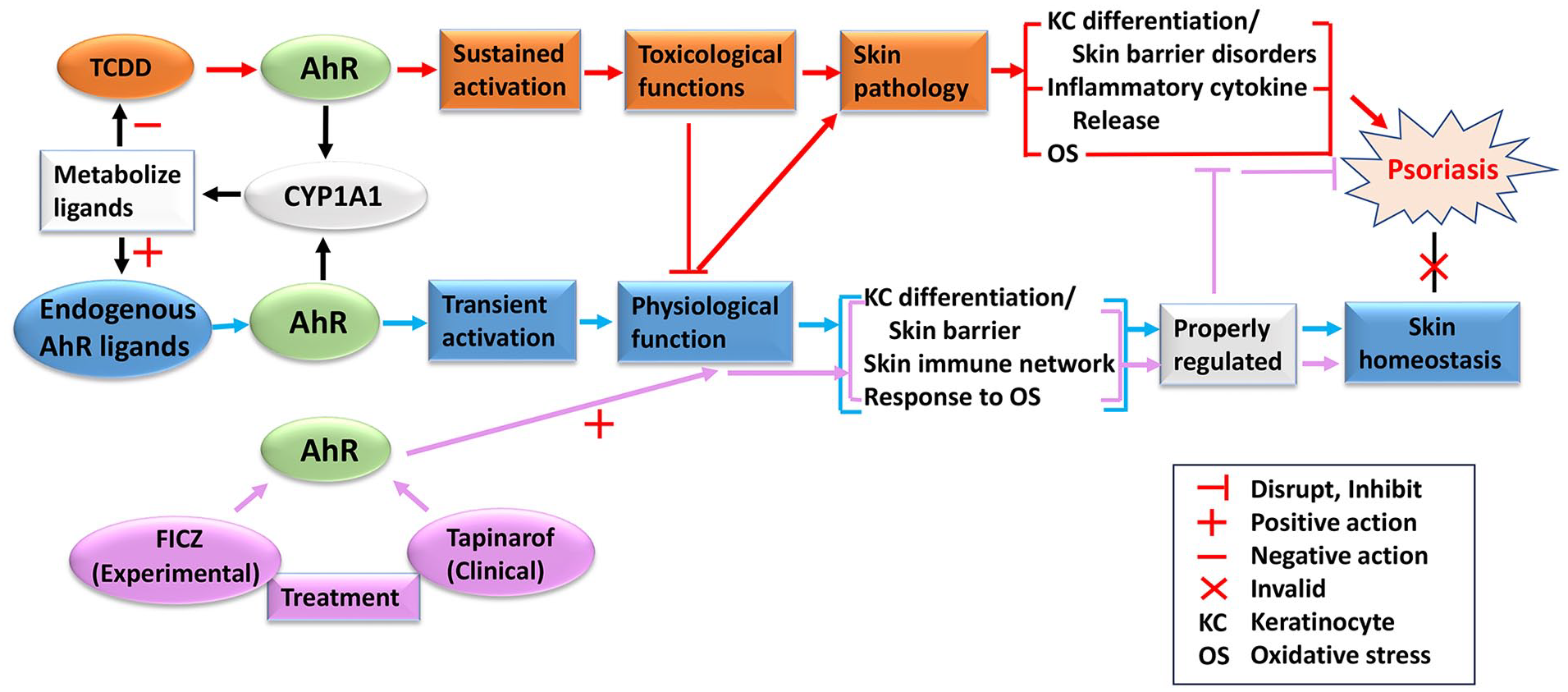
Skin AhR toxicological/physiological function and psoriasis. AhR, aryl hydrocarbon receptor; OS, oxidative stress; TCDD, tetrachlorodibenzo-p-dioxin; FICZ, 6-formylindolo[3,2-b]carbazole.
In healthy skin, AhR physiological functions assure skin homeostasis, 35 through appropriate regulation of the skin immune network, keratinocyte differentiation, skin barrier function, pigmentation, and responses to OS.2,3,39 Impaired AhR physiological function may lead to changes in keratinocyte differentiation/skin barrier and the release of inflammatory cytokines, thereby promoting the pathogenesis of psoriasis. 2 When AhR physiological functions are damaged due to toxicological reactions, these functions require a certain amount of endogenous AhR signalling to be effectively restored (see Figure 1). 36
Endogenous AhR Ligands Are Decreased in Psoriasis
KYNU, a key enzyme in the tryptophan metabolism pathway, is highly upregulated in psoriasis, possibly induced by TNF-α, a cytokine heavily present in the psoriatic micro-environment. 40
KYNU is downstream of indoleamine 2,3-dioxygenase (IDO) in the tryptophan metabolism pathway. Increased KYNU degrades the IDO-produced kynurenine, an endogenous AhR agonist. 40 Furthermore, KYNU also depletes tryptophan in the tissue, thereby interfering with the formation of a batch of tryptophan-derived AhR ligands, including 6-formylindolo[3,2-b]carbazole (FICZ), 13 kynurenic acid, cinnabarinic acid, and xanthurenic acid. 41 Reduced levels of these endogenous AhR ligands in psoriatic skin may weaken the physiological AhR signalling and thus result in increased expression of inflammatory mediators in the skin. 13
AhR Activation and the Treatment of Psoriasis
AhR activation by TCDD induces toxicological responses. Furthermore, high expression of KYNU reduces endogenous ligands in psoriasis. Both events impair the physiological functions of the AhR and drive the pathogenesis of psoriasis.13,37 Activating AhR physiological signalling should help treat psoriasis. 2
The studies by Di Meglio et al 13 showed that FICZ (an endogenous AhR agonist)-induced physiological AhR signals reduced 70% of psoriasis-upregulated genes in lesional skin samples from psoriatic patients, while AhR antagonist was able to increase the expression of these genes. Thus, AhR physiological functions appear to play an important role in modulating the severity of psoriasis. 13 Another study showed that the elevated levels of IFN-γ, IL-17, and IL-22 in CD4+ T cells from patients with psoriasis were significantly reduced after FICZ treatment. 17
In the IMQ-induced mouse psoriasis model, AhR activation with the endogenous ligand FICZ ameliorated the inflammatory profile, whereas AhR-deficient mice showed exacerbated skin inflammation. Absence of AhR on mouse or human keratinocytes caused excessive inflammation. 13 The efficacy of tapinarof, a natural AhR ligand for treatment of psoriasis, has been showed to be attribute to activation of AhR, 3 similar to the endogenous AhR agonist FICZ. These findings indicate that physiological activation of AhR can dampen the severity of psoriasis. 13 The beneficial effects of AhR activation suggest that AhR stimulation may be a therapeutic mechanism in the treatment of psoriasis (see Figure 1).2,13
AhR Agonists for Treating Psoriasis: From Coal Tar to the Present
Coal Tar
Coal tar is one of the oldest and highly effective treatment for psoriasis. Unexpectedly, the mechanism by which coal tar has therapeutic effects has been rarely studied. It is worth noting that van den Bogaard et al 42 reported in 2013 that they found that coal tar activates the AhR in keratinocytes, resulting in induction of epidermal differentiation accompanied by induced expression of terminal differentiation proteins pivotal for barrier function, and demonstrated that AhR signalling is required for normal keratinocyte differentiation. 42 These findings may explain, at least in part, the mechanism by which coal tar is effective in treating psoriasis.
Tapinarof and Benvitimod
Both tapinarof and benvitimod are topical formulations of 2-isopropyl-5-[(E)-2-phenylethenyl] benzene-1, 3-diol (IPBD). Tapinarof cream 1% once daily differs from benvitimod (WBI-1001) 1% twice daily in that it comprises a novel vehicle with specific excipients. They have been investigated in separate clinical trials. 43
IPBD is a novel synthetic compound originally derived from metabolites of a unique group of bacterial symbionts of entomopathogenic nematodes, also named WBI-1001. 44
Tapinarof
The impact of tapinarof on psoriasis involves immune modulation, skin barrier normalization, and antioxidant activity. In a T-cell polarization assay, tapinarof markedly inhibited T-cell proliferation and Th17-cell differentiation and reduced the production of IL-17. In IMQ-induced mouse model of psoriasis, tapinarof reduced skin inflammation and decreased tissue proinflammatory cytokine including IL-17A, IL-17F, IL-19, IL-22, IL-23, and IL-1β expression. The anti-inflammatory effects of tapinarof are mediated via activation of the AhR pathway. Studies have shown that tapinarof induces the expression of skin barrier genes related to keratinocyte differentiation that are downregulated in psoriasis, including filaggrin and loricrin via modulation of the AhR signalling pathway. (see Figure 1) 3
Tapinarof can directly scavenge ROS and also induces the AhR-Nrf2 transcription factor pathway, leading to expression of antioxidant enzyme genes to reduce ROS. Combined antioxidant responses via the Nrf2 pathway and direct ROS scavenging by tapinarof may jointly reduce epidermal OS. 3 These effects of tapinarof are consistent with the role of AhR activation in immune-mediated inflammatory responses, skin barrier gene expression, and antioxidant activity (see Figure 1). 45
In 2019, a phase 2 double-blind, vehicle-controlled, randomized dose finding trial in adults with mild-to-severe psoriasis showed that at 12 weeks statistically significant differences (at .05 significance level) were demonstrated between all the tapinarof treatment groups and the vehicle groups in treatment success, as defined by Physician Global Assessment (PGA) scores and Psoriasis Area and Severity Index (PASI) 75 rates. Almost all patients who achieved either PGA 0 or 1 or PASI 75 using tapinarof demonstrated maintenance of the efficacy level for 4 weeks after the end of the study treatment. It is confirmed that tapinarof is efficacious, with an acceptable safety profile in the adult plaque psoriasis population. 46
In 2021, 2 identical phase 3 randomized trials of tapinarof, enroling 510 and 515 patients with mild-to-severe plaque psoriasis, respectively, were published. Patients were randomly assigned in a 2:1 ratio to use tapinarof 1% cream or vehicle cream once daily for 12 weeks. A PGA response occurred in 35.4% of the patients in the tapinarof group and in 6.0% of those in the vehicle group in trial 1 and in 40.2% and 6.3%, respectively, in trial 2 (P < .001 for both comparisons). A PASI 75 response occurred in 36.1% of the patients in the tapinarof group and in 10.2% of those in the vehicle group in trial 1 and in 40.2% in the tapinarof group and 6.3% in the vehicle group in trial 2 (P < .001 for both comparisons). Adverse events with tapinarof cream included folliculitis, nasopharyngitis, contact dermatitis, headache, upper respiratory tract infection, and pruritus, with no serious adverse events that were considered by the investigators to be related to tapinarof. The authors concluded that tapinarof 1% cream once daily is superior to vehicle control in reducing the severity of plaque psoriasis. 47 A total of 763 patients who completed the 12 week trial received 40 weeks of open-label treatment and 4 weeks of follow-up to assess long-term safety, efficacy, remittive effect, durability of response, and tolerability of tapinarof. Efficacy improved beyond the 12 week trials, with a 40.9% complete disease clearance rate, ∼4 month off-therapy remittive effect, durability on therapy, and consistent safety. 48
In May 2022, tapinarof cream 1% was approved in the United States for the topical treatment of plaque psoriasis in adults. 45
Benvitimod
It is currently agreed that the mechanism by which benvitimod treats psoriasis lies in activating AhR. Keratinocytes play a crucial role in the development and progression of psoriasis. A recent study showed that IL-22 treatment induced HaCaT cell proliferation and that benvitimod significantly inhibited this effect. The antiproliferative effects of benvitimod were determined to be mediated through inhibition of the JAK/STAT3 (Janus kinase/signal transducers and activators of transcription) pathway by AhR. In vivo, benvitimod significantly inhibited imiquimod-induced psoriatic skin lesions and suppressed the proliferation marker PCNA (proliferating cell nuclear antigen) in the epidermis. 49
In 2012, Bissonnette et al 50 reported a phase IIa double-blinded and placebo-controlled clinical trial, in which a total of 61 adults with mild-to-moderate plaque psoriasis were randomized (2:1) to apply 1% WBI-1001 (also known as benvitimod in the literature) in a cream formulation or vehicle twice daily. At week 12, the improvements in both PGA and PASI in the WBI-1001 group were significantly greater than in the placebo group (P < .0001). Adverse drug reactions were all mild or moderate in intensity. Topical WBI-1001 induces significant improvement in patients with plaque psoriasis.
In 2020, a phase III clinical trial was published, in which 686 patients with mild-to-moderate plaque psoriasis were randomized (2:1:1) to receive 1% benvitimod (WBI-1001) cream, 0.005% calcipotriol ointment, or placebo twice a day. At week 12, 50.4% of patients in the benvitimod group achieved PASI 75, which was significantly higher than that in the calcipotriol (38.5%, P < .05) and placebo (13.9%, P < .05) groups. The percent of patients achieving a PGA response in both the benvitimod group (66.3%) and calcipotriol group (63.9%) were significantly higher than that in the placebo group (34%, P < .05). Adverse events included application site irritation, follicular papules, and contact dermatitis. No systemic adverse reactions were reported. The authors concluded that benvitimod cream is effective and safe in patients with mild-to-moderate plaque psoriasis. 51
In 2019, 1% benvitimod cream was approved as a topical drug for the treatment of mild-to-moderate plaque psoriasis in China. 52
AhR Agonists: Potential Candidates for Developing New Drugs to Treat Psoriasis
Based on the accumulated data, especially the research on the anti-psoriasis mechanism of FICZ and tapinarof through the AhR pathway, it is sufficient to believe that activation of AhR can be used as a new strategy for the treatment of psoriasis.2,13 AhR agonists that promote keratinocyte differentiation and suppress immune responses are potential for the treatment of psoriasis. 39 In the recent years, preclinical and preliminary clinical studies have shown the anti-psoriasis effects of a number of AhR agonists, providing potential candidates for the development of new drugs for the treatment of psoriasis (see Table 1).
AhR Agonists: Potential Candidates for Developing New Drugs to Treat Psoriasis.
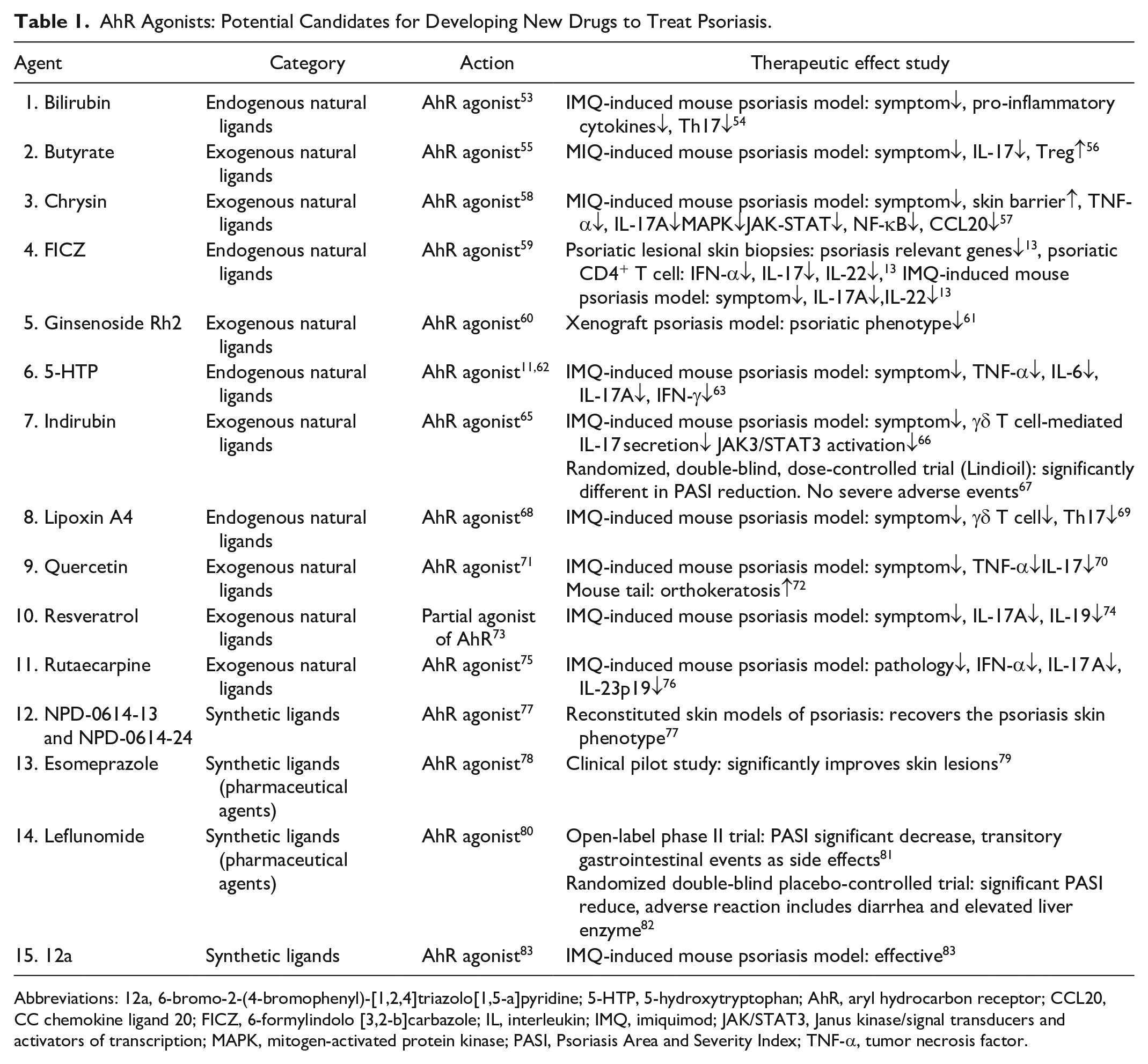
Abbreviations: 12a, 6-bromo-2-(4-bromophenyl)-[1,2,4]triazolo[1,5-a]pyridine; 5-HTP, 5-hydroxytryptophan; AhR, aryl hydrocarbon receptor; CCL20, CC chemokine ligand 20; FICZ, 6-formylindolo [3,2-b]carbazole; IL, interleukin; IMQ, imiquimod; JAK/STAT3, Janus kinase/signal transducers and activators of transcription; MAPK, mitogen-activated protein kinase; PASI, Psoriasis Area and Severity Index; TNF-α, tumor necrosis factor.
Bilirubin
Bilirubin, a heme degradation product, is an endogenous AhR agonist. 53 Insolubility in water is a limitation of bilirubin. Bilirubin-based nanoparticles (BRNPs) may overcome this critical issue. BRNPs are composed of bilirubin and a hydrophilic polyethylene glycol (PEG) polymer base to act as stimulus-responsive drug-delivery vehicles. Topical BRNPs can readily penetrate the outer cornified skin layer in psoriatic skin and become internalized into activated keratinocytes and antigen-presenting cells (APCs). As a therapeutic nanomedicine, BRNPs alleviate psoriatic symptoms in the IMQ-induced mouse model and reduce the psoriasis-related pro-inflammatory cytokines and Th17 cells. The experimental therapeutic efficacy of BRNPs is comparable to that of the steroid medicine, clobetasol propionate. 54
Butyrate
Butyrate, a short chain fatty acid derived from bacterial fermentation of dietary fibres, is an agonist of AhR. 55 In an IMQ-induced mouse psoriasis model, topical sodium butyrate reduced the skin lesions, downregulated IL-17, and induced Treg. 56
Chrysin
Chrysin, a flavonoid extracted from passionflower, honey, and propolis, 57 is a natural agonist of AhR. 58
Studies have shown that chrysin reduces IMQ-induced psoriasis-like skin lesions in mice and improves the skin barrier. Chrysin also suppresses the TNF-α, IL-17A, or IL-22-induced phosphorylation of mitogen-activated protein kinase (MAPK) and JAK/STAT pathways, activation of NF-κB pathway, and expression of CC chemokine ligand 20 (CCL20) and antimicrobial peptides in epidermal keratinocytes, indicating that chrysin could ameliorate the inflammatory reactions induced by these proinflammatory cytokines relevant to psoriasis. 57
FICZ
FICZ is an endogenous agonist of AhR derived from tryptophan. 59 FICZ treatment strikingly decreased the psoriasis relevant genes in psoriatic lesional skin biopsies. 13 FICZ treatment decreased the levels of IFN-α, IL-17, and IL-22 in CD4+ T cells from patients with psoriasis. 17 FICZ systemic administration ameliorates IMQ-induced psoriasiform skin inflammation in mice and reduces expression of IL-17A and IL-22. 13
Ginsenoside Rh2
Ginsenoside Rh2 (GRh2), a protopanaxadiol-type ginsenoside, is an AhR agonist. 60 GRh2 suppresses psoriatic features in a mouse xenograft psoriasis model that receives human psoriatic nonlesional skin grafts to develop a psoriatic phenotype, reducing acanthosis, T lymphocytes, vessel density, and VEGF-A. Treatment with an antagonist of VEGF mimics the effects of GRh2. GRh2 may have an anti-psoriasis effect through angiogenesis suppression. 61
5-Hydroxytryptophan
5-Hydroxytryptophan (5-HTP), a hydroxylated derivative of tryptophan, is a mild AhR agonist.11,62 5-HTP attenuated IMQ-induced psoriasiform dermatitis in mice, decreased the TNF-α, IL-6, IL-17A, and IFN-γ in skin and serum. 5-HTP significantly inhibited keratinocyte activation with decrease in IL-6 production and p-extracellular signal-regulated kinase 1/2 and p-STAT3 expression. 5-HTP also inhibited the differentiation of IFN-γ- and IL-17A-expressing CD4+ T cells and related cytokine production in splenocytes. 63
Indirubin
Indirubin, a bis-indole alkaloid obtained from various natural sources, is one of the main bioactive components of Indigo naturalis. 64 Indirubin is an AhR agonist. 65 Oral administration of indirubin ameliorates IMQ-induced psoriasis in mice, mainly by inhibiting γδ T cell-mediated inflammatory responses involving IL-17 secretion and JAK3/STAT3 activation. 66
Lindioil is an ointment primarily composed of indirubin. In a randomized, double-blind, dosage-controlled trial, 91 patients with plaque psoriasis were treated with Lindioil containing 200, 100, 50, or 10 μg/g of indirubin twice daily for 8 weeks. The reduction in PASI score was significantly different among the 4 groups with the 200 μg/g group being the largest. No severe treatment-related adverse events were reported. Lindioil is effective and safe for treating psoriasis. 67
Lipoxin A4
Lipoxin A4 (LXA4), a metabolite for arachidonic acid, is an AhR agonist. 68 LXA4 inhibits the production of inflammatory cytokines and cell proliferation of human epidermal keratinocytes (NHEK). LXA4 alleviates IMQ-induced psoriasis-like dermatitis, reduces the proportion of IL-17A-producing γδT cells in skin and skin draining cervical lymph nodes, and the proportion of Th17 cells in spleens. 69
Quercetin
Quercetin, a dietary flavonoid abundant in many natural plants, 70 is an AhR ligand and acts as an AhR activator. 71 Quercetin significantly attenuated IMQ-induced psoriasis-like lesions in mice, reducing TNF-α and IL-17. The underlying mechanism may be associated with improving anti-inflammatory and antioxidant status and inhibiting the activation of the noncanonical NF-κB signalling. 70 In the mouse tail test for anti-psoriatic potential, quercetin significantly promoted the terminal differentiation of keratinocytes. Moreover, quercetin showed appreciable antiproliferant activity in HaCaT cell line. 72
Resveratrol
Resveratrol, a natural phenolic compound produced by several plants including grapes, nuts, and berries, 73 is a partial agonist of AhR. 73 Resveratrol significantly alleviated the IMQ-induced psoriasis-like skin inflammation in mice and decreases IL-17A and IL-19. 74
Rutaecarpine
Rutaecarpine (RUT), an indolopyridoquinazolinone alkaloid isolated from Evodia rutaecarpa (Juss.), is a promising naturally derived AhR agonist. 75 RUT treatment improved IMQ-induced psoriasis-like dermatitis pathology and downregulated the expression of IFN-α, IL-17 A, and IL-23p19 in the skin lesions, as well as their levels in the serum in mice. 76
NPD-0614-13 and NPD-0614-24
NPD-0614-13 and NPD-0614-24 are 2 new synthetic AhR agonists structurally related to the natural agonist FICZ. They recovered the altered proliferation and counteracted the proinflammatory effects in human keratinocytes stimulated with TNF-α, and showed pro-differentiative and anti-inflammatory effects in a human epidermal and full-thickness reconstituted skin models of psoriasis. These data provide the basis for considering NPD-0614-13 and NPD-0614-24 as potential new drugs for the treatment of psoriasis. 77
Esomeprazole
Esomeprazole, a classical benzimidazole derivative—proton pump inhibitor, is an agonist of AhR. 78 In a pilot study, the PASI values of 10 psoriatic patients treated with oral esomeprazole 40 mg BID (twice a day) for 90 days reduced from 5.52 ± 2.93 to 0.89 ± 0.74 (P = .0002). 79
Leflunomide
Leflunomide, an immunomodulatory drug, is an AhR agonist. 80
In a phase II trial, eight psoriatic patients received oral leflunomide 20 mg daily for 12 weeks. PASI score decreased from 20.08 ± 6.85 to 12.51 ± 11.83 (P = .03). Adverse reactions primarily consisted of transitory gastrointestinal events. 81 A randomized double-blind placebo-controlled trial including 190 patients demonstrated that oral leflunomide is effective for plaque psoriasis. Significant differences in favour of leflunomide were observed in the PASI (PASI 50 in 30.4% of patients vs 18.9% for placebo; P = .05). Diarrhea was the most common adverse events. Adverse drug reactions included elevated liver enzyme. No serious liver toxicities occurred. 82
6-bromo-2-(4-6-bromo-2-(4-bromophenyl)-[1,2,4]triazolo[1,5-a]pyridine (12a)
The 12a, a derivative of triazolopyridine, is an AhR agonist. The 12a promotes skin barrier repair and reduces OS. Both topical and oral 12a significantly mitigated IMQ-induced mouse psoriasis-like skin lesion and reduced IL-17. Furthermore, 12a possesses good pharmacokinetic properties and safety. Therefore, 12a can be taken as a candidate of new drug development for psoriasis. 83
Conclusion
AhR has toxicological functions and physiological functions. The formal may disrupt the later, resulting in pathological processes. In this case, activation of AhR is required to restore the physiological functions.
In psoriasis, both AhR and CYP1A1 are upregulated, suggesting that AhR overexpression and activation may contribute to the pathogenesis of the disease.
TCDD, an environmental pollutant and exogenous AhR ligand, activates AhR to drive the pathogenesis of psoriasis. This must be a toxicological response and can disrupt the physiological AhR functions. Therefore, the treatment of psoriasis requires activating the physiological signalling of the AhR to restore its physiological function. Furthermore, high expression of KYNU in psoriasis leads to a reduction in the pool of tryptophan-derived endogenous AhR agonists, thus weakening the physiological function of AhR normally maintained by endogenous AhR agonists and increasing the need for therapeutic activation of AhR.
Studies on psoriasis patients and animal models have shown that activating the physiological function of AhR with the endogenous agonist FICZ can dampen the severity of psoriasis. Both the oldest and effective treatment for psoriasis coal tar and the new anti-psoriasis drug tapinarof work by activating AhR. Based on the accumulated data, especially the research on the anti-psoriasis mechanism of FICZ and tapinarof through the AhR pathway, it is sufficient to believe that activation of AhR can be used as a new strategy for the treatment of psoriasis. AhR agonists that promote keratinocyte differentiation and suppress immune responses are potential for the treatment of psoriasis. AhR agonists showing anti-psoriasis effects in preclinical and/or preliminary clinical studies may be offered as potential candidates for the development of new drugs for the treatment of psoriasis.
Supplemental Material
sj-docx-1-cms-10.1177_12034754241239050 – Supplemental material for The Role of Aryl Hydrocarbon Receptor in the Pathogenesis and Treatment of Psoriasis
Supplemental material, sj-docx-1-cms-10.1177_12034754241239050 for The Role of Aryl Hydrocarbon Receptor in the Pathogenesis and Treatment of Psoriasis by Xiran Lin, Xianmin Meng and Jingrong Lin in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.