
Abstract

To the Editor:
Cutaneous lupus erythematosus sometimes produces a considerable challenge in clinical dermatology due to its diverse manifestations and impact on patient quality of life. Among its variants, discoid lupus erythematosus (DLE) and subacute lupus erythematosus (SCLE) are notable for their distinct patient profiles, each bearing unique therapeutic implications. 1 Despite extensive research into their pathophysiological distinctions, there remains a gap in knowledge as to how these differences manifest clinically in patients’ demographic distributions, comorbidity profiles, and medication usage patterns. By systematically comparing and elucidating the critical differences in patient disease profiles and treatment regiments of SCLE versus DLE patients, we aim to contribute to a more differentiated diagnostic and therapeutic framework for clinicians.
We performed a retrospective analysis in the All of Us database, a component of the National Institute of Health’s (NIH) Precision Medicine Initiative that containing de-identified patient health records from over 1 million participants. Patients were dichotomized by DLE (SNOMED codes 200938002 and 79291003) and SCLE (SNOMED code 239891002) status. Demographics, medications prescribed, and comorbidity data were collected and compared following lupus diagnosis. Chi-square test was used to compare categorical variables (demographics, comorbidities, and medications) and Student’s t test was used for age comparisons. Confounding factors were accounted for by adjusting for demographics and baseline comorbidities. P < .05 was considered significant. All analyses were conducted in Python (V3.8).
A total of 992 DLE and 81 SCLE patients were included. SCLE patients were, on average, older than DLE patients (54.0, SD: 15.0 vs 49.5, SD:14.6; P = .008). The racial distribution significantly varied between SCLE and DLE patients (P = .003), with 74.63% of SCLE and 49.65% of DLE patients being white. Furthermore, 19.40% of SCLE patients were Black/African American while 42.52% of DLE patients were Black/African American (Supplemental Table S1).
A total of 17,282 and 1676 prescription records were obtained from DLE and SCLE patients, respectively. DLE patients were prescribed azathioprine (2.29% vs 0.78%, P < .001) and mycophenolate mofetil (13.44% vs 3.34%, P < .001) significantly more than SCLE patients. Contrarily, SCLE patients were prescribed chloroquine phosphate (1.25% vs 0.26%, P < .001) methotrexate (12.47% vs 5.87%, P < .001), prednisone (42.24% vs 38.04%, P < .001), and triamcinolone acetonide (9.13% vs 4.50%, P < .001) significantly more than DLE patients (Table 1).
Univariant Chi-Square Analysis of Common Lupus Medications in DLE Versus SCLE Patients.
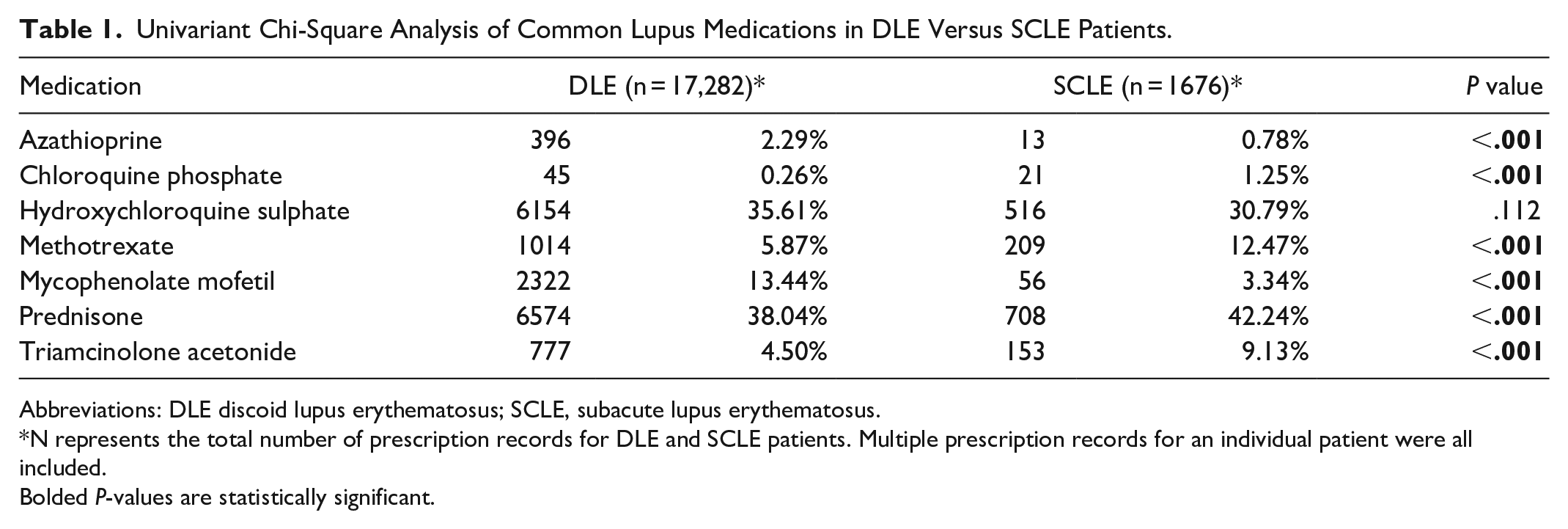
Abbreviations: DLE discoid lupus erythematosus; SCLE, subacute lupus erythematosus.
N represents the total number of prescription records for DLE and SCLE patients. Multiple prescription records for an individual patient were all included.
Bolded P-values are statistically significant.
Comorbidity analysis demonstrated an increased occurrence of keratoconjunctivitis sicca in Sjögren’s syndrome in SCLE patients compared to DLE patients (12.35% vs 4.74%; P = .016; Supplemental Table S2).
The older age at diagnosis of SCLE can be attributed to a drug-induced etiology—the most common subtype in the elderly. 2 The increased use of medications for age-related comorbidities, such as antihypertensives and relatively new biologic and chemotherapeutic agents, delayed symptom development following exposure, and older age of onset supports this concept.3,4 SCLE manifests more insidiously with no induration as compared to DLE, providing greater impetus for later medical consultation. 5 SCLE more commonly presents with multi-organ involvement and progresses to SLE, necessitating systemic therapies and antimalarial medications. 4 Low-dose topical steroids are optimal to reduce superficial inflammation while mitigating systemic side effects in SCLE. To prevent further cutaneous disfiguration and to reduce inflammation that promotes progression to squamous cell carcinoma, stronger immunosuppressants may be utilized for DLE. 5 Limitations include retrospective nature and limited sample size. In conclusion, we present clinically useful distinctions in SCLE and DLE patient disease profiles to elucidate diagnostic and therapeutic differences.
Supplemental Material
sj-docx-1-cms-10.1177_12034754241266144 – Supplemental material for Distinct Patient Disease Profiles in Discoid Lupus Erythematosus and Subacute Lupus Erythematosus: A Retrospective Study
Supplemental material, sj-docx-1-cms-10.1177_12034754241266144 for Distinct Patient Disease Profiles in Discoid Lupus Erythematosus and Subacute Lupus Erythematosus: A Retrospective Study by Nilesh Kodali, Ruchi Biswas, Rohan Singh, Shivkar Amara and Robert A. Schwartz in Journal of Cutaneous Medicine and Surgery
Footnotes
Data Availability
Data are not publicly available and can be accessed through accreditation with the All of Us research database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.