
Abstract
Background:
Hidradenitis suppurativa (HS) is a chronic and debilitating skin disorder. Secukinumab, a biologic agent targeting interleukin-17, is a new therapeutic option for HS. However, data regarding its long-term outcomes are scarce.
Objective:
To evaluate the long-term effectiveness, safety, and predictors of response to secukinumab in a real-world cohort of patients with moderate-to-severe HS.
Methods:
Multicentre retrospective cohort study across 12 Italian tertiary referral hospitals. The primary effectiveness outcomes were the proportion of patients achieving Hidradenitis Suppurativa Clinical Response (HiSCR) and a 55% reduction in the International Hidradenitis Suppurativa Severity Score System (IHS4-55) at any time point.
Results:
A total of 77 patients (53% female; median age 38 years, interquartile range: 27-50) met the inclusion criteria. At week 52, 36.2% of patients achieved HiSCR and 55.6% achieved IHS4-55. The mean reduction from baseline to week 52 was 50.8% for skin pain Numeric Rating Scale and 55.2% for Dermatology Life Quality Index. Agreement between IHS4-55 and HiSCR was 76.6% (Cohen’s kappa 0.5255; 95% CI: 0.4307-0.6202, P < .0001). Patients in Hurley stage 3 had a significantly lower hazard ratio (HR) of achieving IHS4-55 than those in Hurley stage 2 (HR 0.52; 95% CI: 0.31-0.89, P = .017), which persisted in the multivariable model (HR 0.56; 95% CI: 0.31-0.99, P = .044). No new safety concerns were identified.
Conclusions:
This study suggests that secukinumab provides clinically meaningful long-term outcomes in HS management, even in bio-experienced patients.
Introduction
Hidradenitis suppurativa (HS) is a chronic, debilitating inflammatory disorder of the terminal hair follicle. It typically manifests with deep-seated inflammatory nodules, abscesses, and tunnels in apocrine gland-bearing areas. 1 Current challenges include significant diagnostic delay (7-12 years from the first symptoms until correct diagnosis) and a remarkable impact on patients’ quality of life.2,3 The pathogenesis of HS is multifactorial, involving genetic and epigenetic factors as well as environmental, hormonal, microbiological, and immunological components.1,4 In recent years, the interleukin-17 (IL-17) pathway has been described as a pivotal axis in HS development by driving the recruitment and accumulation of neutrophils and other inflammatory cells into the skin.5-7 Elevated IL-17A levels have been observed in both serum and lesional skin of patients with HS, with notably high T-helper 17 cells and IL-17-producing cells in active lesions. 8 This evidence has led to the exploration of biologic agents targeting IL-17 for HS management.6,8 In this context, secukinumab, a fully human monoclonal antibody that selectively binds to and neutralizes IL-17A, has recently been investigated. 9 In 2023, the SUNSHINE and SUNRISE trials demonstrated the promising efficacy of this agent in treating moderate-to-severe HS, leading to secukinumab approval in Europe. 10 The primary endpoint, defined as the proportion of patients with Hidradenitis Suppurativa Clinical Response (HiSCR) at the 16th week, was met by 45% to 46% of patients in both trials. Moreover, secukinumab effectively improved patients’ health-related quality of life measures, with sustained benefits up to week 52 across all dosing regimens. However, only a few reports explored the real-world effectiveness and safety of secukinumab so far, and data regarding its long-term outcomes remain scarce.5,8,11-19 This study aimed to address this knowledge gap by investigating long-term outcomes and clinical predictors of response among patients diagnosed with moderate-to-severe HS and undergoing secukinumab in a real-world setting.
Materials and Methods
Study Design and Population
We conducted a multicentre, retrospective cohort study across 12 Italian tertiary referral hospitals. Patients were eligible if aged ≥18 years and diagnosed with moderate-to-severe HS (defined as a total of 5 or more inflammatory lesions affecting at least 2 distinct anatomical areas). 10 All participants had comprehensive medical records and were either treated with secukinumab for concomitant psoriasis or with off-label for HS, between April 2018 and April 2024. Patients that had 20 or more fistulae at baseline and with a follow-up period shorter than 12 weeks were excluded. Identification of eligible cases was achieved through the retrospective review of both electronic health records and specific datasets from the participating sites. The study protocol was approved by the institutional review board (no 0055827), and the study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cohort studies. 20
Data Collection
Data including demographic and medical history were collected at baseline, while disease severity and treatment outcomes were assessed at all scheduled time points (baseline, 5, 16, 28, 52 weeks, and then every 6 months for a total duration of 3 years after treatment initiation). HS phenotypes were considered according to the van der Zee and Jemec classification. 21 The latter one distinguishes 6 different clinical presentations, namely, the regular, frictional furuncle, scarring folliculitis, conglobata, syndromic, and ectopic type. Safety was monitored through laboratory tests, physical examinations, and recording treatment-emergent adverse events (TEAEs). Ultrasound assessments were performed when there was uncertainty in evaluating subclinical lesions. Patients were stratified according to Hurley stage, a clinical staging system subdivided into stage 1 (single or multiple abscesses without sinus tract formation or scarring), stage 2 (recurrent abscesses with 1 or more sinus tracts and scarring widely separated by normal skin), and stage 3 (diffuse involvement with multiple sinus tracts and no intervening normal skin). 22 Skin pain Numeric Rating Scale (NRS), ranging from 0 (no skin pain) to 10 points (skin pain as bad as you can imagine), was used to evaluate skin pain intensity during the previous 24 hours before the visit. 10 The impact on quality of life was evaluated by means of the Dermatology Life Quality Index (DLQI). 23
Outcomes
The primary outcomes were (i) the proportion of patients who achieved the clinical response HiSCR at the 52nd week (defined as a ≥50% reduction in inflammatory lesion count and no increase in abscesses or fistulas compared to baseline), 24 (ii) the proportion of patients who achieved International Hidradenitis Suppurativa Severity Score System (IHS4-55) at the 52ndweek (defined as a ≥55% reduction in the IHS4 score, the latter calculated as the number of nodules multiplied by 1, plus the number of abscesses multiplied by 2, plus the number of draining tunnels multiplied by 4. Scores are categorized as mild disease for a total score ≤3, moderate disease for scores of 4 to 10, and severe disease for scores ≥11). 25 Secondary outcomes included the following: (i) the proportion of patients who achieved AN50 at the 52nd week (achievement of a 50% reduction in abscess and nodule count), (ii) the proportion of patients who achieved NRS30 at the 52nd week (defined as a ≥30% reduction and ≥2-unit reduction in skin pain on a continuous NRS from baseline via the patient global assessment of skin pain—at worst, in patients with a baseline NRS ≥3), 10 (iii) mean percent changes from baseline in skin pain NRS and DLQI, (iv) incidence of TEAEs, and (v) treatment outcomes beyond 52 weeks of secukinumab for all scores listed.
Statistical Analysis
Categorical variables were summarized using frequencies and percentages, while quantitative variables were described using means, medians, standard deviations, and interquartile ranges (IQRs). Descriptive statistics were presented by response group, with responders defined as those who achieved at least one of the scores HiSCR and HIS-55, and nonresponders defined as those who did not achieve either. Differences between groups were evaluated using chi-squared tests for categorical variables and Kruskal-Wallis tests for continuous numeric variables. Exploratory analyses were conducted to assess the treatment response as measured by the following scores: HiSCR, IHS4-55, NRS30, and AN50. For each score and each time point, the frequency of responders was calculated. A Fine and Gray model was then utilized to assess the impact of the following variables on the time-to-response according to each score: age, sex, smoking status, body mass index (BMI), duration of HS, bio-naïve to secukinumab, and Hurley staging at baseline. All variables were assessed both individually and in a multivariable model. Finally, Cohen’s kappa coefficient was employed to evaluate the level of agreement between HiSCR and IHS4-55 scores across the duration of the study. All tests were 2-sided, and a P < .05 was considered statistically significant. All analyses were performed using SAS® software, version 9.4 (SAS Institute, Inc, Cary, NC, USA).
Results
Patients’ Characteristics
A total of 77 Caucasian patients were included in the study, with a median age of 38 years (IQR: 27-50). The cohort comprised 53% females (n = 41) and 47% males (n = 36). Smoking status distribution showed 33.8% nonsmokers (n = 26), 61% smokers (n = 47), and 5.2% former smokers (n = 4). The median BMI was 24.8 (IQR: 21.0-30.5). The Hurley stage distribution at the beginning of treatment was 44% in stage 2 (n = 34), and 56% in stage 3 (n = 43). The median duration of HS was 11 years (IQR: 5-18), with 7.8% of patients (n = 6) being bio-naïve. As for the treatment regimen, all the participants underwent 5 weekly subcutaneous injections of 300 mg secukinumab, followed by a maintenance phase of 300 mg subcutaneously every 4 weeks (q4w).
Outcomes
The proportion of patients achieving clinical response increased from weeks 5 to 52 across all scores: from 30.2% to 36.2% for HiSCR, from 31.1% to 55.6% for IHS4-55, from 35.8% to 81% for NRS30, and from 36.5% to 46.8% for AN50 (Figure 1). There were no significant differences in baseline characteristics between different response classes (Supplementary Table 1). The overall agreement between IHS4-55 and HiSCR scoring systems was 76.6% and Cohen’s kappa coefficient was 0.5255 (95% CI: 0.4307-0.6202, P < .0001; Supplementary Table 2). Throughout the study period, the median time to first clinical response was 4 months (IQR: 1.25-4) for HiSCR, 4 months (IQR: 1.25-7) for IHS4-55, 4 months (IQR: 1.25-5.5) for NRS30, and 1.25 months (IQR: 1.25-4) for AN50. At the end of the 52 week treatment period, a total of 6 (7.8%) patients had discontinued secukinumab due to lack of effectiveness, 5 (6.5%) due to the loss of response, 6 (7.8%) were lost to follow-up, and 1 patient (1.3%) due to AE. Additionally, 14 patients had not yet reached the 52 week follow-up.
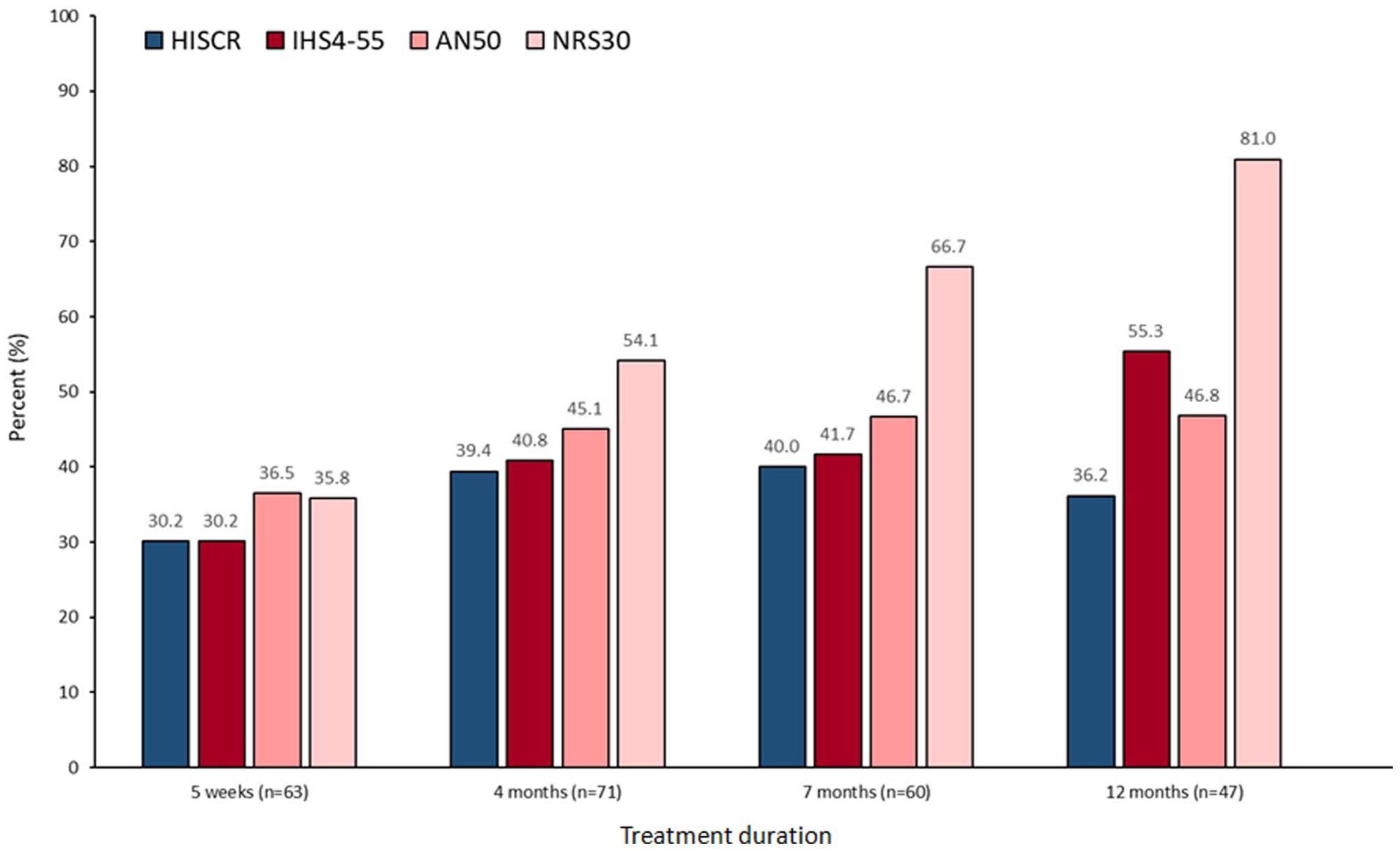
Bar graph showing the percentage of patients achieving HiSCR, IHS4-55, AN50, and NRS 30 at the week 5 and at months 4, 7, and 12. HiSCR, Hidradenitis Suppurativa Clinical Response; IHS4, Hidradenitis Suppurativa Severity Score System; IHS4-55, 55% reduction in the IHS4 score; AN50, achievement of a 50% reduction in abscess and nodule count; NRS30, ≥30% reduction and ≥2-unit reduction in skin pain on a continuous NRS from baseline via the patient global assessment of skin pain—at worst, in patients with a baseline NRS ≥3; NRS, Numeric Rating Scale.
Long-Term and Safety Outcomes
From week 52 to the end of the study, clinical outcomes and quality of life assessments were conducted for 47 patients, who were still undergoing secukinumab. Of these, 11 patients discontinued the treatment, while the remaining patients were still receiving secukinumab at the end of the study (Supplementary Tables 3 and 4). The reasons for discontinuation included lack of effectiveness (n = 4; 5.2%), loss of response (n = 4; 5.2%), discontinuation based on patient decision (n = 1; 1.3%), and introduction of belimumab for concomitant systemic lupus erythematosus in 1 patient (1.3%). Throughout the study period, only 1 AE was observed in terms of paradoxical psoriasis following the initiation of secukinumab, which resulted in the discontinuation of the medication.
Predictors of Treatment Response
In the analysis of predictors for treatment response, BMI emerged as a significant predictor of AN50 and NRS30 response in both univariable [hazard ratio (HR): 1.04, 95% CI: 1.00-1.08, P = .040 and HR: 0.93, 95% CI: 0.89-0.97, P = .002] and multivariable (HR: 1.04, 95% CI: 1.00-1.09, P = .028 and HR: 0.94, 95% CI: 0.90-0.99, P = .019) models adjusted for age, duration of HS, and Hurley staging. HS duration also showed a significant predictive value for NRS30 response, with a HR of 1.04 (95% CI: 1.01-1.06, P = .002) in the univariable analysis and 1.05 (95% CI: 1.01-1.09, P = .008) in the multivariable one. As for IHS4-55, patients with Hurley stage 3 had a significantly lower hazard of achieving a response than those in stage 2, as indicated by a HR of 0.52 (95% CI: 0.31-0.89, P = .017) in the univariable model. This association persisted in the multivariable model, with a HR of 0.56 (95% CI: 0.31-0.99, P = .044). Finally, none of the baseline independent variables significantly influenced the achievement of HiSCR in either univariable or multivariable analysis (Supplementary Table 5).
Discussion
Patients with HS require long-term management and regular follow-up due to the highly recalcitrant nature of the disease. Current HS management includes topical therapies, systemic antibiotics, retinoids, corticosteroids (mostly intralesional), and various surgical procedures, which may demonstrate limited efficacy in moderate-to-severe HS. 1 The tumour necrosis factor-α antagonist adalimumab was the first Food and Drug Administration and European Medicines Agency approved biologic for HS, though its efficacy varies, with clinical response rates of ~50% in phase III trials (41.8% in PIONEER I and 58.9% in PIONEER II). 26 Moreover, patients undergoing adalimumab may experience secondary lack of efficacy and paradoxical reactions, thus underscoring the need for other therapeutic options.27,28
The primary aim of our study was to address the lack of knowledge regarding the long-term outcomes of secukinumab in treating moderate-to-severe HS. Our findings indicate that a relevant subset of patients with HS treated with secukinumab experienced a sustained clinical response over 52 weeks of treatment. Data from the SUNSHINE and SUNRISE trials have previously shown that patients with HS treated with secukinumab at different dosing intervals achieved HiSCR rates ranging from 42% to 46% at week 52. 10 In our sample, HiSCR achievement was slightly lower than in the SUNSHINE and SUNRISE trials 10 and than other real-world studies.5,8,11-19,29-31 By contrast, the proportion of patients in our cohort achieving IHS4-55 at week 52 (55.6%) was consistent with the pooled data from a post hoc analysis of SUNSHINE and SUNRISE for secukinumab q4w (57.6%). 32 Nevertheless, such comparisons must be interpreted with caution, since differences in outcomes may arise from heterogeneity across several factors, including study design, enrolled populations, prior biologic exposure, and concomitant treatments.
In this study, inferential analyses were exclusively conducted on patients with HS receiving secukinumab up to week 52. This approach was adopted to maintain a sufficiently large sample, as the poor representation of data beyond week 52 in our cohort precluded reliable inferential conclusions. Nonetheless, these patients were descriptively evaluated to provide a long-term assessment of secukinumab at time points where real-world evidence is lacking. To improve the accuracy of drug effectiveness validation, we evaluated clinical response at each visit using both HiSCR and IHS4-55. The IHS4-55 score addresses some of the drawbacks of HiSCR by dynamically including draining tunnels and allowing the analysis of HS patients with an AN count below 3 or more than 20 draining fistulae. 25 Comparing the IHS4-55 and HiSCR scoring systems, a moderate statistically significant agreement beyond chance was found. These results align with the post hoc analyses of SUNSHINE and SUNRISE trials, which showed a strong concordance between IHS4-55 and HiSCR responses at weeks 16 and 52 (≥85.7% in pooled analysis and by trial) in all treatment arms. 32 The difference between the 2 scores may highlight the key role of IL-17 in dermal tunnels formation, explaining the superior response to secukinumab in patients with this type of lesions, better captured in IHS4-55 score. Similar effects of IL-17 signalling antagonists on HS tunnels have also been observed with brodalumab, a human monoclonal IgG2 antibody that binds with high affinity to human IL-17 receptor A.31-33 In previous trials, 20% to 25% of participants had been treated with adalimumab before starting secukinumab, highlighting the need to evaluate treatment outcomes in this underrepresented subset of patients.10,34 Our cohort is largely composed of individuals previously exposed to biologic agents, with only 7.8% being bio-naïve, providing additional evidence on secukinumab effectiveness in managing HS bio-experienced patients. The impact of Hurley stage on IHS4-55 appeared to be the strongest and most clinically significant, whereas other statistically significant HRs were closer to 1, suggesting a weaker or negligible effect of the associated variables on the outcome. The difference in predictive factors between HiSCR and IHS4-55 may be attributed to the distinct aspects of disease severity they assess. Additionally, the relatively small sample size may have contributed to variability in treatment response. Increasing evidence supports IL-17A and IL-17F as key drivers of HS pathogenesis. IL-17-producing CD4+ T cells are enriched more than 40-fold in HS-involved skin compared with those in normal skin. 35 Furthermore, upregulation of IL-17A and IL-17F mRNA in lesional tissue and elevated IL-17 serum levels in patients with HS have been extensively reported.36 -38 A recent study validated tape strips as a minimally invasive method for identifying cutaneous biomarkers in HS, detecting an upregulation of known HS biomarkers such as IL-17A in both non-lesional and lesional skin. Interestingly, high variability in IL-17A expression among patients with HS was also detected. 39 These findings may partially explain the variability in clinical response to secukinumab observed in our cohort. Secukinumab was well-tolerated, with no new safety concerns observed, aligning with safety profiles reported in long-term studies of patients under treatment for other skin conditions such as psoriasis and psoriatic arthritis. 40
Limitations
Study limitations include its retrospective design with heterogeneous follow-up intervals. The sample size was relatively small, particularly beyond 1 year of therapy where long-term outcomes may have also been subject to survivorship bias. Selection bias may be present, as patients were enrolled from tertiary referral centres and were almost exclusively Caucasian, which could limit generalizability. In addition, unmeasured confounders and missing data were not fully accounted for and may have influenced treatment outcomes. Nonetheless, this study represents one of the largest real-world cohorts of patients with HS treated with secukinumab and provides some of the longest follow-up data available to date.
Conclusions
This cohort of patients undergoing secukinumab adds to the existing evidence concerning the effectiveness and safety of targeting IL-17 axis in HS, even in bio-experienced patients. Long-term treatment with secukinumab demonstrated clinically meaningful outcomes in the management of moderate-to-severe HS. Further research focusing on the high variability of observed clinical responses is warranted, aiming to explore the underlying mechanisms driving these differences and develop tailored treatment approaches for each patient.
Supplemental Material
sj-docx-1-cms-10.1177_12034754261418237 – Supplemental material for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study
Supplemental material, sj-docx-1-cms-10.1177_12034754261418237 for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study by Gianluca Avallone, Gabriele Roccuzzo, Luca Valtellini, Chiara Moltrasio, Giovanni Genovese, Federica Repetto, Mohamed Aouadi, Alessia Moglia, Flavia Manzo Margiotta, Natale Schettini, Fabrizio Martora, Luigi Gargiulo, Mario Valenti, Dalma Malvaso, Nicoletta Bernardini, Annunziata Dattola, Claudio Conforti, Claudio Marasca, Federica Derlino, Carlo Alberto Maronese, Silvia Giordano, Francesca Satolli, Valentina Dini, Vincenzo Bettoli, Matteo Megna, Antonio Costanzo, Ketty Peris, Nevena Skroza, Antonio Giovanni Richetta, Luca Fania, Pietro Quaglino, Giovanni Pellacani, Angelo Valerio Marzano and Simone Ribero in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-2-cms-10.1177_12034754261418237 – Supplemental material for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study
Supplemental material, sj-docx-2-cms-10.1177_12034754261418237 for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study by Gianluca Avallone, Gabriele Roccuzzo, Luca Valtellini, Chiara Moltrasio, Giovanni Genovese, Federica Repetto, Mohamed Aouadi, Alessia Moglia, Flavia Manzo Margiotta, Natale Schettini, Fabrizio Martora, Luigi Gargiulo, Mario Valenti, Dalma Malvaso, Nicoletta Bernardini, Annunziata Dattola, Claudio Conforti, Claudio Marasca, Federica Derlino, Carlo Alberto Maronese, Silvia Giordano, Francesca Satolli, Valentina Dini, Vincenzo Bettoli, Matteo Megna, Antonio Costanzo, Ketty Peris, Nevena Skroza, Antonio Giovanni Richetta, Luca Fania, Pietro Quaglino, Giovanni Pellacani, Angelo Valerio Marzano and Simone Ribero in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-3-cms-10.1177_12034754261418237 – Supplemental material for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study
Supplemental material, sj-docx-3-cms-10.1177_12034754261418237 for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study by Gianluca Avallone, Gabriele Roccuzzo, Luca Valtellini, Chiara Moltrasio, Giovanni Genovese, Federica Repetto, Mohamed Aouadi, Alessia Moglia, Flavia Manzo Margiotta, Natale Schettini, Fabrizio Martora, Luigi Gargiulo, Mario Valenti, Dalma Malvaso, Nicoletta Bernardini, Annunziata Dattola, Claudio Conforti, Claudio Marasca, Federica Derlino, Carlo Alberto Maronese, Silvia Giordano, Francesca Satolli, Valentina Dini, Vincenzo Bettoli, Matteo Megna, Antonio Costanzo, Ketty Peris, Nevena Skroza, Antonio Giovanni Richetta, Luca Fania, Pietro Quaglino, Giovanni Pellacani, Angelo Valerio Marzano and Simone Ribero in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-4-cms-10.1177_12034754261418237 – Supplemental material for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study
Supplemental material, sj-docx-4-cms-10.1177_12034754261418237 for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study by Gianluca Avallone, Gabriele Roccuzzo, Luca Valtellini, Chiara Moltrasio, Giovanni Genovese, Federica Repetto, Mohamed Aouadi, Alessia Moglia, Flavia Manzo Margiotta, Natale Schettini, Fabrizio Martora, Luigi Gargiulo, Mario Valenti, Dalma Malvaso, Nicoletta Bernardini, Annunziata Dattola, Claudio Conforti, Claudio Marasca, Federica Derlino, Carlo Alberto Maronese, Silvia Giordano, Francesca Satolli, Valentina Dini, Vincenzo Bettoli, Matteo Megna, Antonio Costanzo, Ketty Peris, Nevena Skroza, Antonio Giovanni Richetta, Luca Fania, Pietro Quaglino, Giovanni Pellacani, Angelo Valerio Marzano and Simone Ribero in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-5-cms-10.1177_12034754261418237 – Supplemental material for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study
Supplemental material, sj-docx-5-cms-10.1177_12034754261418237 for Long-Term Outcomes of Secukinumab in Moderate-to-Severe Hidradenitis Suppurativa: A Multicentre Cohort Study by Gianluca Avallone, Gabriele Roccuzzo, Luca Valtellini, Chiara Moltrasio, Giovanni Genovese, Federica Repetto, Mohamed Aouadi, Alessia Moglia, Flavia Manzo Margiotta, Natale Schettini, Fabrizio Martora, Luigi Gargiulo, Mario Valenti, Dalma Malvaso, Nicoletta Bernardini, Annunziata Dattola, Claudio Conforti, Claudio Marasca, Federica Derlino, Carlo Alberto Maronese, Silvia Giordano, Francesca Satolli, Valentina Dini, Vincenzo Bettoli, Matteo Megna, Antonio Costanzo, Ketty Peris, Nevena Skroza, Antonio Giovanni Richetta, Luca Fania, Pietro Quaglino, Giovanni Pellacani, Angelo Valerio Marzano and Simone Ribero in Journal of Cutaneous Medicine and Surgery
Footnotes
Author Contributions
G.A., G.R., L.V.: data curation, conceptualization, methodology, writing—original draft preparation. C.M., G.G., F.R., M.A., A.M., F.M.M., N.S., F.M., L.G., M.V., D.M., N.B., A.D., C.C., C.M., F.D., C.A.M., S.G., F.S., V.D., V.B., M.M., A.C., K.P., N.S., A.G.R., L.F., P.Q., and G.P.: data curation, writing—review and editing. S.R.: supervision, writing—review and editing, final approval of the draft. A.V.M.: supervision, writing—review and editing, final approval of the draft.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.R. has received honoraria/travel grants or research grants from AbbVie, Novartis, J&J, BMS, Almirall, Sandoz, L’Oréal, UCB, Eli Lilly, and Leo Pharma. K.P. has served on advisory boards for Almirall, AbbVie, Biogen, Celgene, Leo Pharma, Novartis, Pierre Fabre, Sanofi, Sandoz, Sun Pharma, and Janssen, and has been a principal investigator for Almirall, AbbVie, Eli Lilly, Galderma, Leo Pharma, Novartis, Sanofi, and Janssen. AVM has received consulting fees and disease-relevant honoraria from AbbVie, Amgen, Boehringer Ingelheim, BMS, Incyte, Leo Pharma, Novartis, Pfizer, Sanofi, and UCB.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Reviewed and approved by Ethics Committee of AOU Città della Salute e della Scienza di Torino: approval no. SS-Dermo16-HS #0055827.
Consent for Publication
The patients in this manuscript have given written informed consent to the publication of their case details.
Supplemental Material
Supplemental material for this article is available online.