
Abstract
Background:
Data on the incidence of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) in Thailand, where high-risk HLA alleles are prevalent, remain limited. Existing prognostic scores, including SCORTEN, may not capture all mortality determinants.
Objective:
To estimate the incidence and identify factors associated with in-hospital mortality in adult patients with SJS/TEN in Thailand.
Methods:
We conducted a retrospective cohort study using the nationwide Thai National Health Security Office database. Adults hospitalized with SJS/TEN were identified by International Statistical Classification of Diseases, 10th Revision codes between 2017 and 2024. Cox regression with time-varying coefficients was used to examine mortality risk factors.
Results:
A total of 7237 incident cases were identified (83.9% SJS). Median age was 57 years (interquartile range 42-69), and 50.5% were female. The estimated incidence was 17.3/million (95% confidence interval [CI], 16.9-17.7), with a decline over time. In-hospital mortality was 4.1% for SJS and 15.5% for TEN. Independent factors associated with mortality beyond SCORTEN included invasive ventilation (hazard ratio [HR], 14.99; 95% CI, 7.08-31.75), liver disease (HR, 2.49; 95% CI, 1.13-5.46), renal disease (HR, 2.46; 95% CI, 1.96-3.04), and myocardial infarction (HR, 1.90; 95% CI, 1.19-3.04). Mortality risk also increased progressively with age (≥60 years) and varied by hospital type. Time-varying analysis showed that TEN, liver disease, and ventilation had the strongest early impact, whereas infections, particularly skin and soft tissue infections, emerged later (HR at day 28, 2.64; 95% CI, 1.37-5.09).
Conclusions:
The incidence of SJS/TEN in Thailand is high. Mortality is influenced by factors beyond established scoring systems, with effects that evolve over time.
Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but life-threatening dermatologic emergencies, most often triggered by adverse drug reactions. 1 They are associated with long-term morbidity, high mortality, and considerable healthcare burden. 2 Disease severity is classified according to the extent of skin detachment into SJS (<10%), SJS/TEN overlap (10%-30%), and TEN (>30%).
The global incidence of SJS/TEN is estimated at 1 to 13 cases/million/year, but rates vary considerably across regions. 1 Genetic susceptibility, particularly the distribution of high-risk HLA alleles, is an important contributor to regional variation. For example, HLA-B*15:02 and HLA-B*58:01, which are linked to carbamazepine- and allopurinol-induced SJS/TEN, are prevalent in Southeast Asian populations. 1 Given the established interaction between these drugs and high-risk HLA alleles, nationwide epidemiologic data are needed to better characterize the burden of SJS/TEN in Thailand.
Mortality rates of SJS/TEN range from 10% to 40% worldwide, 1 but predicting outcomes remains challenging. The SCORTEN score is the most widely used prognostic model, but its performance could be inconsistent, particularly in patients with multiple comorbidities not included in the score.3,4 Furthermore, most existing evidence comes from single-center studies with relatively small sample sizes, limiting generalizability. 4 Identifying additional prognostic factors in large, diverse cohorts is therefore essential to refine risk stratification.
To address these gaps, we conducted a nationwide cohort study using the Thai National Health Security Office (NHSO) database from 2017 to 2024. Our objectives were to estimate the incidence of SJS/TEN among adults in Thailand and to identify factors associated with in-hospital mortality.
Materials and Methods
Study Population and Data Source
This retrospective study examined a comprehensive national dataset obtained from Thailand, focusing on adult patients (aged ≥18 years) admitted to hospitals with SJS and TEN between January 1, 2017 and December 31, 2024. Pediatric patients were excluded because SJS/TEN in children differs from adult disease in comorbidity profile, medication exposure, and baseline mortality risk. Given that the study aimed to estimate incidence and evaluate factors associated with in-hospital mortality, particularly comorbidity-related factors, the cohort was restricted to adults to reduce clinical heterogeneity and improve the interpretability of multivariable analyses.
Data were acquired from the NHSO and classified according to the International Statistical Classification of Diseases, 10th Revision, Thai Modification (ICD-10-TM). SJS/TEN cases were categorized based on ICD-10 codes L51.1 to L51.3 as primary diagnoses. Incident cases were defined as hospitalization episodes with a principal diagnosis of SJS/TEN. The database is structured at the hospitalization (visit) level and does not support linkage of individual patients across multiple admissions. Therefore, repeated admissions or inter-hospital transfers could not be excluded.
The dataset included demographic variables such as patient age, sex, and month and year of admission and discharge. Age was analyzed both as a continuous variable and categorized into 5 groups (18-39, 40-59, 60-69, 70-79, and ≥80 years), consistent with SCORTEN and other severity scoring systems.3,5 -7 Additional variables included length of hospital stay (LOS), geographical health regions (Bangkok, central, northern, eastern, northeastern, and southern divisions).
Hospitals were categorized according to the Thai Ministry of Public Health classification system, which reflects differences in service capacity and referral role. University-affiliated hospitals are tertiary academic centers that provide comprehensive subspecialty care, advanced critical care services, and serve as national referral centers. Regional hospitals are large tertiary-level referral centers with broad specialty services and intensive care capabilities. General hospitals provide secondary-level care and function as provincial referral centers with more limited subspecialty capacity. Community hospitals primarily deliver primary and basic inpatient care and typically stabilize patients prior to referral to higher-level facilities when advanced management is required.
Secondary diagnoses were identified using ICD-10 codes and classified according to the Charlson Comorbidity Index (CCI). Because the administrative dataset does not include present-on-admission indicators, these recorded conditions may represent either preexisting comorbidities or complications occurring during hospitalization. The Charlson comorbidities included renal disease (ICD-10: I120, I131, N03, N05, N17, N18, N19, N250, Z49), myocardial infarction (I21, I22, I252), congestive heart failure (I099, I110, I130, I132, I255, I420, I425-I429, I43, I50, P290), peripheral vascular disease (I70, I71, I731, I738, I739, I771, I790, I792, K551, K558, K559, Z958, Z959), cerebrovascular disease (G45, G46, I60-I69, H340, G041, G114, G80-G84), hemiplegia (G041, G114, G801, G802, G81, G82, G830-G834, G839), dementia (F00-F03, F05, G30, G311), chronic pulmonary disease (I278, I279, J40-J47, J60-J67, J684, J701, J703), rheumatic disease (M05, M06, M31-M36), peptic ulcer disease (K25-K28), liver disease (K70-K77), malignancies (C00-C97), HIV infection (B20-B22, B24), and diabetes mellitus (E10-E14). Additional conditions previously associated with SJS/TEN mortality were also considered, including septicemia (A021, A227, A267, A328, A40, A41, A427, B377), tuberculosis (A16-A19), skin infections (L08), urinary tract infections (N390), pneumonia (J10-J18, B012, B052, B206, B953, B960, B961), and acidosis (E872). Procedures of interest comprised intravenous immunoglobulin infusion (ICD-9: 99.14), parenteral nutrition (99.15), renal replacement therapy (hemodialysis [ICD-9:39.95] or peritoneal dialysis [ICD-9:54.98]), and noninvasive or invasive mechanical ventilation (93.9, 96.7). In addition, ocular procedures were identified from ICD-9 codes for operations on the eye, orbit, and adnexa (10, 80, 82, 84-89, 94, 101-105, 112-116, 119, 128-129, 144, 159, 162-163), while urogenital procedures were defined by codes for operations on the urinary tract and male/female genital organs (57-69). Healthcare expenditures and discharge status were also analyzed.
Statistical Analysis
Demographic data were summarized using descriptive statistics. Normally distributed variables were reported as mean ± standard deviation, whereas non-normally distributed data were presented as median with interquartile range (IQR).
Incidence rates of SJS/TEN were calculated as the number of new cases divided by national person-years at risk, based on annual Thai population statistics, and expressed per 1 000 000 person-years. Ninety-five percent confidence intervals (CIs) were derived from Poisson models using annual mid-year population estimates (2017-2024). Age-adjusted rates were subsequently estimated using the direct standardization method, applying weights from the proportional representation of age groups in the reference population. Admission rates associated with SJS/TEN were also computed per 100 000 individuals.
For factors associated with in-hospital mortality, univariable Cox regression was performed for all candidate factors and expressed as crude hazard ratios (HRs) with 95% CIs, and variables with P < .20 were considered for multivariable modeling. Collinearity was assessed using Pearson correlation coefficients; when strong correlations were identified, only the most clinically relevant variable was retained. Multivariable Cox proportional hazards models were then fitted, and results were reported as adjusted HRs with 95% CIs.
Proportional hazards assumptions were evaluated using Schoenfeld residuals and log-log survival plots. Variables that violated the assumption were modeled using extended Cox regression with interactions between covariates and ln(time). For these factors, time-varying HRs were reported at clinically relevant intervals (days 7 and 28), and HR(t) curves with 95% confidence bands were plotted. All analyses were performed using Stata version 16.1 (StataCorp, College Station, TX, USA), and 2-sided P < .05 was considered statistically significant. Ethical approval was obtained from the Human Research Ethics Committee, Institutional Review Board of Khon Kaen University (HE681587).
Results
Demographic Data of the Studied Populations
Supplementary Table S1 presents the demographic and clinical characteristics of 7237 hospitalized adults with SJS/TEN between 2017 and 2024. The median age was 57 years (IQR 42-69), with the largest proportion in the 18 to 39 year age group; 50.5% were female. Most patients resided in northeastern Thailand. Renal disease was the most frequently recorded coexisting condition, and 5% required invasive mechanical ventilation. The majority were treated at regional or general hospitals. The median LOS was 6 days (IQR 4-10), with median healthcare costs of USD 317.79 (187.02-423.65). The overall in-hospital mortality was 5.96%, with higher mortality in TEN (15.52%) compared with SJS (4.11%). No cases were coded as SJS/TEN overlap (ICD-10 L51.3) in the database. The overall incidence of SJS/TEN was 17.3/1 000 000 person-years (95% CI, 16.9-17.7), with SJS at 14.5 (95% CI, 14.2-14.9) and TEN at 2.8 (95% CI, 2.6-3.0). Age-adjusted hospitalization rates for SJS/TEN from 2017 to 2024 are presented in Figure 1.
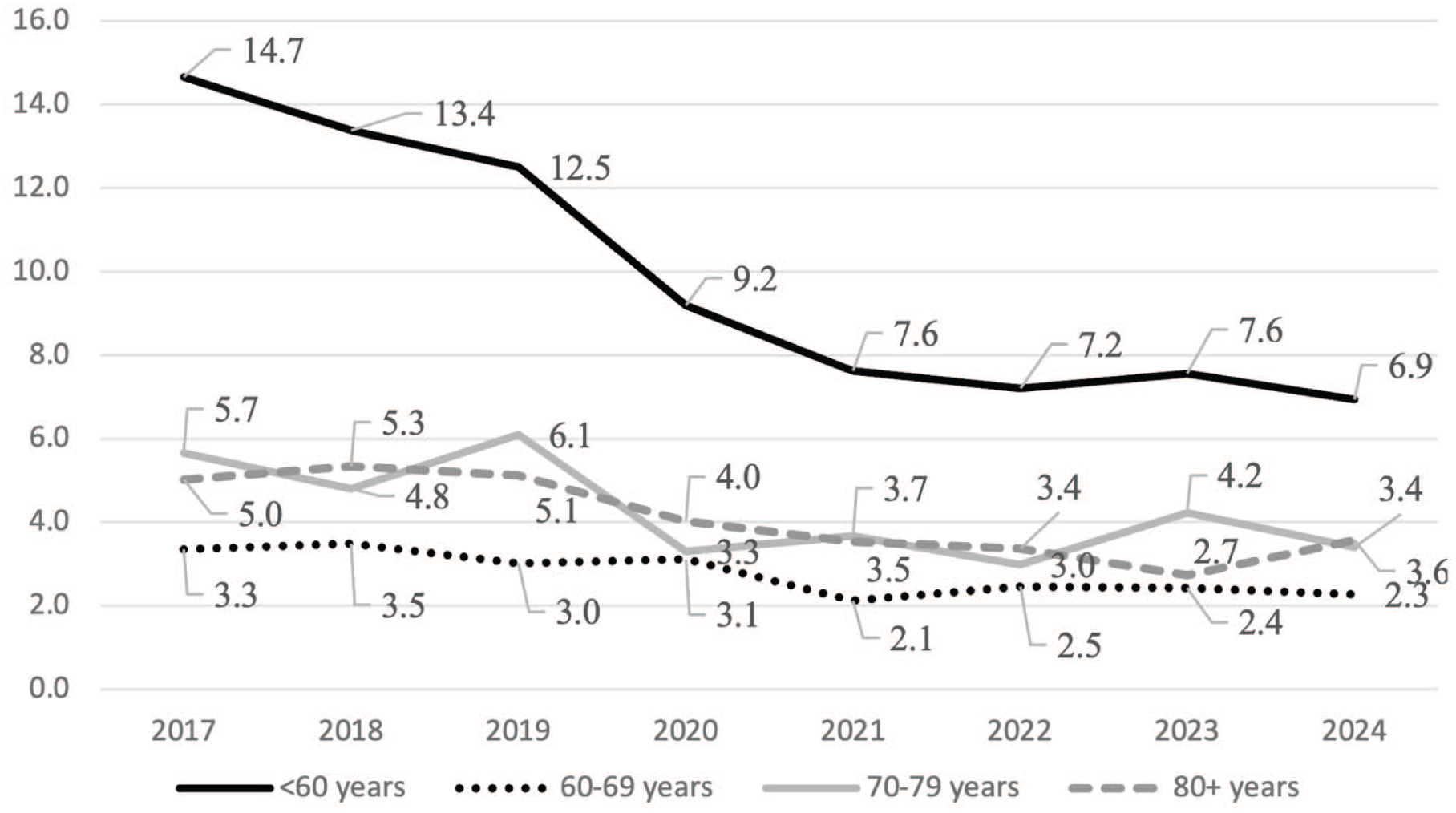
Age-adjusted rates of hospitalization due to SJS/TEN from 2017 to 2024. SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis.
Factors Associated With In-Hospital Death of Patients With SJS/TEN From 2017 to 2024
In the univariate Cox regression analysis, factors associated with in-hospital death (P < .20) included age, healthcare region, hospital type, principal diagnosis (SJS or TEN), and coexisting diagnoses recorded during hospitalization such as renal disease, myocardial infarction, hemiplegia, peptic ulcer, liver disease, malignancy, HIV infection, diabetes mellitus, acidosis, malnutrition, septicemia, skin and soft tissue infection, urinary tract infection, and pneumonia. Invasive procedures, including renal replacement therapy, an indwelling Foley catheter, ocular procedures, noninvasive ventilation, and invasive mechanical ventilation were also significant. Intravenous immunoglobulin (IVIG) administration was not significantly associated with in-hospital mortality.
Pearson correlation analysis demonstrated high collinearity between age and age by group (r = 0.96), between CCI and HIV infection (r = 0.76), between all malignancies and solid malignancy (r = 0.92), and between genital procedure and indwelling Foley catheter (r = 0.97). To avoid collinearity, only age by group, HIV infection, all malignancies, and an indwelling Foley catheter were retained in the final model.
The selected variables were then entered into the multivariable Cox regression model. The standard Cox model assumes that the HR associated with each predictor remains constant over time. We therefore assessed whether this assumption was met for each variable. For several predictors, including principal diagnosis, liver disease, infections, and invasive mechanical ventilation, the association with mortality changed during hospitalization rather than remaining constant. These factors were, therefore, modeled using time-dependent effects, allowing their impact on mortality to vary over time.
In the final multivariable analysis, factors independently associated with increased risk of in-hospital death (P < .05) included older age (particularly ≥60 years compared with 18 to 39 years), admission to regional and general hospitals compared with university-affiliated hospitals, diagnosis of TEN, and coexisting diagnoses recorded during hospitalization such as renal disease, myocardial infarction, liver disease, and acidosis. Receipt of invasive mechanical ventilation was also associated with increased mortality risk. By contrast, pneumonia was associated with a lower risk of death in the baseline analysis (P = .01). When modeled as time-varying covariates, infections demonstrated changing effects over time: the HR for skin and soft tissue infection was low at baseline (HR 0.19, 95% CI, 0.18-2.02) but increased substantially by day 28 (HR 2.64, 95% CI, 1.37-5.09). Similar time-dependent risk patterns were observed for pneumonia and urinary tract infection. In contrast, the effects of invasive mechanical ventilation, principal diagnosis, and liver disease were the highest risk at an early stage, but diminished with time. For example, invasive mechanical ventilation was associated with markedly increased mortality early in admission (HR 14.99, 95% CI, 7.08-31.75 at baseline) but the effect attenuated by day 28 (HR 2.17, 95% CI, 1.48-3.17). A similar effect was observed for TEN (principal diagnosis) and for liver disease. Full results are summarized in Supplementary Table S2, with time-varying HRs illustrated in Figure 2.
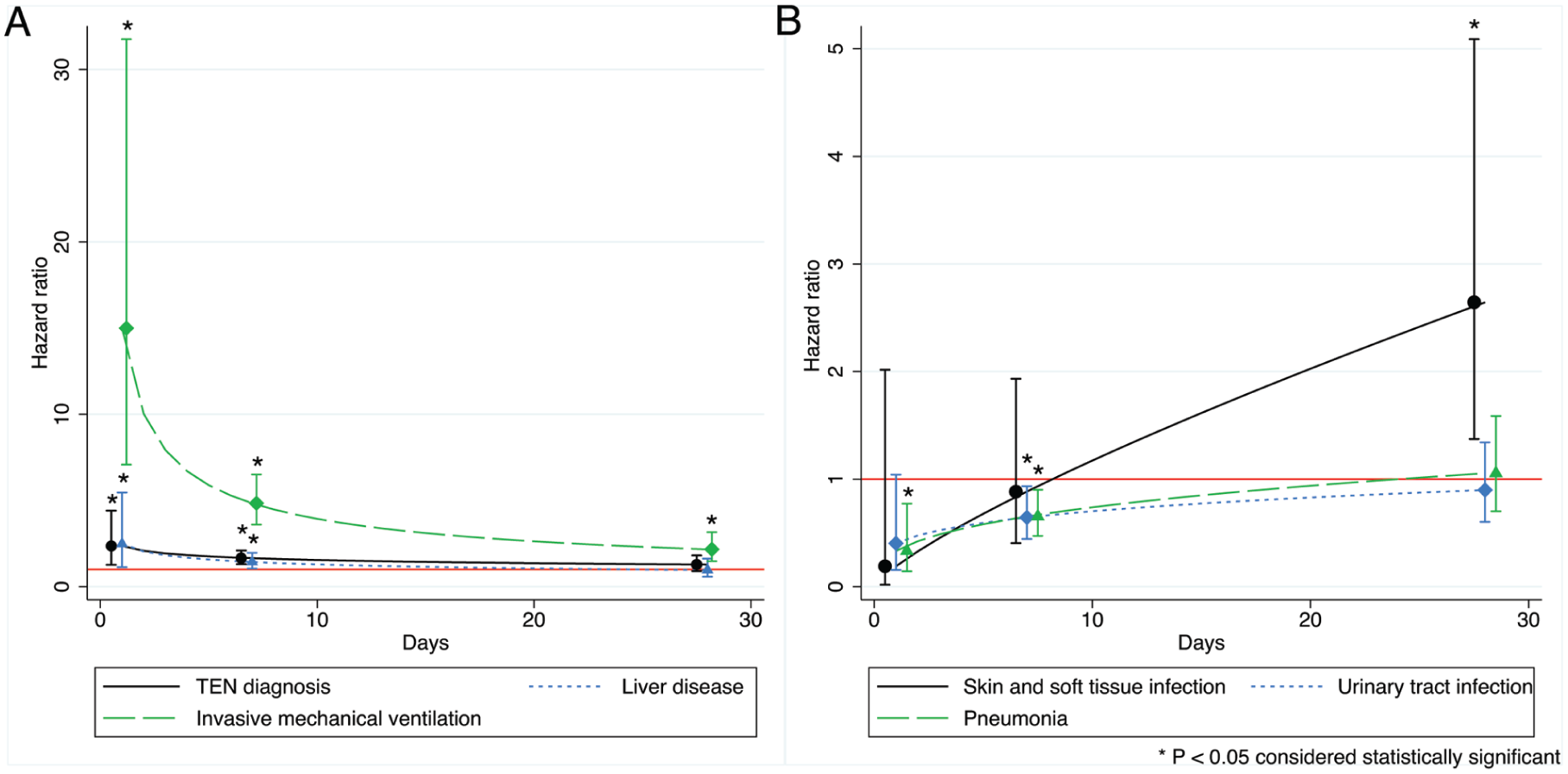
Time-varying hazard ratios for mortality in SJS/TEN. (A) The effects of TEN diagnosis, liver disease, and invasive mechanical ventilation diminished over time. (B) Infections (skin and soft tissue, urinary tract, and pneumonia) became increasingly important later in hospitalization, with skin and soft tissue infection showing a significant effect at day 28. SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis.
Discussion
Incidence and Temporal Trends
This nationwide cohort study describes Thai patients with SJS/TEN between 2017 and 2024. The overall incidence was 17.3/million population (14.5 for SJS and 2.8 for TEN), which is higher than most previously reported rates, including those from other Asian countries such as Korea (3.9-5.0 for SJS and 0.9-1.5 for TEN) and Japan (reported as prevalence, 2.5 for SJS and 1.0 for TEN).8 -13 This difference may partly reflect genetic susceptibility, as high-risk HLA alleles (eg, HLA-B*15:02 and HLA-B*58:01) are present in more than 10% of the Thai population. 1 We observed a declining trend in hospitalizations over time, consistent with a previous report. 12 In Thailand, pre-prescription HLA-B*15:02 screening prior to carbamazepine use was incorporated into national reimbursement policy in 2018, while HLA-B*58:01 screening prior to allopurinol was added in 2021.14,15 Although the present database does not contain prescribing or genetic testing data, the temporal pattern of decline may be associated with the progressive implementation of pharmacogenomic screening policies. This observation highlights the potential population-level impact of regulatory pharmacogenomic screening initiatives on severe adverse drug reactions. Despite these trends, in-hospital mortality in our cohort was 4.11% for SJS and 15.52% for TEN, comparable to outcomes reported in other countries.11 -13
Factors Associated With Mortality and Scoring Systems
Several prognostic scoring systems, SCORTEN, ABCD-10, AllSCAR, and CRISTEN, have been developed to predict mortality in SJS/TEN.3,5 -7 These models incorporate age, body surface area involvement, comorbidities (eg, chronic kidney disease, diabetes, cardiovascular disease, and malignancy), laboratory abnormalities (elevated blood urea nitrogen (BUN), metabolic acidosis, and hyperglycemia), and infections. Among them, SCORTEN remains the most widely used model and has demonstrated moderate discriminatory performance in Thai cohorts (area under the receiver-operator curve = 0.77). 7
In line with these models, our multivariable analysis showed that advancing age significantly increased mortality risk, particularly among patients over 60 years, with risk rising in a graded fashion. This is consistent with previous reports and likely reflects the greater vulnerability of elderly patients to complications and comorbidities.12,16 It suggests that age may warrant greater weighting in future refinements of prognostic models. Although our dataset did not include overlap cases, a diagnosis of TEN was independently associated with mortality, underscoring the prognostic impact of extensive skin detachment.
Renal disease was also identified as strongly associated with increased mortality, consistent with prior studies.2,5,17,18 However, receipt of renal replacement therapy was not independently associated with mortality in our analysis, in contrast to earlier reports. 19 This discrepancy may reflect residual confounding or differences in study design.
Cardiovascular comorbidities have also been proposed as mortality predictors, as in the CRISTEN scoring system, possibly because affected patients are exposed to multiple medications and at risk of drug-drug interactions. 5 Such interactions may accelerate hypersensitivity or worsen disease severity. Preexisting cardiovascular disease has also been suggested as a marker of bacteremia in SJS/TEN. 20 In our study, myocardial infarction predicted mortality, whereas congestive heart failure and diabetes mellitus did not, in contrast to CRISTEN. This may reflect ICD-10 coding limitations, which may group stable heart failure and well-controlled diabetes together with more severe disease, potentially diluting their prognostic effect. However, our results emphasize the particularly strong association between myocardial infarction and in-hospital mortality among cardiovascular conditions.
Malignancy, particularly solid tumors, was associated with mortality in univariable analysis but was only borderline significant in multivariable models. This may similarly reflect ICD-10 coding, which cannot distinguish active from remote malignancy, an important prognostic factor. 21 Hematologic malignancy was not associated with mortality in our cohort, contrary to previous studies, likely because of the small number of cases. 2 As proxies for unavailable laboratory data, we used renal disease and acidosis to reflect elevated BUN and low bicarbonate; both were significantly associated with mortality, in line with earlier reports. 3
Infections were also important predictors of mortality. Previous studies identified systemic infections (eg, pneumonia, urinary tract infection, and skin and soft tissue infection) as risk factors but did not assess the timing of the effect.5,7,22 Using time-varying coefficient analysis, we found that the impact of infections evolved dynamically: HRs were initially low, likely reflecting survivor bias, but rose steadily, becoming significant by 28 days, particularly for skin and soft tissue infections. This aligns with prior reports that skin is the most common source of bacteremia in SJS/TEN and underscores the importance of infection prevention and close monitoring throughout hospitalization. 22
Additional Predictors
Reports have noted the underperformance of established scoring systems, especially in patients with multiple comorbidities. 4 Our study identified additional predictors. Liver disease was significantly associated with mortality, consistent with earlier findings, possibly explained by increased antigen formation, drug-drug interactions, or toxic serum drug levels. 23 Invasive mechanical ventilation showed the strongest association with mortality, which is biologically plausible given that SJS/TEN can cause bronchial epithelial necrosis and airway compromise, and ventilation often reflects severe disease.24,25 Time-varying analysis further revealed that the effects of mechanical ventilation, liver disease, and TEN diagnosis were greatest early in hospitalization but attenuated over time, suggesting that these patients may benefit from early, aggressive management, including intensive supportive care in specialized ICUs with vigilant monitoring, consideration of specific therapies where appropriate, and timely referral to expert centers when needed. 26
Patients with HIV infection are known to be at increased risk of developing SJS/TEN. However, some studies have reported mortality to be lower than predicted, and CD4 count has not been shown to correlate with SCORTEN.27,28 Consistent with this, we found that HIV status was not independently associated with in-hospital mortality. This may partly reflect closer clinical monitoring in HIV programs, which could facilitate earlier recognition and prompt drug withdrawal. Immunologic factors may also play a role. Because the pathogenesis of SJS/TEN is driven primarily by CD8+ cytotoxic T cells, natural killer cells, and NKT cells, depletion of CD4+ lymphocytes in HIV may contribute less directly to prognosis. 1 Further studies evaluating the role of CD4 counts are needed to clarify their impact on SJS/TEN outcomes.
Tuberculosis has also previously been proposed as a mortality risk factor in SJS/TEN. 2 However, a recent epidemiologic study by Wasuwanich et al during the same study period as ours found no significant association, likely because of low case numbers. 12 Considering Thailand is endemic for tuberculosis, we included 459 patients with tuberculosis, but similarly found no association with mortality. Therefore, while tuberculosis patients may be at risk of developing SJS/TEN, tuberculosis infection itself does not appear to increase mortality risk.
SJS/TEN has also been associated with gastrointestinal complications such as peptic ulcer disease and malnutrition, which may worsen prognosis.29,30 However, no significant associations were observed in our study, likely because of small case numbers and potential underreporting.
Beyond patient factors, hospital type significantly influenced outcomes in our cohort, consistent with previous studies showing that patients admitted to centers with SJS/TEN expertise have better prognoses.31,32 Limited dermatology expertise and resource availability in some hospitals may explain this variation, underscoring the need for improved early recognition, referral systems, and standardized care. Regarding treatment, IVIG use was not associated with reduced mortality in our cohort, consistent with previous conflicting reports. 33 We were unable to assess corticosteroids because of potential underreporting or anti-TNF agents due to lack of specific ICD-9 codes. These limitations highlight the need for prospective studies with detailed treatment data.
Our study has several strengths. It is the first nationwide analysis of SJS/TEN in Thailand, encompassing a large, representative population over multiple years, and it characterizes both incidence and mortality predictors in an Asian population known for higher genetic susceptibility compared to non-Asian populations. The use of linked hospital discharge data allowed us to capture a wide range of comorbidities, complications, and in-hospital outcomes. Furthermore, the application of time-varying coefficient analysis provided novel insights into the dynamic effects of infections, comorbidities, and procedures on mortality risk.
However, several limitations should be acknowledged. This study was based on a hospitalization-level administrative database that lacks present-on-admission indicators and unique patient identifiers; therefore, recorded coexisting diagnoses may represent either pre-existing comorbidities or complications developing during hospitalization, and repeated admissions or inter-hospital transfers could not be excluded. Accordingly, the reported incidence reflects admission-based rather than person-based rates. Reliance on ICD-10 and ICD-9 coding may have introduced misclassification, including possible reclassification of SJS/TEN overlap cases under SJS or TEN because of coding practices. In addition, because erythema multiforme shares overlapping diagnostic codes with SJS, some degree of diagnostic overlap cannot be excluded. However, infections typically associated with erythema multiforme were infrequently recorded in this cohort. Key clinical variables, including body surface area detachment, laboratory parameters required for SCORTEN calculation, genetic information such as high-risk HLA alleles, and detailed treatment data for both SJS/TEN and underlying comorbid conditions, were unavailable, precluding formal SCORTEN validation, direct evaluation of HLA-associated risk, and assessment of treatment-modifying effects. Furthermore, the study was restricted to adults (≥18 years), and incidence was calculated using national population figures as the denominator. As the NHSO database covers ~70% of the Thai population and healthcare access varies across regions, including more limited availability of dermatology specialists and advanced diagnostic services in some rural areas, the reported rates may not fully capture the true national burden. Finally, residual confounding cannot be excluded despite multivariable adjustment.
Conclusion
This nationwide adult cohort demonstrates that the incidence of SJS/TEN in Thailand is higher than rates reported in several other countries. In-hospital mortality was independently associated with older age, TEN diagnosis, cardiovascular, renal, and liver comorbidities, mechanical ventilation, and hospital type. Time-varying analysis showed that TEN diagnosis, liver disease, and mechanical ventilation were linked to increased early mortality risk, whereas infectious complications became more prominent later during hospitalization. These findings emphasize the importance of early recognition of high-risk patients and continued monitoring for complications throughout hospitalization. Further research is needed to clarify how dynamic risk factors can be better addressed to improve outcomes in SJS/TEN.
Supplemental Material
sj-doc-3-cms-10.1177_12034754261455749 – Supplemental material for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort
Supplemental material, sj-doc-3-cms-10.1177_12034754261455749 for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort by Rachot Wongjirattikarn, Charoen Choonhakarn, Suteeraporn Chaowattanapanit, Anupol Panitchote, Narachai Julanon, Thanaphon Anutraungkool, Poonchana Wareechai and Panita Limpawattana in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-1-cms-10.1177_12034754261455749 – Supplemental material for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort
Supplemental material, sj-docx-1-cms-10.1177_12034754261455749 for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort by Rachot Wongjirattikarn, Charoen Choonhakarn, Suteeraporn Chaowattanapanit, Anupol Panitchote, Narachai Julanon, Thanaphon Anutraungkool, Poonchana Wareechai and Panita Limpawattana in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-2-cms-10.1177_12034754261455749 – Supplemental material for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort
Supplemental material, sj-docx-2-cms-10.1177_12034754261455749 for Incidence and Factors Associated With In-Hospital Mortality in Adult Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Nationwide Thai Cohort by Rachot Wongjirattikarn, Charoen Choonhakarn, Suteeraporn Chaowattanapanit, Anupol Panitchote, Narachai Julanon, Thanaphon Anutraungkool, Poonchana Wareechai and Panita Limpawattana in Journal of Cutaneous Medicine and Surgery
Footnotes
Acknowledgements
We would like to thank the National Health Security Office (NHSO), Bangkok, Thailand, and the Research Program of Khon Kaen University (RP68-5-001) for their support.
Ethical Considerations
This research obtained ethical approval from the Human Research Ethics Committee of the Institutional Review Board at Khon Kaen University (HE681587).
Author Contributions
R.W. was responsible for conceptualization, data analysis, visualization, and drafting of the manuscript. C.C. contributed to study design, supervision, and manuscript revision. S.C., N.J., and T.A. contributed to study design. A.P. assisted with data analysis and visualization. P.W. contributed to data collection. P.L. contributed to study design, data analysis, supervision, and critical revision of the manuscript. All authors reviewed and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.