
Abstract
This essay contrasts the experiences of hospitalization and transition from hospital to home of people who have recently acquired a spinal cord injury (SCI) and the health professionals who work with them before and during pandemic-related restrictions. These experiences are analyzed through the theoretical frameworks of liminality and intersectional Critical Disability Studies. Drawing on narrative-ethnographic data collected in Spain, I illustrate that the rehabilitation hospital is conceived as a “parenthetical bubble-shell” the boundedness and permeability of which was radically altered during lockdown. First, I discuss how this transformed the way people with an SCI adjust to new ways of approaching space and time in hospital settings. Second, I explore how lockdown impacted key processes of “discharge preparation.” Third, I argue that the intersection between ability, gender, and social class modulates the extent to which exiting the hospital before and during the pandemic represented an ongoing crisis.
Introduction
This article delves into partial results of an ongoing narrative-ethnographic study on what it means to “adjust” to a newly acquired spinal cord injury (SCI) in the context of a Spanish reference rehabilitation hospital, and the spatial and symbolic transition from hospital to home. My study addresses how people who were inpatients at the rehabilitation hospital or transitioning from hospital to home in March 2020 experienced the mutual effects of the crisis that comes with acquiring an SCI and the so-called “coronavirus crisis.” Shortly after lockdown in Spain began mid-March 2020, the regional Department of Health instructed the specialized rehabilitation hospital to hand over two of its four units to a nearby general hospital to treat COVID-19 patients. As a result, only the neurological patients who required professional care that could not be provided at home, remained in the hospital, isolated in their rooms. The other patients were discharged, and some did not get the chance to make important adjustments to their domestic space before going home.
This essay aims to expand our understanding of “disability adjustment” by contrasting the experiences of both patients and health professionals before and during pandemic restrictions. “Adjustment” has historically been of interest for my discipline, social psychology. More recently, several authors have begun developing a spatial-temporal understanding of adjustment (Gomersall & Madill, 2015; Papadimitriou, 2008) that addresses the geographical understandings of the “territorialities of disabled people” (Borioli, 2010, p. 245). I will engage with this interdisciplinary dialogue by linking it to the frameworks of liminality and intersectional Critical Disability Studies (CDS) (Goodley, 2017). This allows a better understanding of the relationship between the mutual dis/abling spaces and cultures of the pandemic crisis and SCI.
Disability and the Pandemic as Rites of Passage in a Dis/Ableist World
Van Gennep (1960/1909) used liminality to refer to the intermediate phase of “rites of passage.” This is a special type of transition by which an individual (or a group) moves from one subject position (or a social order) to another. Typically, rites of passage begin with a crisis that results in a phase of spatial and symbolic separation of an individual or group from their place in the social structure. Through this separation, the structure of everyday life dissolves for the subject and they can enter a liminal phase. The liminal phase entails occupying an ambivalent borderland space (both physically and symbolically) in a waiting time while undergoing transformations to become something new. Afterward, the phase of physical and symbolic re-aggregation is expected to take place for the subject of the rite to resume a place in a “new normalcy.”
In his book Eventful Bodies, Schillmeier (2016) conceptualized illness, impairment, and the SARS-CoV epidemic that took place at the very beginning of the 21st century as “cosmopolitical events,” as they disrupt, question, alter, and endanger “embodied life and social orderings” (p. 132). Cosmopolitical events are the kind of crises that give way to a rite of passage so that a new order can arise. Indeed, the notion of rite of passage has been used to describe the “crisis” that comes with the advent of an SCI (Murphy et al., 1988) as well as the coronavirus crisis (Bell, 2021).
Traditionally, illness or impairment are said to cause a “disruption.” While Bury (1982, p. 169) argued such disruption is “biographical,” Gomersall and Madill (2015, p. 407) describe it as “chronotopic,” since what is disrupted is the ways the ill or injured subject moves through space and time. People who acquire an SCI are transferred to a specialized rehabilitation hospital which inaugurates a liminal phase where people “learn to live as a disabled person” (Murphy et al., 1988, p. 239). Street and Coleman (2012) noted that hospitals are of interest for geography as they are heterotopias, “a space of multiple orderings,” simultaneously “bounded and permeable” (p. 5). This essay will illustrate how the hospital’s regime of boundedness and permeability is crucial for disabled people to adjust to living with a chronotopic disruption.
While Gomersall and Madill (2015) do not use the following categories, it is clear from their study that “chronotopic disruption” involves in fact two disruptions: diachronotopic and synchronotopic. On one hand, diachronotopic disruption involves the before/after impairment axis. Namely, the fact that dis/ableism 1 establishes impaired bodies as an essentially lesser kind of human imposes a “ruptured time” (p. 408), as it is impossible for a person who has sustained an impairment to think of their own social place as a continuity. This is even more pressing when the impairment is associated with “enwheelment,” that is, the process of adjustment to a radically new way of relating with the physical and social space assembled along a wheelchair in hospital settings (Papadimitriou, 2008, p. 695; see also Gaete-Reyes, 2015). In fact, Papadimitriou and Stone (2011) argue that in hospital settings, not only does acquiring an SCI involve a spatial transformation, but also an existential-temporal one, since the disabled subject can no longer make decisions regarding the future based on the embodiment of before. It is therefore relevant to explore what ways of relating to space and time after impairment are encouraged in hospital settings.
On the other hand, synchronotopic disruption involves the inside/outside and self/other axes. The dis/ableist organization of space-time usually confines disabled people inside segregated and somewhat “adjusted” spaces (such as the rehabilitation hospital), itineraries, and rhythms. This limits their “spatial choices” in comparison with those of the “able-bodied” subject (Kitchin, 1998, p. 348) and situates them in what Kafer (2013) calls “crip time.” That is, disabled bodies orient themselves to time in a way that challenges “normative and normalising expectations of pace and scheduling” (p. 27). Following Campbell (2009), liminality lies in the fact that, outside of those spaces, itineraries, and rhythms, dis/ableism places impaired people “out of place” and “out of sync” with respect to others (Imrie, 2014; Rothfelder & Thornton, 2017, p. 368). This is why Murphy et al. (1988) argue that liminality expands beyond the physical “re-aggregation phase” that comes with discharge, so it is relevant to explore how chronotopic disruption is experienced inside and outside of the hospital.
Bell’s (2021) analysis of COVID-19 pointed to lockdown as a liminal space-time because the subjects who experienced it “become something else” through the transformation of the movement patterns of human and non-human agents in space and time. For many, lockdown meant entering “a world that seems to end at the sidewalk (. . .) for 70+ more days” (p. 81). Because of dis/ableism, this was a common reality for many disabled people living in the community even before the pandemic, which is why Samuels and Freeman (2021) claim that the pandemic universalized “crip time.” However, this does not mean that the pandemic equalized abled and disabled subjects. Thorneycroft and Asquith (2021) argue that during the pandemic “abled subjects have used their anxieties, precarities and precariousness to put disabled people in their place to shore up their own selves” (p. 142). “Putting disabled people in their place” has meant, for instance, to expose them to unprecedented amounts of violence by rendering them disposable and in effect “out of place” in hospital settings. I will show how the pandemic radically altered the opportunities for experiencing the aforementioned diachronotopic and synchronotopic disruptions.
Finally, in recent years, several studies have claimed that understanding dis/ableism calls for an intersectional approach (García-Santesmases and Sanmiquel-Molinero, 2022; Goodley, 2017). Elsewhere (Sanmiquel-Molinero, 2023), I have begun to explore how, as Gomersall and Madill (2015) argue, chronotopic disruption appears to be a “gendered phenomenon” (p. 413). As Soldatic and Meekosha (2012, p. 151) point out, “the disabled identity is not only gendered but also bears markers of class,” and this “mediates access to the vital social, moral and cultural capital necessary to become socially mobile.” These intersectional axes of difference have impacted chronotopic disruption after discharge during the pandemic.
Method
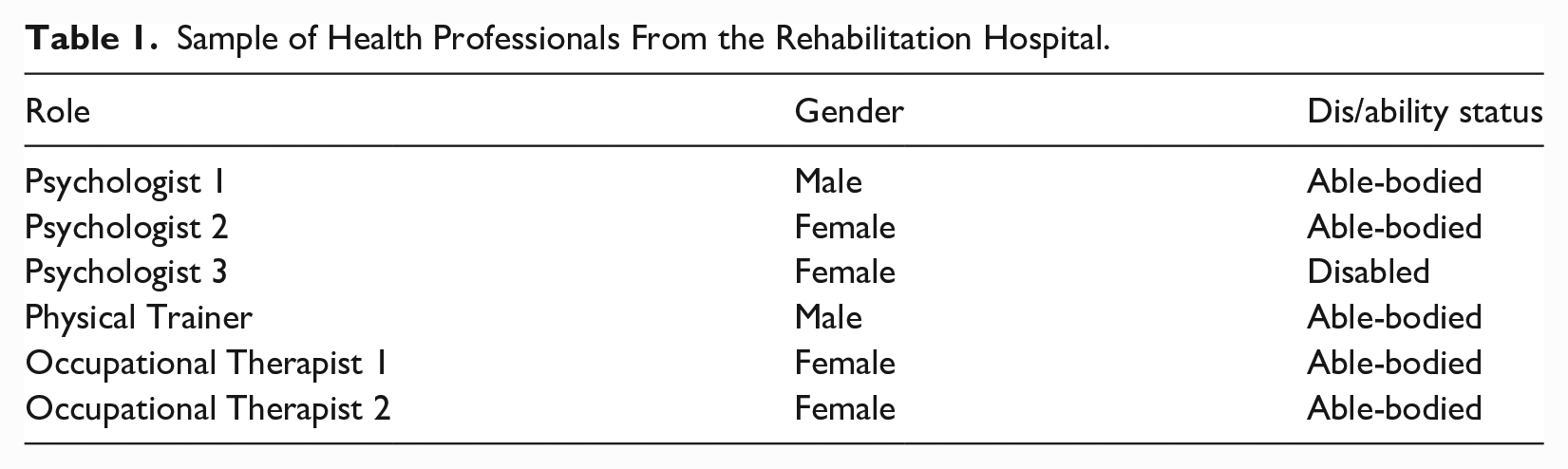
I combined two research techniques to study a rehabilitation hospital in Spain. On one hand, I chose an ethnographic approach triangulating participant observation in different hospital spaces, ethnographic interviews with psychology and rehabilitation professionals (Table 1), and “shadowing” (Jirón & Iturra, 2014). Shadowing consists of following people around during their daily routines in the rehabilitation hospital and outside to see how they interact with the world and how the world interacts with them. I applied this technique with five out of seven participants with an SCI (see Table 2) from June 2019 to March 2020 and from July 2020 to the present in a flexible scheme because of local Covid-19 restrictions. On the other hand, I undertook what I have elsewhere called “Chronotopic Diffraction” (CD), 2 where a narrative diary was constructed with six out of seven participants with an SCI through, on average, bi-monthly encounters. The theoretical, ethical, and political foundations of this technique can be found in Sanmiquel-Molinero (2023).
Sample of Health Professionals From the Rehabilitation Hospital.
Participants with an SCI.
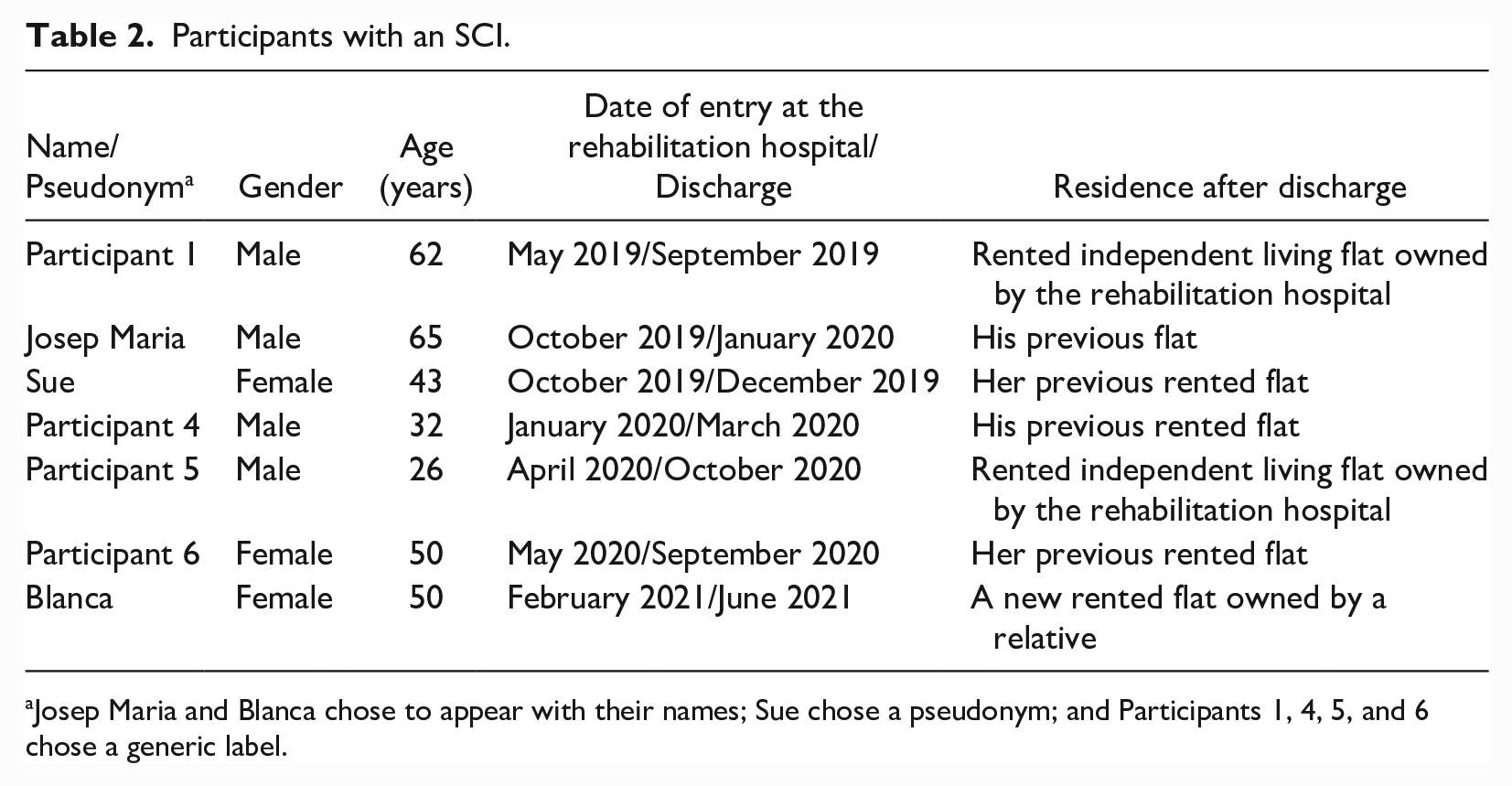
Josep Maria and Blanca chose to appear with their names; Sue chose a pseudonym; and Participants 1, 4, 5, and 6 chose a generic label.
Data collection started in June 2019 and was interrupted between March and June 2020 during lockdown because all preferred to suspend fieldwork. After lockdown, some CDs were constructed face-to-face, whereas others were developed online. Finally, data analysis involved iterative readings of my ethnographic notes as well as the narratives constructed with participants, during which I selected those extracts that referred to space and time in the hospital and the discharge process.
The Hospital as a Parenthetical Bubble-Shell
Before the start of the pandemic, several participants with an SCI and health professionals had already defined the rehabilitation hospital as a “bubble,” a metaphor that is sometimes associated with a “parenthesis” or a “shell”: During the last month, I have started to come out of the “[hospital name]-shell.” It has been wonderful. (. . .) In [hospital name], you are in a bubble because there is nothing. There is so much nature around, there are no shops. (Participant 1, December 2019, CD) I’m in a parenthesis. Sometimes I think about it and say: “Hell, somehow, this is like stopping time!.” (Participant 1, November 2020, CD)
These metaphors evoke a formative liminal space-time that is physically separated from the rest of the world, in the middle of nowhere and stops the flow of life (as parentheses do in texts). In the following two subsections, I develop how these metaphors relate to the two aforementioned modes of chronotopic disruption before and during the pandemic. The third subsection explores whether exiting the hospital means exiting the liminal phase epitomized by the metaphor of the “parenthetical bubble-shell.”
Diachronotopic Disruption: Situating an Emerging Enwheeled and Contemporizing Body-Subject
In terms of diachronotopic disruption, the idea of the hospital as a shell indicates that the birth of a new disabled body-subject is expected after a gestational stage that marks a before/after rupture. According to some professionals, lockdown merely “slowed down” the production of this “new, ready to exit the hospital-shell subject” for those who stayed in the hospital: People with an SCI who stayed in the hospital during lockdown really felt they were wasting their time (. . .). They were very anxious and craved rehabilitation (. . .). We have slowed down the process, but it has not stopped the expected levels of recovery. (Occupational Therapist 1, interview, September 2021)
The liminal space-time these patients occupied was expanded in terms of (waiting) time when compared with that of people who underwent hospitalization before lockdown, precisely because it was more compressed in terms of space. During lockdown, SCI patients remained isolated in their bedrooms: They could not attend the gym, the psychoeducation group, or receive external visits. In what follows, I will discuss the role of these three spaces in the constitution of an emerging “enwheeled and contemporising subject,” and the impact (or lack of thereof) lockdown had on this process.
Before lockdown, depending on the type of SCI and related medical complications, people could spend up to 5 hours per day in the gym. Just as the urban gym, the hospital gym is a space of “structured variety” (Sassatelli, 2015, p. 240), where different bodily techniques are applied in spatially segregated areas (the “walking department,” the “transfers area,” the “sports area,” to name just a few) for 1-hour long slots. In the gym, people with an SCI learn new ways of moving through space while “enwheeled” (Papadimitriou, 2008), but they also negotiate the ambiguous permanence in time of enwheelment and their bodily state after the injury. According to psychologists in the rehabilitation hospital, this ambiguity causes anxiety, and it calls for adjustment to a new approach to time called “contemporizar.”
3
Interestingly, contemporizing has two paradoxical meanings. The first one is primarily developed in the gym and entails focusing on the controllable aspects of the present as an anxiolytic strategy against an uncertain future: Contemporising means: If you are to be discharged a month from now, it is rational to worry about it and to start making plans, but now you may not know what will happen then, so try to focus on the day to day, on what you will do for the next sixty minutes. What is it? Stretching at the gym. Focus on that. (Psychologist 1, interview, September 2021)
While focusing on whatever activity they have for the next hour in the gym, people look up to the-body-of-others-that-is-potentially-like-their-own as a reference point for the ambiguous permanence of enwheelment (García-Santesmases and Sanmiquel-Molinero, 2022), and they focus on those who have overcome it. For some participants, the gym thus becomes a space that encourages ableist mythologies where overcoming enwheelment is conceived as a matter of “moral strength”: When it comes to this kind of injury, doctors (. . .) tend to say: “You are never going to walk again.” (. . .) This stimulates some people to overcome [impairment]: (. . .) “For fuck’s sake I’ve shut [the doctor] up and said, Look, I’m walking.” (. . .) Moral strength is crucial: without it, there is no effort. (Sue, CD, March 2020)
In contrast to being a space where “overcoming” mythologies that reinforce the instability of the enwheeled body flourish, according to Psychologist 2, the space of the gym operates as a bath of “hard realism” through which the person is “situated” as permanently disabled irrespective of their “will.” She notes that lockdown impeded this: Going [to the gym] and doing the exercises, finding the difficulties, (. . .) talking to other people and seeing that you are like them. . . . It is a bath of information that situates you, a bath of hard realism where you see that this is not a matter of will, that you are there giving it all and it does not change the injury. [During lockdown] our patients could not have this vital experience (. . .). This caused lots of patients to cling to unrealistic expectations for a long time. They thought that (. . .) their injury would improve when they got to go to the gym. (Psychologist 2, interview, July 2020)
Before lockdown, patients usually received external visits in the afternoon, right after they had finished their gym routine. If the gym is a crucial space for negotiating the permanence of enwheelment over time, Blanca’s narrative—which took place 1 year after the first lockdown, when external visits were allowed—illustrates how encounters with acquaintances “from before” in the hospital formative shell are crucial for negotiating the meaning of enwheelment: Now, friends (. . .) are coming to visit me (. . .). This experience is helping me prepare for when I go back home. (. . .) The first visual impact for them is to see me in the wheelchair. I can see it often overwhelms them, so I usually transfer from the wheelchair to a bench (. . .). It makes them more comfortable; they think: “She is like before.” (. . .) They say: “Doesn’t it bother you to be in a wheelchair?” (. . .) I, on the other hand, perceive it the other way round, I almost thank the wheelchair for keeping me active. (Blanca, CD, April 2021)
This extract illustrates that, in the context of these visits, the enwheeled subject must negotiate diachronotopic disruption: whether they are “a different person” (who is worse off) than before. Here, the enwheeled body-subject must manage the emotional crisis that enwheelment poses to others spatially: Blanca temporarily “dis-enwheels” herself to make people comfortable and be seen as “the same as before.”
Finally, before and after lockdown, people with an SCI could choose to attend a psychoeducation group, which took place once a week during gym hours. There, people who had been in the hospital in the past would sometimes give a speech whenever they visited the hospital for a check-up. Between June 2019 and September 2021, two different psychologists guided those sessions, one of whom has an SCI. This is how Blanca talked about the sessions led by her on the day of her discharge: I really liked the group space with [Psychologist’s name] and she helped me a lot with certain issues. (. . .) her testimony relieves you (. . .). When you leave the hospital, you think you are going to have to do rehabilitation all your life, you always look at the future from where you are now, but (. . .) a boy from Navarre came to the group (. . .) and told us that he does not lead that kind of lifestyle and (. . .) you see possibilities that you had not imagined. (Blanca, CD, June 2021)
Thus, the group acts as a mirror that displays what an enwheeled subject can do in the future (Papadimitriou & Stone, 2011, p. 2126). Importantly, such possible subjectivities need not resemble how one is in the immediate moment, which resonates with the second meaning of “contemporizing.” Paradoxically, besides focusing on the present to manage an anxiogenic future, contemporizing also entails invoking an implicitly better future as an anxiolytic in the face of an uncertain present circumstance: (. . .) because the present is a difficult moment. We have had many difficulties (. . .) contemporising means saying: (. . .) let’s not assume that your life from now on will be based on the situation you are living now. (Psychologist 3, interview, September 2021)
Interestingly, although it could be thought that not having had the opportunity to envision such possible futures during the pandemic had a major impact, the three psychologists I interviewed did not feel that this was the case. They considered that it was rather “able-bodied society” who, during the pandemic, had adjusted to the contemporizing attitude they promote in people with an SCI, which resonates with the “universalisation of crip time” (Samuels & Freeman, 2021, p. 246): I cannot see differences between patients [before and after the pandemic] I think the pandemic has helped us (. . .). We have approached death. We have approached illness. We have made an exercise in flexibility. “This is what we can do here and now, and we will see what we can do in the future.” (. . .) even though I predict that we will be the same as before in no time. (Psychologist 2, interview, September 2021)
The next section will explore synchronotopic disruption and how the pandemic affected it.
Synchronotopic Disruption: Mal/adjusting to the Outside From the Inside
As the spatial-temporal and relational rules that govern the parenthetical bubble-shell differ from those of “the outside world,” “discharge preparation,” a process of progressive adjustment to the outside space-time, is needed. On one hand, this process includes “weekend outings” and “urban outings” (weekly outings with a small group of inpatients led by the gym staff). In June 2019, Psychologist 1 informed me that the aim of “urban outings” was to get the person used to architectural and attitudinal barriers. Urban and weekend outings were suspended during lockdown. As of September 2021, when these outings resumed, one of the hospital physical trainers had “noticed that a lot of people lack street experience, even though the training they undertake here is now the same as before the pandemic.”
Sue and Blanca had the opportunity to undertake such outings. Their narratives illustrate that the “street experience” that some inpatients may have lacked was one of synchronotopic disruption: The feeling they call “the [hospital name] bubble” rings true to me (. . .). As opposed to the inside, the outside is insecure. When you leave the hospital, two things happen. First, you feel more insecure walking around. (. . .) Second, they stare at you. At the beginning it was like, “They are looking at me, they are looking at me.” Now (. . .) I don’t care. I’ve accepted that people will stare at me. (Sue, CD, March 2020) I’ve already noticed the change when I’ve gone out these last few weekends. In the street, a lot of things were happening so fast (. . .). Here, it’s very easy to predict everything. That makes your body get used to a biorhythm, and when that changes, boom! (. . .). I’m afraid of having to get used to new spaces that now feel so volatile (. . .). I’m going to be more stressed, attentive to the space. (Blanca, CD, June 2021)
These excerpts point to two major differences between the outside and the inside of the bubble that only become detectable when inpatients go outside. First, unlike inside, outside the bubble, the disabled body-subject must adjust to being constantly marked as an object “out of place” (Kitchin, 1998), deserving of constant stares that make it “dys-appear” (Imrie, 2004, p. 751). Second, inside the bubble, the built space is mostly adjusted to physically disabled bodies. They are expected to move safely and autonomously in predictable rhythms, so space and time also disappear for the disabled gaze. On the contrary, outside, space is often felt as insecure, and time is frenetic: this causes a permanent crisis that must be constantly adjusted to.
The second aspect of discharge preparation involves making “feeling of being at home” (Schillmeier & Heinlein, 2009, p. 222), since the (often enwheeled) disabled body’s “place” in the previous domestic space cannot be taken for granted. The fact that this must happen while they are still in the liminal phase of negotiating the permanence of enwheelment can generate maladjustments, which were exacerbated by the impossibility of weekend outings during the pandemic: Some people think that, by the time of discharge, they will be better off than they actually will, so they will not be able to sort some things [related to their home] out. Other people overestimate their future needs (. . .) they spend lots of money, and they get home, and they don’t have a home, they have a clinic (. . .). If you can spend a weekend at home (. . .) you get to see if you should move the furniture. (. . .) [Otherwise] you may find out you do not fit into the elevator once you are at home. . . . Not being able to experience this has a cost. (Psychologist 1, interview, September 2021)
In the following section, we will see how the intersection between ability, gender, and social class mediates the extent to which the process of “making a home” and returning to one during the pandemic has posed a crisis for the disabled body.
Back Home During Covid-19, out of the ‘Parenthetical Bubble-Shell’?
The advent of lockdown and the ensuing shutdown of two rehabilitation hospital units meant that many people had to leave hospital before their discharge date. This rushed their rite of passage into the community, altering the precarious adjustment process between their “not-yet-rehabilitated” bodies and their homes. One of the professionals of the hospital service that supports people in the transition to home recounted their feeling of “losing their place” in the hospital bubble: We really supported all the people who were discharged from hospital in a very hasty manner. (. . .) They went home without the necessary adjustments, without health education, without being linked to primary care, in a context where the primary care system was totally knocked out (. . .). There was also a lot of anger and a lot of complaints (. . .). This idea of “getting a fair treatment” was quite hard to handle (. . .). Maybe it’s just a personal sensation, but I feel that those who did not claim [treatment after lockdown] lost out. (Occupational Therapist 2, interview, September 2021)
Josep Maria was discharged a month before lockdown. The fact that he owned his flat and had a good economic situation allowed him to adjust his bathroom before going home. However, it was impossible to adjust the kitchen space to an enwheeled body. He assumed that the relatives who were living with him would be willing to take care of meal preparation among other needs, or that he would be able to eat in restaurants. Lockdown put him in an unexpected crisis as it prevented the precarious assemblage between his body, his flat, the restaurants where he planned to eat and his relatives from continuing to make his independence possible. The crisis was sorted out through a highly gendered re-adjustment (Winance, 2006), in which his female partner rushed to take care of him: My son [and his partner] suddenly moved out on 7 March [2020] (. . .). They didn’t think that they were going to shut everything down and I wouldn’t have anything to eat. (. . .). Since lockdown was already being talked about, I told my partner to move here straight away. (. . .) Thanks to her, I have been able to get through lockdown without any problems. (. . .) She has been here (. . .) taking care of the shopping, making the daily menus, etc. From day 1, I’ve been going to the shops with her everyday. (Josep Maria, CD, June 2020)
Not all participants could go out every day during lockdown like Josep Maria did. Because of imminent lockdown, Participant 4 returned to an un-adjustable flat with no lift because it was rented and he had no money to move elsewhere. This inaccessible assemblage made him dependent on his female partner not only financially, but also concerning his body: I should adjust the toilet (. . .). On the one hand, this is not possible because it is a rented flat. On the other hand, because of the money (. . .). Right now, I just need help in the shower and that’s it. My wife helps me. (. . .) I am worried because I have a 10-year-old and I should bring money home (. . .). Now, my wife is the one who works. (. . .) I don’t have a lift and I can’t go down to the street. (. . .) I can’t live here like this, because I can’t move around. When my wife starts working [after lockdown], I won’t be able to go out. I won’t be able to take the child to school. (. . .) I haven’t left the house since I came back from the hospital. (. . .) I’ve been stuck at home when everyone else had to be. This has made it much more bearable. It’s not the same as being locked up alone and seeing everyone in the street. (Participant 4, CD, June 2020)
The intersection between ability and social class led to a particularly compressed personal chronotope for Participant 4 back home. Unlike Josep Maria, he could not afford to adjust his flat or move elsewhere and thus was “locked in” at home with little opportunity to go out and act as the “male breadwinner” he used to embody. Interestingly, his current personal chronotope is said to be unsustainable over time because of the high degree of immobilization it entails, and because of the dependence on the female partner generated by and compensating for inaccessible spaces. However, the excerpt also highlights that, to date, this immobility and dependence had not been experienced as unlivable precisely because it did not represent a major synchronotopic disruption with respect to the rest of the world.
The intersection between gender and ability emerges when comparing Participant 4 and Josep Maria’s stories, who got through the pandemic thanks to their female partners, with that of Participant 6. She also returned to a rented flat that was unadjustable to her body shortly before the second pandemic wave: My husband supports me now and it’s not ok. (. . .) The rent has been going up for two years now. This is wrong because all he does is work and help me: he has no life. (. . .) I wanted to get divorced, but (. . .) where am I supposed to go with nothing? (. . .). It’s not normal (. . .) that they let me go home with a man I was already thinking of divorcing three days before my injury. What if it was a man who mistreats you? (. . .). They don’t keep an eye on you either, they don’t call you. (. . .) it’s not right for me, and it’s not right for him either. (. . .) As I sleep in the living room and he sleeps in the bedroom, it’s as if we were flatmates. (Participant 6, CD, April 2021)
Participant 6 noted how the transformation of the couple’s relationship into a power imbalanced flatmate/caretaker relationship occurred in part because it was impossible to adjust the bedroom space, which forced her to sleep in the living room. As opposed to her male counterparts, for her, being dependent on her male partner was intolerable. She also raised the risks that such dependence and the impossibility of finding another home entail in terms of gender-based violence.
Finally, the pandemic has also contributed to a greater compression of the personal chronotope of other participants, reducing their ability to move both physically and in terms of their “social place” as officially “disabled people.” The liminal state of waiting in which the people who returned home during the pandemic were left was not limited to waiting for resuming their treatments, but also for the acquisition of their “place” as officially disabled, which hindered their mobility through space-time (e.g., preventing them from moving by car because they did not have a disabled parking card). The pandemic also delayed the acquisition of mobility devices. In his account, Participant 1 described how his discharge from the hospital did not mean his immediate exit from the hospital bubble-shell, partly because of fear of becoming infected and partly because the manual wheelchair he left the hospital with was unsafe (he had several falls with it) and did not allow him to go very far from the hospital apartment complex he now lives in. He thus had to adjust his routes to his assemblage with a manual wheelchair. In September 2020, he was considering buying a motorized handbike: I feel like changing my wheelchair because I have a bit of a grudge against mine after the crash I took [going down a kerb]. (. . .) I have a neighbour who has the [handbike brand] and he’s gone as far as the mouth of the [local river]. I am so envious! (. . .) My friends told me to go to Madrid to a party, but I haven’t gone. I’d like to, but I think that I would need the handbike to take that step. It will give me much more movement and freedom. Plus, there’s the COVID thing. (. . .) I try not to go out because of the bug. (Participant 1, CD, September 2020)
Nine months later, Participant 1 still did not have his handbike, and it made it difficult for him to get to the COVID vaccination site. Interestingly, his envied neighbor offered to tow him with his handbike to get to the appointment. He accepted despite knowing that such a strange enwheeled assemblage would be marked as “out of place” by the able-bodied gaze: Well, vaccination has been a bit of a challenge. (. . .) They gave [my neighbour with a handbike] the same vaccination post as me (. . .). He said, “Great, let’s go together.” “Listen, the thing is that I’m so slow with my wheelchair.” He said, “Let’s do this: you hold on to the back of my chair and I’ll take you with my handbike.” I said: “Come on, we’re going to be on TV!.” “Don’t worry about it!.” (. . .) I focused on the fact that we did 900 metres on one go, but I’m sure we were a hell of a spectacle. (Participant 1, CD, May 2021)
This extract highlights that the disabled body-subject does not passively assume the spectacularised out-of-placeness to which dis/ableist stares condemn to. Instead, counternormative mutually supportive assemblages among enwheeled peers are crucial to thrive in pandemic times of crisis.
Concluding Remarks
In this article, I have explored the notion of rehabilitation hospitals as “parenthetical bubble-shells.” That is, liminal space-times where newly disabled people experience two kinds of chronotopic disruption and adjust to new ways of approaching space and time: enwheelment and contemporization. Notably, both synchronotopic and diachronotopic disruptions only become perceptible when people encounter the parenthetical bubble-shell’s “before” (e.g., acquaintances who visit them) and its “outside” (e.g., weekend and urban outings). Lockdown drastically altered the hospital’s regime of boundedness and permeability (Street & Coleman, 2012), thus altering the opportunities for the disabled body to develop an enwheeled and contemporizing subjectivity before exiting the hospital.
The findings expand the conceptualization of enwheelment as a liminal approach to space that develops in the rehabilitation setting and extends beyond such facilities. The wheelchair is an “ambivalent” (Gaete-Reyes, 2015, p. 357) or “liminal device” (Papadimitriou, 2008, p. 694)because it is understood by disabled people as enabling while ableist imaginaries associate it as a “barrier” to abilities. Notably, enwheelment is also liminal because the disabled subject must negotiate, in the context of several hospital socialization spaces that were radically altered during the pandemic, its ambiguous permanence, as well as whether it entails diachronotopic disruption (becoming someone/something else). In fact, the pandemic expanded the liminality that enwheelment entails by making them cling to ableist expectations of overcoming, as well as by delaying the acquisition of several social and physical mobility devices associated with wheelchair use, thus restricting mobility and citizenship for disabled people (Gaete-Reyes, 2015). Just as class and gender determined for whom the world became a liminal space that “ended at the sidewalk” during the coronavirus crisis (Bell, 2021), these axes of difference also modulated the extent to which enwheelment posed a permanent synchronotopic disruption after discharge from the parenthetical bubble-shell.
I have also shown that enwheeled subjects are not mere victims of dis/ableist arrangements. Rather, they actively seek to form new assemblages that sustain their independence, sometimes in ways that reflect gender and class inequalities. Thus, we should not assume a powerless, homogeneous, and universal disabled subject, and future studies should further examine the complex and situated intersections that throw some disabled people and those who sustain their independence into compressed spaces that create permanent and naturalized crises in the so-called “new normalcy” after the pandemic (Danylevich & Patsavas, 2021).
In the same vein, the present work also urges us to problematize the so-called “universalization of crip time” during the pandemic (Samuels & Freeman, 2021, p. 246). Psychologists in the present study referred to this as the temporary universalization of “contemporization.” Like enwheelment when it comes to space, contemporizing can be understood as a liminal approach to time, since it implies carrying out two apparently paradoxical operations with future and present in times of crisis. Since contemporization used in this sense seems to be a local phenomenon, future studies should also explore whether it is also encouraged in other locations. Notably, the fact that such a liminal approach to time is considered unsustainable for the able-bodied subject should remind that it is also unsustainable for disabled people. Indeed, liminality is an insecure space-time that simultaneously poses an opportunity for the collective production of a better new normalcy. This should not imply disavowing temporary able-bodiedness but creating the spatial-temporal conditions so that embodying disability does not condemn us all to permanent crisis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Ministerio de Ciencia, Innovación y Universidades (Grant FPU17/01545). I also thank the people who have participated in this research for their time and dedication.