
Abstract
Introduction
Natalizumab is a humanized monoclonal antibody raised against human α4-integrin which is currently approved as a monotherapy for relapsing–remitting multiple sclerosis (RRMS) patients with high disease activity. In two double-blind, placebo-controlled trials (AFFIRM and SENTINEL), natalizumab has been shown to slow the progression of disability in RRMS patients and to reduce the number of new or enlarging T2 hyperintense and gadolinium-enhancing magnetic resonance (MR) lesions. 1 – 2 Apart from these primary endpoints, several post hoc analyses of data from these trials have provided further insights into benefits of natalizumab therapy: Significantly more natalizumab-treated patients could be defined as free of clinical and radiological disease activity. 3 In another analysis, reduction of visual function was evaluated using data from both trials. Visual function was measured by Sloan low-contrast letter acuity chart, 4 and natalizumab-treated patients were found to have a reduced risk of visual loss. 5 This analysis underlines the fact that a single parameter cannot capture the complexity and heterogeneity of multiple sclerosis (MS) and that different outcome measures can be useful in different clinical situations. The most widely used Expanded Disability Status Scale, for example, includes eight different functional systems – one of them represents the visual system. At scores higher than 4.0, however, this composite score is mainly determined by the pyramidal system (ability to walk). 6 The Multiple Sclerosis Functional Composite (MSFC) is another composite score measuring lower as well as upper extremity function and cognitive ability. Natalizumab treatment was recently shown to reduce MSFC progression in the patient collectives of these trials. 7
A number of diagnostic tools are applied in clinical practice, including clinical evaluation, magnetic resonance imaging (MRI), cerebrospinal fluid (CSF) studies and neurophysiological methods. Among these, evoked potentials (EP) are widely used in the functional assessment of visual (VEP), sensory (SEP) and motor (MEP) pathways. Repetitive evaluation of EPs can be useful for the assessment of disease progression as they correlate with disease disability. 8 As described above, treatment effects of natalizumab on Expanded Disability Status Scale, low-contrast letter acuity chart and MSFC could already be demonstrated – parameters which do in part include the visual, sensory or motor system. Thus far, the direct impact of natalizumab on functional parameters of nerve conduction assessed by evoked potentials has not been investigated.
Patients and methods
Patients
All RRMS patients included in this study were seen at the MS centre of the University of Wuerzburg from 2006 to 2009. Forty-four patients with clinically definite MS according to the McDonald criteria 9 were consecutively included in this study when they fulfilled the following inclusion criteria: patients underwent detailed physical and neurological examination (including Expanded Disability Status Scale) as well as multimodal EP, i.e. VEP and/or SEP and/or MEP, 1 year prior to natalizumab treatment and were followed for at least 6–12 months during treatment. All recordings were done for diagnostic purposes only. Forty out of 44 patients had previously received at least one other immunomodulatory agent, while four patients (9%) were treatment-naive prior to natalizumab therapy.
Evoked potentials
All electrophysiological examinations were performed on a commercial PC-based neurophysiological recording system (Multiliner, Toennies Division of Viasys Healthcare, Höchberg, Germany) as described earlier. 10 Filters and other technical settings were chosen according to established guidelines. 11
Visual evoked potentials
In brief, monocular visual stimulation was performed using a pattern-reversal checkerboard screen (14 × 10 checks of 1°, reversing frequency of 2/s; mean luminance 20 cd/m2 with a contrast of 99.5%). A needle recording electrode was placed at Oz′ (5 cm above the inion) and the reference at Fz. An average of two to three trials (200 patterns each) were analysed according to laboratory reference values (upper limit P100/N2 latency: 120 ms; lower limit for P100 (P1-N2); amplitude, lower limit: 5 mV). A W-shaped P100 deformity was rated abnormal when the difference between the two positive peaks exceeded 10 ms. Normal limits were 60% for side differences in amplitude (calculated from the highest amplitude) and 7.0 ms for differences in latency.
Somatosensory evoked potentials
Tibial nerve stimulation was performed at the ankle with surface electrodes at 1.5 times motor threshold as described earlier 10 (stimulation rate: 3/s, pulse duration: 100–200 µs). Needle recording electrode was positioned at Cz, reference electrode at Fz, and 200 responses were averaged (two runs). Latencies were analysed from the beginning of the stimulus artefact to the P40 peaks (upper limit: 43.9 ms for 175 ± 5 cm body height [mean ± standard deviation]). The limit was adopted for deviated body lengths by 0.17 ms/cm. The lower normal limit of the P40 amplitude was 0.3 mV and less than 50% reduction compared with the highest P40 amplitude on either side.
Magnetic motor evoked motor potentials
Magnetic motor cortex stimulation was performed in accordance with standard protocols. 10,11 A circular high-performance coil attached to a Magstim 200 stimulator (Micromed, Freiburg, Germany) was positioned over the vertex for stimulating the leg representation of the motor cortex and was recorded using surface electromyographic (EMG) electrodes from both anterior tibial muscles. L5 lumbar roots were stimulated by placing the coil over the upper lumbar region (three successive stimuli each). The shortest latencies between the trigger signal and the MEP response were accepted. Difference between cortical and radicular stimulation was calculated as central motor conduction time (CMCT; upper limits: 17.8 ms ≥175 cm body length; 19.3 ms <175 cm). Side differences in latency of 2.0 ms and less than 50% difference between the MEP amplitudes on either side were scored as abnormal. In addition to amplitude and latency criteria, dispersed MEP with four or more baseline crossings on cortical stimulation were also rated abnormal.
Scoring and analysis of EP data
The primary goal of this study was to evaluate the influence of natalizumab treatment on electrophysiological measures in RRMS patients. Furthermore, we correlated alterations in evoked potentials (VEP, SEP, MEP) with the Expanded Disability Status Scale as a general marker for permanent disability.
Therefore we defined an ordinal EP score in which each abnormal result scored one point (e.g. abnormal latency and/or amplitude on either side). Sum scores of each electrophysiological measure were calculated from absolute values. The range of scores was: 0 (no pathological value on both sides), 1 (pathological value on one side, decrease in amplitude or abnormal latency), 2 (pathological value on one side, abnormal amplitude and latency or pathological value on both sides, latency or amplitude), 3 (pathological value on both sides, one side with abnormal latency and amplitude plus one side with abnormal amplitude or latency) and 4 (pathological values on both sides assessed). These values were followed and compared between time before treatment initiation (t = −1 to t = 0) and time after natalizumab initiation (t = 0 to t = +1) in the patient cohort. Further, these sum scores were correlated with the Expanded Disability Status Scale of the patients over time.
Statistics
Differences in Expanded Disability Status Scale and EP sum scores were compared by two-tailed t-test or Mann–Whitney U-test. Spearman’s rank correlation coefficients were calculated and compared by two-tailed t-test. All data are presented as mean ± standard error and significance was assumed for p < 0.05.
Results
Patient characteristics

EDSS: Expanded Disability Status Scale, RRMS: relapsing–remitting multiple sclerosis.
We generated a sum score to quantify the changes observed (for calculation see Patients and methods section). We found that VEP sum scores showed an improvement in 33% of patients after 6–12 months (from t = 0 to t = +1) of natalizumab treatment, 41% remained stable (no changes in the sum scores) and 26% deteriorated. This was in clear contrast to the time previous to natalizumab initiation, when only 9% showed VEP amelioration before treatment onset, but 81% remained stable or deteriorated (from t = −1 to t = 0). These data indicate that treatment with natalizumab was associated with a significant proportion of patients showing an amelioration in the VEP sum score (p = 0.041; see Figure 1A).
Development of EP sum scores before and under natalizumab therapy. EP sum scores were assessed on a qualitative scale (0: no pathology on both sides; 4: abnormal latencies and amplitudes on both sides) and change was described as ‘worsened’ (positive change in sum score ≥1), ‘no change’ or ‘improved’ (reduction in sum score ≥1), 1 year before natalizumab therapy and 6–12 months after therapy onset. (A) VEP before (n = 22) and after (n = 27; p = 0.041) natalizumab. (B) SEP before (n = 19) and after (n = 19; p = 0.027) natalizumab. (C) MEP before (n = 17) and after (n = 21; p = 0.060) natalizumab. EP: evoked potential, MEP: motor evoked potential, SEP: somatosensory evoked potential, VEP: visual evoked potential.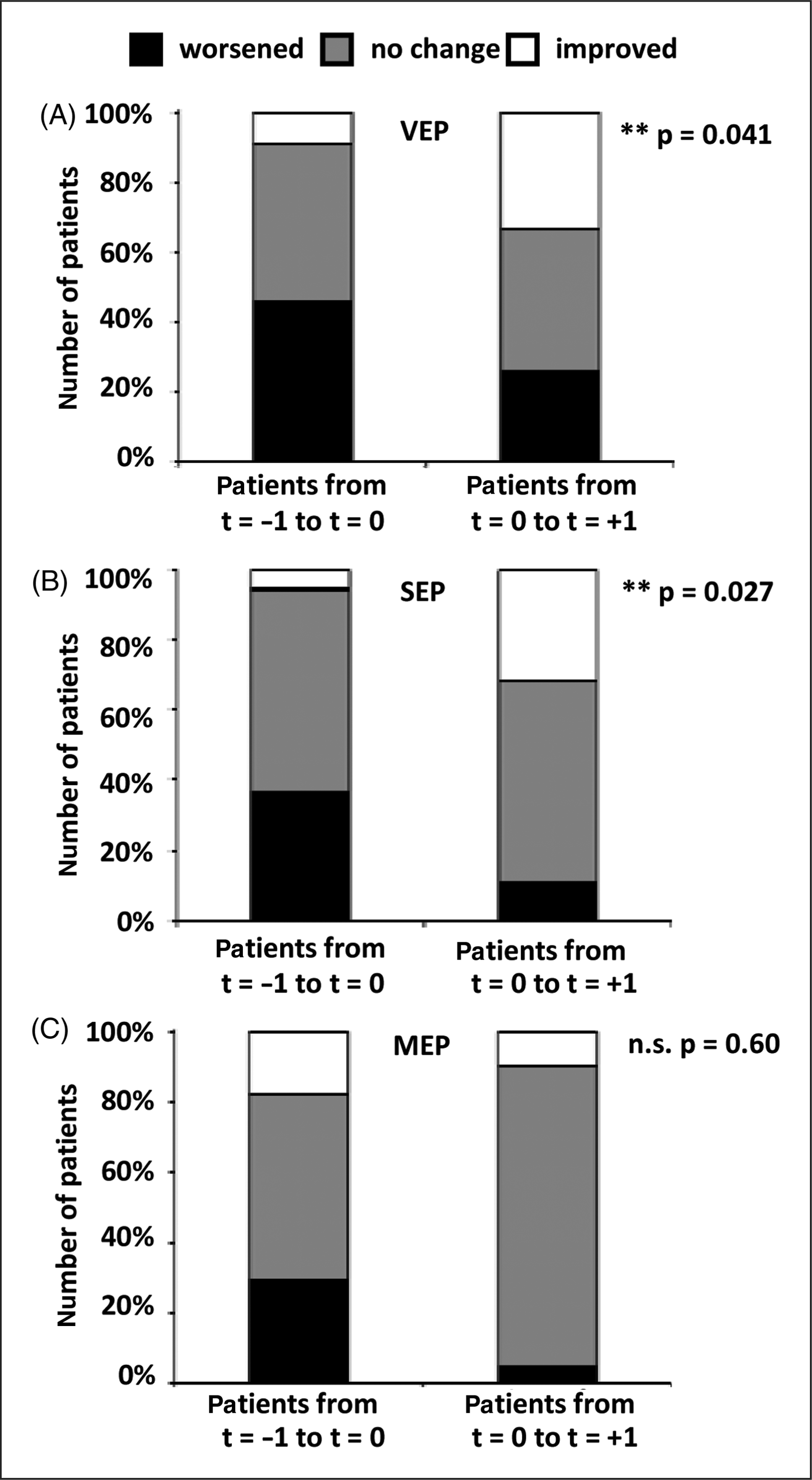
Similar results were found for SEP recordings (p = 0.027). While 32% of the treated patients showed beneficial effects at t = +1, only 5% of the same patients showed improvement prior to treatment. In 11% we found SEP worsening under natalizumab treatment whereas 37% of the patients showed SEP deterioration before treatment (Figure 1B). In 58% of the patients we found no significant SEP changes over time. Although benefical effects of natalizumab on functional measures of nerve conductance could be captured by VEP and SEP recordings, no significant effects were seen with MEP. Under therapy only 10% of the patients showed an improvement (t = +1) versus 18% at t = 0. MEP worsening could be detected in 5% of the treated patients (t = +1) versus 29% at t = 0 (p = 0.60; Figure 1C). In about 70% of the patients no MEP changes were observed over the study period.
As mentioned above, our sum score consisted of pathological latencies and amplitudes assessed for both sides and thus cannot discriminate whether natalizumab has a preferred effect on either amplitude or latency changes. Detailed analysis of the sum score compositions showed that changes in VEP scores relied more on amplitude changes than on latency (amplitude points: 61%, latency points: 39%), while SEP and MEP sum scores consisted nearly equally of amplitude and latency pathologies. These effects were not significant, however. Thus, natalizumab treatment had no preferred effect, as the contribution of amplitude and latency to the sum score compositions was unchanged on natalizumab compared with before.
The Kurtzke Functional Systems (FS) and Expanded Disability Status Scale 12 remain the most widely used scoring systems to assess neurological disability in MS. 13 In our cohort, Expanded Disability Status Scale 12 months prior to treatment initiation (t = −1) was 2.77 ± 0.03 (n = 44). At the timepoint of treatment initiation it was 3.40 ± 0.03 (t = 0; n = 44; p = 0.03). On natalizumab treatment the score again dropped significantly (3.02 ± 0.04 at t = +1; n = 41; p = 0.02; see Table 1).
Changes in EP in the natalizumab group were compared with changes in Expanded Disability Status Scale score. There was a significant correlation for VEP (R = 0.67; p = 0.001) and MEP (R = 0.49; p = 0.03), which was not demonstrable for SEP (R = 0.22; p = 0.36; Figure 2). Of note, correlation of EP score changes and Expanded Disability Status Scale changes during the pretreatment phase was generally weaker (VEP: R = 0.21; SEP: R = 0.14; MEP: R = 0.28) and not statistically different.
Correlation between EDSS and EP sum scores. Changes in EDSS after natalizumab treatment were described as ‘worsened’ (positive change in EDSS ≥1 for 6 months), ‘no change’ and ‘improved’ (reduction in EDSS ≥1 for 6 months), and EP development of each patient is shown in the diagrams. (A) VEP (R = 0.67; p = 0.001). (B) SEP (R = 0.22; p = 0.36). (C) MEP (R = 0.49; p = 0.03). EDSS: Expanded Disability Status Scale, EP: evoked potential, MEP: motor evoked potential, SEP: somatosensory evoked potential, VEP: visual evoked potential.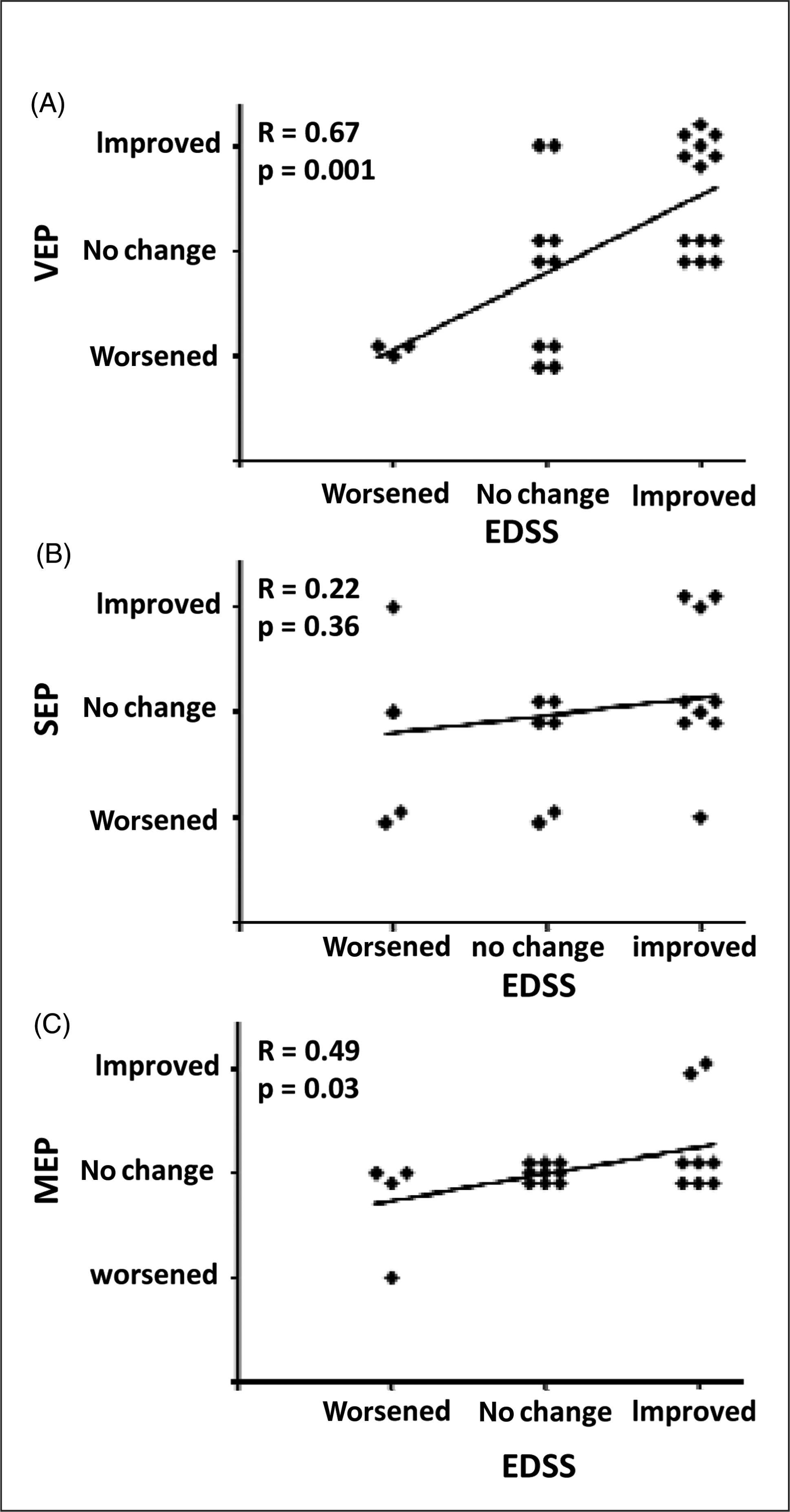
EP changes and EDSS functional scores
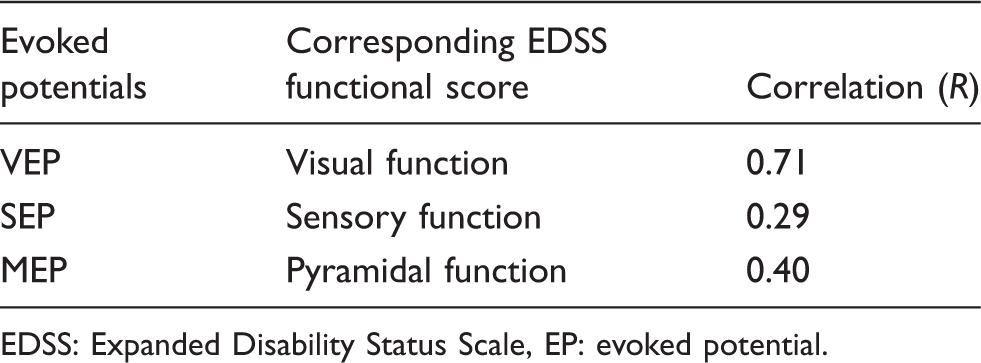
EDSS: Expanded Disability Status Scale, EP: evoked potential.
In summary, our results show that EP recordings (VEP, SEP > MEP) can be useful tools to demonstrate effects of immunoselective treatment with natalizumab on a functional level. Natalizumab treatment resulted in an increased number of patients showing stable or ameliorated results in the visual and somatosensory systems. Moreover, VEP and MEP results are significantly correlated with changes in the Expanded Disability Status Scale over time.
Discussion
Extensive clinical trial data as well as several years of clinical experience underline the therapeutic benefit of natalizumab in reducing clinical disease activity at different levels – despite rare but severe side effects, such as progressive multifocal leukoencephalopathy (PML). 14 The influence of natalizumab therapy on the functional capability of nervous conduction as assessed by evoked potentials has not previously been investigated. Previous studies for other approved medications have already revealed an improvement of MEP under interferon beta-1a 15 and VEP under interferon beta-1b 16 treatment in RRMS patients. In contrast, no difference was found in a small study for VEP under interferon beta-1a therapy. 17 Furthermore, the diagnostic as well as prognostic value of serial evoked potential measurements underlines their clinical usefulness for monitoring disease development. 10,18 – 20
In our study we investigated EP developments under natalizumab therapy. In our cohort of 44 patients we demonstrate that an increased number of patients showed stable or ameliorated VEP and SEP during 1 year after initiation of natalizumab treatment. It seems reasonable to suggest that treatment effects of natalizumab are caused by its immunomodulatory effect on T lymphocytes, rather than by a direct effect on nerve conduction or remyelination, as it showed equal effects on amplitude and latency changes. The reasons for a lack of effect of natalizumab on motor evoked potentials, however, remain unclear. Apart from intrinsic limitations of this study (retrospective, limited patient number), differences in the recovery of different inflammatory stimuli between distinct tracts may present a reasonable explanation. Especially the assessment of MEP, albeit largely representing the functional capability of the pyramidal tract, has various contaminating factors, thereby influencing both the sensitivity and the specificity for ‘motor conduction’. Thus, in a limited number of patients with heterogeneous affection of the pyramidal tract, it is not unexpected that this readout did not show uniform results.
Another major result of this study is the fact that VEP and MEP are significantly correlated with changes in the Expanded Disability Status Scale on natalizumab treatment. Differences in correlations between Expanded Disability Status Scale in general and the corresponding Expanded Disability Status Scale functional scores might be due to limitations of the Expanded Disability Status Scale: at scores higher than 4.0 (mean Expanded Disability Status Scale at t = 0 was 3.40 in our collective), this composite score is very much determined by the pyramidal system (ability to walk). Developments in the visual and sensory systems may therefore be relatively underestimated at higher Expanded Disability Status Scale scores. This could explain the higher correlation coefficients which we obtained for VEP/SEP and Expanded Disability Status Scale functional scores. However, the general tendency and statistical significance were comparable to the Expanded Disability Status Scale data.
In summary, our study demonstrates that natalizumab is able to stabilize and to improve the functional capability of nervous system conductions (VEP and SEP). Evoked potentials might therefore be considered a useful tool in order to evaluate drug effects in clinical practice. However, the analysis of EPs in a larger group of patients under prospective conditions is required.
Footnotes
Acknowledgements
We would like to thank Karl-Heinz Reiners and Klaus Toyka for proof-reading of the manuscript and valuable discussions.
Funding
S.G.M. has received honoraria for lecturing and travel expenses for attending meetings and has received financial research support from Bayer, Biogen Idec, Sanofi-Aventis, Bayer Schering, Merck Serono and Teva. H. Wiendl has received funding for travel and speaker honoraria from Bayer Schering Pharma, Biogen Idec/Elan Corporation, Sanofi-Aventis, Merck Serono, and Teva Pharmaceutical Industries Ltd.; has served/serves as a consultant for Merck Serono, Medac, Inc., Sanofi-Aventis/Teva Pharmaceutical Industries Ltd., Biogen Idec, Bayer Schering Pharma, Novartis, and Novo Nordisk; and receives research support from Bayer Schering Pharma, Biogen Idec/Elan Corporation, Sanofi-Aventis, Merck Serono, and Novo Nordisk.
Conflict of interest statement
S.B., C.S. and K.G. declare no conflict of interest; other authors as above.