
Abstract
Objective:
To evaluate efficacy and safety of abrocitinib and dupilumab in the treatment of moderate-to-severe atopic dermatitis (AD).
Methods:
A retrospective analysis of 104 patients with moderate-to-severe AD (January-June 2023) was conducted. Patients received either oral abrocitinib 200 mg/day (n = 51) or subcutaneous dupilumab 300 mg every 2 weeks (n = 53, baseline load 600 mg) for 24 weeks.
Results:
At 4, 8, and 12 weeks posttreatment, patients in the abrocitinib group exhibited significantly lower Eczema Area and Severity Index (EASI) scores compared to the dupilumab group (P < .05). Additionally, patients in the abrocitinib group demonstrated significantly lower Numeric Rating Scale for Pruritus (P-NRS) scores at 4, 8, 12, 16, and 24 weeks posttreatment compared to the dupilumab group (P < .05). Furthermore, patients in the abrocitinib group showed significantly lower Dermatology Life Quality Index (DLQI) scores at 4, 8, 12, and 16 weeks posttreatment compared to the dupilumab group (P < .05). Compared with dupilumab group, EASI, P-NRS and DLQI levels in abrocitinib group were more significantly decreased. The incidence of conjunctivitis in dupilumab group was significantly higher than that in abrocitinib group (P < .05). The incidence of nausea in abrocitinib group was significantly higher than that in dupilumab group (P < .05).
Conclusion:
Both abrocitinib and dupilumab can significantly relieve pruritus and improve quality of life in patients with moderate-to-severe AD at 24 weeks after treatment, but abrocitinib is more effective in relieving pruritus. Both abrocitinib and dupilumab have high safety, but require attention for gastrointestinal symptoms and conjunctivitis, respectively.
Introduction
Atopic dermatitis (AD) is a prevalent chronic inflammatory skin condition that significantly impacts patients’ quality of life. 1 In China, AD ranks first in terms of socioeconomic burden among all dermatological diseases, highlighting its substantial public health importance. 2 For patients with moderate-to-severe AD who do not respond adequately to topical treatments, systemic therapy remains the most effective approach. 3
Traditional systemic medications, such as cyclosporine and corticosteroids, have been used for years to manage AD. These medications can offer some efficacy in controlling the disease; however, they are associated with significant side effects, which necessitate cautious use and monitoring. 4 The search for safer and more effective systemic therapies has led to the development of novel biologic and small-molecule treatments.
Dupilumab, a subcutaneously administered monoclonal antibody, targets the interleukin (IL)-4 receptor subunit alpha, thereby inhibiting IL-4 and IL-13 signalling pathways. These pathways play crucial roles in the pathogenesis of AD. Clinical studies have demonstrated that dupilumab significantly alleviates AD symptoms and improves patients’ quality of life.5,6 Its ability to modulate the immune response by blocking key cytokines has made it a cornerstone in the treatment of moderate-to-severe AD.
In addition to biologics such as dupilumab, small-molecule inhibitors have also shown promise in the treatment of AD. Abrocitinib, a Janus kinase-1 (JAK1) inhibitor, reversibly and selectively inhibits JAK1, a critical intracellular enzyme for the signal transduction of multiple cytokines implicated in the pathogenesis of AD, including IL-4, IL-13, IL-31, and thymic stromal lymphopoietin. 7 By blocking the JAK1-STAT (Signal Transducer and Activator of Transcription) pathway, abrocitinib dampens the inflammatory cascade and reduces the neuronal sensitization that drives pruritus. For instance, the pruritogenic cytokine IL-31 exerts its effects directly through receptors that signal via JAK1. Therefore, abrocitinib’s inhibition of this pathway is considered a key mechanism for its rapid and effective alleviation of itch sensation. Current research findings suggest that abrocitinib demonstrates significant efficacy in mitigating the symptoms of AD and substantially improving patients’ quality of life. 8
Despite the promising results of both dupilumab and abrocitinib in international studies, there remains a notable gap in the literature regarding their use in Chinese AD patients. No clinical studies conducted in China have thus far evaluated the therapeutic efficacy and safety profiles of both abrocitinib and dupilumab in this population. This gap underscores the need for localized research to understand how these treatments perform in different demographic and genetic backgrounds.
In light of paucity of data in the patient population in China, our retrospective study aims to compare the efficacy and safety of 2 novel drugs, abrocitinib and dupilumab, in the treatment of moderate-to-severe AD. It quantitatively evaluates their specific effects on alleviating skin symptoms, relieving pruritus, and improving quality of life from multiple perspectives. The findings are intended to provide objective and scientific evidence for clinicians to make precise medication decisions for patients with moderate-to-severe AD, and are of great clinical significance and value. By providing valuable empirical data, our study seeks to inform and optimize the development of comprehensive treatment strategies tailored to the specific needs of these patients. We hope that our findings will contribute to better clinical decision-making and improved patient outcomes in the management of AD.
Materials and Methods
Participants
This study is a retrospective analysis. The electronic medical records of 104 moderate-to-severe AD patients who visited our hospital between January and June 2023 were reviewed. Inclusion criteria were: age between 18 and 60 years; clinical diagnosis of AD with a disease duration of at least 6 months; systemic treatment for AD within the past year, or at least 4 weeks of continuous topical treatment for AD within the past 6 months with unsatisfactory results; and moderate-to-severe AD defined by an Eczema Area and Severity Index (EASI) score ≥ 16.9,10 The diagnosis of AD was based on the “Chinese AD Diagnostic Criteria” proposed by Zhang Jianzhong. 11 Exclusion criteria included previous use of JAK inhibitors or IL-4/IL-13 inhibitors; history of hematological diseases or malignancies; incomplete medical records; and nonadherence to prescribed medications during treatment.
Data Collection
General information was collected, including age, gender, duration of AD, affected body surface area, history of allergic rhinitis, and asthma. EASI (the maximum score of EASI is 72 points), Dermatology Life Quality Index (DLQI, the maximum value of DLQI is 30 points), and Numeric Rating Scale for Pruritus (P-NRS, ranging from 0 for “no itch” to 10 for “worst imaginable itch”) which refers to average pruritus were collected at 0, 4, 8, 12, 16, and 24 weeks. Serum total Immunoglobulin E (IgE) levels and eosinophil counts were tested at 0, 8, 16, and 24 weeks. Treatment-related adverse events were recorded, including conjunctivitis, nausea, headache, acne or folliculitis, and local injection site reactions (itching, erythema, swelling, pain) in dupilumab group.
Medication Administration
Patients were assigned to the abrocitinib or dupilumab groups based on shared decision-making between clinicians and patients, considering factors such as treatment accessibility, patient preference, and clinical suitability (eg, contraindications, comorbidities). Randomization was not applied in this retrospective study. Abrocitinib group patients received oral abrocitinib 200 mg/day for a 24-week treatment period. The 200 mg dose was selected based on prior clinical trials demonstrating its efficacy and safety profile in moderate-to-severe AD populations. 12 Dupilumab group patients received subcutaneous injections of dupilumab 300 mg every 2 weeks (with a baseline loading dose of 600 mg). The treatment period was 24 weeks. During treatment, patients were allowed to use moisturizers, topical moderate-potency corticosteroids, and topical calcineurin inhibitors.
Statistical Analysis
Data were analyzed using SPSS software (version 29.0). Normality of continuous data was tested using the Kolmogorov–Smirnov test. Data conforming to a normal distribution were analyzed using independent sample t-tests or one-way ANOVA and expressed as mean ± standard deviation (
Results
Baseline Characteristics
This study reviewed the medical records of 104 patients, with 51 in the abrocitinib group and 53 in the dupilumab group. There were no statistically significant differences in age, gender, disease duration, affected body surface area, baseline EASI, baseline P-NRS, baseline DLQI, prevalence of allergic rhinitis, or allergic asthma between the 2 groups (P > .05). The incidence of comorbid cutaneous viral infections (eg, herpes simplex virus) at baseline was also comparable between the groups. Furthermore, the proportion of patients who had received a varicella-zoster virus vaccine prior to initiating treatment was not significantly different. The baseline characteristics of the patients are shown in Table 1.
Comparison of Baseline Characteristics between the 2 Groups (
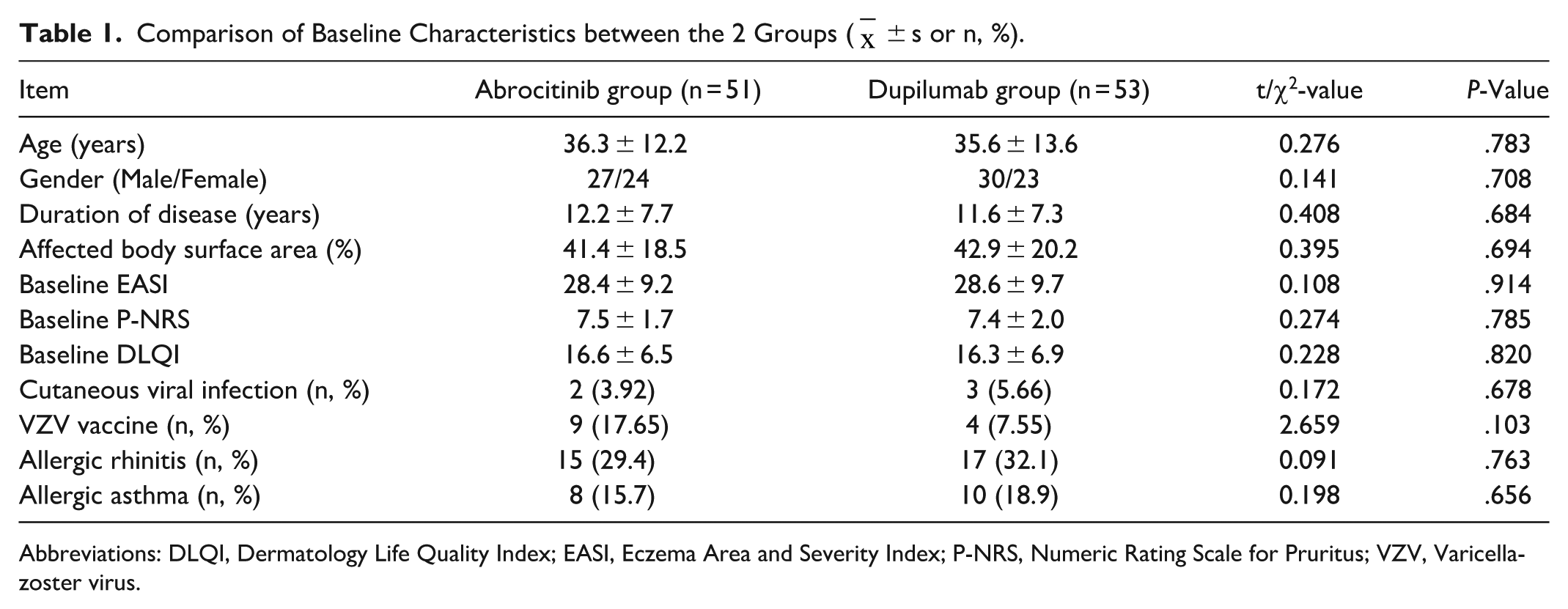
Abbreviations: DLQI, Dermatology Life Quality Index; EASI, Eczema Area and Severity Index; P-NRS, Numeric Rating Scale for Pruritus; VZV, Varicella-zoster virus.
Clinical Efficacy Indicators
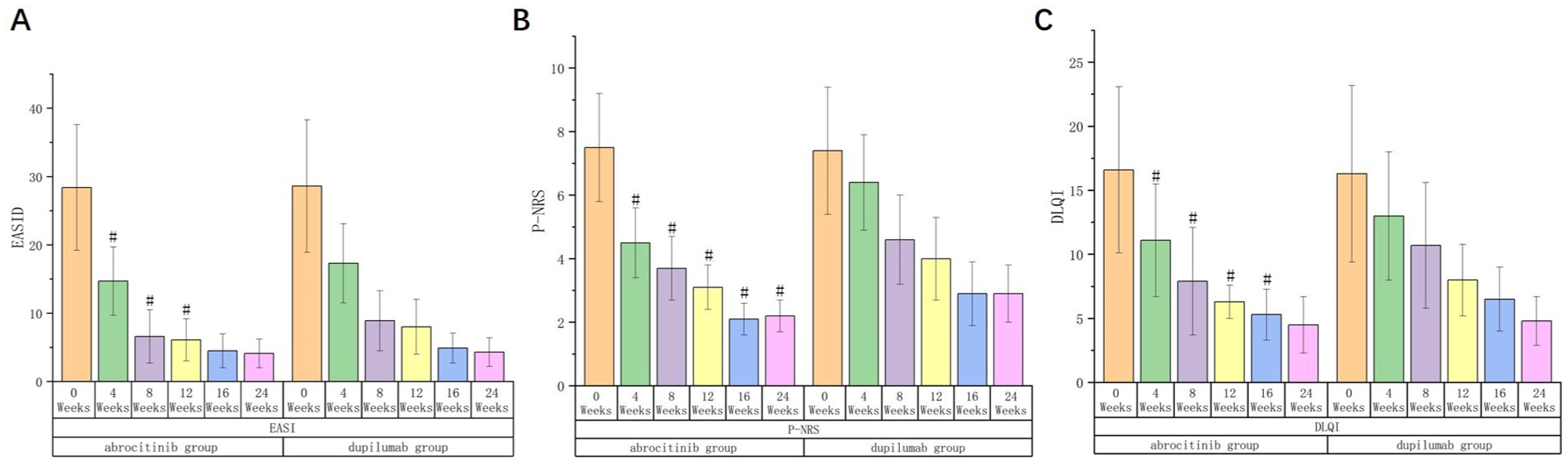
As the treatment period extended, the EASI, P-NRS, and DLQI in both groups showed a gradual decreasing trend. At the 4, 8, and 12 weeks posttreatment intervals, the EASI scores in abrocitinib group exhibited a notably lower magnitude compared to those in dupilumab group, with these differences being statistically significant (P < .05). Similarly, the P-NRS scores in abrocitinib group were significantly reduced relative to dupilumab group at the 4, 8, 12, 16, and 24 weeks posttreatment assessments, with all observed differences achieving statistical significance (P < .05). Additionally, the DLQI scores in abrocitinib group showed a marked reduction compared to dupilumab group at the 4, 8, 12, and 16 weeks posttreatment evaluations, with these reductions also being statistically significant (P < .05). The comparison of clinical efficacy indicators at each time point posttreatment between the 2 groups is shown in Table 2. The trend of changes in clinical efficacy indicators at each time point posttreatment in both groups is illustrated in Figure 1.
Comparison of Clinical Efficacy Indicators at Various Time Points After Treatment in Both Groups (
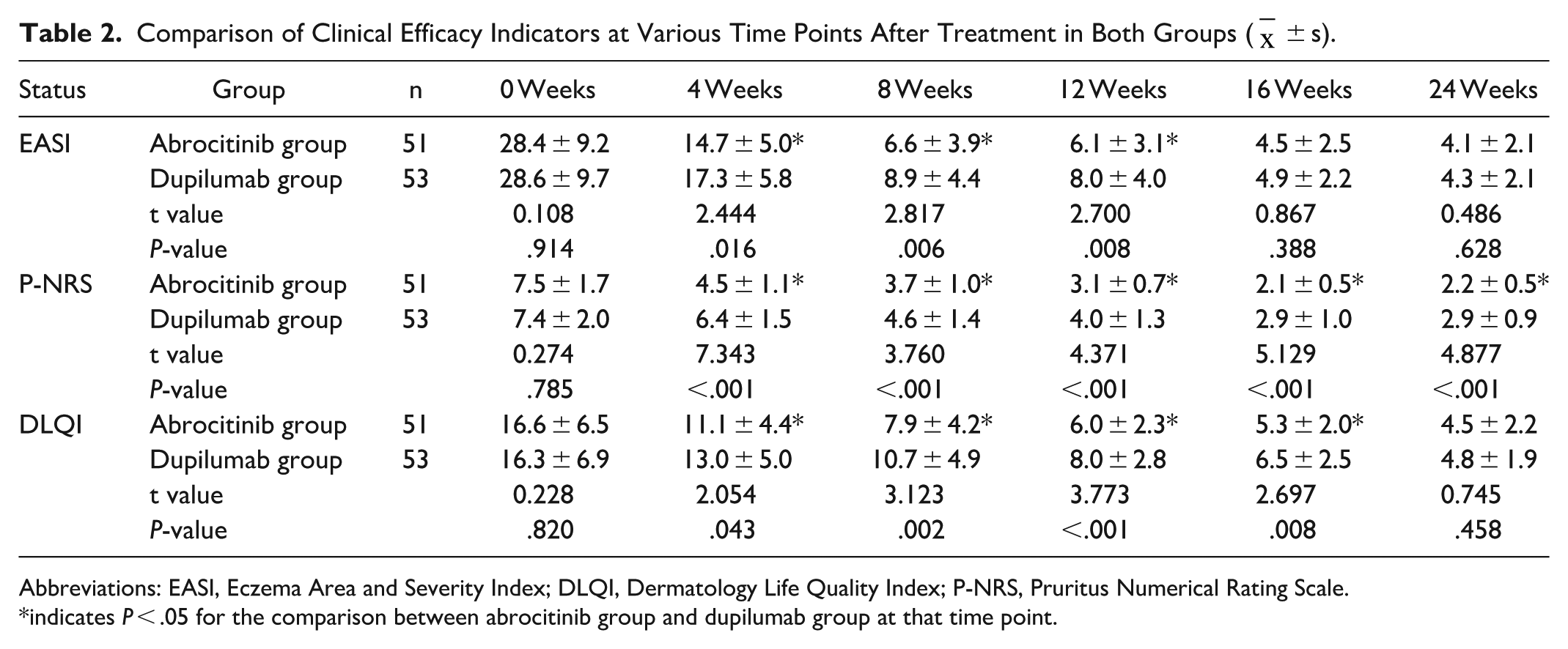
Abbreviations: EASI, Eczema Area and Severity Index; DLQI, Dermatology Life Quality Index; P-NRS, Pruritus Numerical Rating Scale.
indicates P < .05 for the comparison between abrocitinib group and dupilumab group at that time point.
Changes in Inflammatory Biomarkers
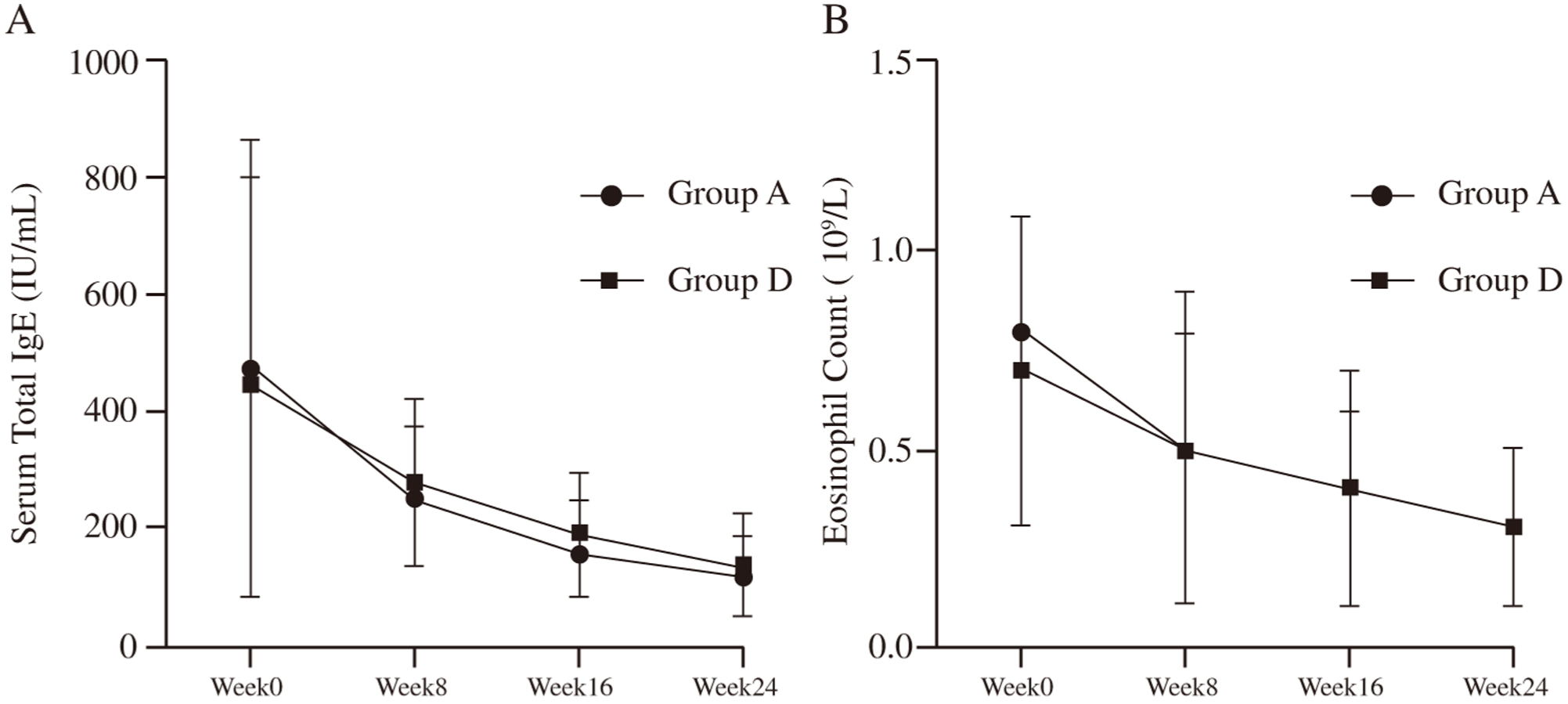
We further evaluated the changes in key inflammatory biomarkers, including serum total IgE and eosinophil counts (Figure 2). In both the abrocitinib and dupilumab groups, a clear downward trend was observed for both serum total IgE levels from baseline to week 24 (Figure 2A). A similar reduction was also seen in eosinophil counts over the same period (Figure 2B). Despite these improvements within each group, a comparative analysis revealed no statistically significant differences between the abrocitinib and dupilumab groups at weeks 8, 16, or 24 for either biomarker (P > .05).
Safety Indicators
The incidence of conjunctivitis in dupilumab group was significantly higher than in abrocitinib group (P < .05). Among the 10 patients in dupilumab group who developed conjunctivitis, 6 had conjunctival hyperemia and 4 were sensitive to light. All cases were cured after consultation with an ophthalmologist. The incidence of nausea in abrocitinib group was notably higher compared to dupilumab group, with a statistically significant difference observed (P < .05). Conversely, there were no statistically significant differences detected in the incidence of headache or acne/folliculitis between the 2 groups (P > .05). In dupilumab group, 10 patients experienced local injection site reactions, with an incidence rate of approximately 18.9%, all of which were mild and resolved without special treatment. The comparison of treatment-related adverse reactions between the 2 groups is laid out in Table 3.
Comparison of Directly Treatment-Related Adverse Reactions between the 2 Groups.

Discussion
Simpson et al 13 demonstrated that dupilumab improved pruritus symptoms, anxiety, and depression in AD patients who had inadequate response to topical treatments within 16 weeks. A recent meta-analysis summarized the effects of dupilumab on AD, showing improvements in clinical symptoms and quality of life in both adult and pediatric/adolescent patients. 14 Abrocitinib is a selective JAK1 inhibitor that blocks the Adenosine Triphosphate (ATP) binding site to selectively inhibit JAK1, reducing downstream gene transcription and persistent inflammatory cytokines, thereby decreasing the production of key factors and other markers involved in AD progression. 15 Another study by Simpson et al 16 evaluated the efficacy of different doses of abrocitinib (200 and 100 mg/day) in treating moderate-to-severe AD. The results showed that both doses significantly reduced the impact of AD symptoms on quality of life, with the 200 mg/day dose being more effective than the 100 mg/day dose.
The EASI is a physician-based assessment tool commonly used to evaluate the severity of AD. 1 In this study, patients treated with abrocitinib had significantly lower EASI scores within 12 weeks compared to those treated with subcutaneous dupilumab. However, at 16 and 24 weeks posttreatment, there were no statistically significant differences in EASI between the 2 groups. This suggests that abrocitinib is more effective than dupilumab in reducing lesion area and severity within 12 weeks but that dupilumab achieves similar therapeutic effects after prolonged treatment. This observation may be attributed to the distinct mechanisms of action of abrocitinib and dupilumab. Abrocitinib, a JAK1 inhibitor, alleviates inflammatory responses by suppressing the JAK pathway, thereby reducing cytokine signalling, cytokine-induced gene expression, and cellular activation. In contrast, dupilumab, a humanized monoclonal antibody, binds to the α subunit of the IL-4 receptor, inhibiting downstream signalling pathways of IL-4 and IL-13, which mitigates cutaneous inflammation. Although these agents target different molecular pathways, both ultimately suppress inflammatory cascades and improve clinical manifestations of AD. Drucker et al 17 recently conducted a network meta-analysis comparing the effects of dupilumab and abrocitinib on AD, finding that at 16 weeks, abrocitinib 200 mg daily was associated with slightly greater reductions in EASI compared to dupilumab, although our real-world data did not show a statistically significant difference at this time point. This discrepancy may reflect differences between the controlled setting of randomized trials and the heterogeneity of real-world clinical practice. Persistent severe pruritus caused by AD significantly impacts patients’ daily lives, sometimes leading to sleep disturbances, anxiety, and other complications. 18 The P-NRS and DLQI are patient-based assessments used to evaluate pruritus severity and quality of life, respectively. Based on our study, patients treated with abrocitinib exerted notably lower P-NRS scores within 24 weeks compared to those treated with subcutaneous dupilumab, indicating that abrocitinib is superior to dupilumab in relieving AD-related pruritus. Shi et al 19 depicted that switching AD patients who had inadequate response to subcutaneous dupilumab to oral abrocitinib significantly reduced P-NRS scores. These findings imply that abrocitinib may be more efficacious than dupilumab in alleviating pruritus among AD patients.
In terms of safety, this study revealed a higher incidence of nausea associated with abrocitinib, which notably diminished when the medication was administered after meals. Common adverse reactions to dupilumab, such as conjunctivitis, were observed to be mild across all patients in the study. However, it is crucial to note that recent studies have indicated an elevated risk of cardiogenic death among rheumatoid arthritis patients treated with tofacitinib, another JAK inhibitor, leading to class-wide warnings for JAK inhibitors like abrocitinib. 20 Consequently, when utilizing abrocitinib and dupilumab in clinical settings, it is imperative to thoroughly evaluate the patient’s baseline health status to preempt serious adverse events.
This study is not without its limitations. First, as a retrospective analysis, the nonrandomized assignment of treatments may introduce selection bias, potentially influencing outcome comparisons between groups. Second, being a retrospective study, it may be susceptible to measurement bias, which could impact the accuracy of the results. Third, serum total IgE levels were assessed every 8 weeks during outpatient follow-ups, thereby limiting the ability to precisely track the dynamic changes in these levels over time. Fourth, given the relatively recent availability of abrocitinib in China, the sample size in this study was comparatively small, which precluded the use of the proportion of patients achieving at least 90% improvement in EASI (EASI-90) as an outcome measure. Future research would benefit from prospective randomized controlled trials to further substantiate the therapeutic efficacy and safety profiles of abrocitinib and dupilumab in patients with moderate-to-severe AD.
In conclusion, both abrocitinib and dupilumab demonstrate significant alleviation of pruritus and enhance the quality of life in patients with moderate-to-severe AD after treatment. However, abrocitinib appears to be more effective in relieving pruritus at 24 week compared to dupilumab. While both medications exhibit high safety profiles, careful monitoring of gastrointestinal symptoms with abrocitinib and conjunctivitis with dupilumab is warranted.
Footnotes
Authors’ Contributions
X.W. contributed to the conception and design of the study; X.H. and M.Z. performed the experiments; S.W., X.H. and M.Z. collected and analyzed data; X.H. and M.Z. wrote the manuscript; X.W. revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study protocol was in accordance with the Declaration of Helsinki of the World Medical Association. This study was approved by the Ethical Research Committee of Renmin Hospital, Hubei University of Medicine. Prior to participation in the study, patients and their guardians provided informed consent, demonstrating their willingness to be included in the research.
Availability of Data and Materials
The data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.