
Abstract
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system (CNS) which often leads to neurological disability. 1,2 Measuring disease progression in MS with sufficient accuracy and to be able to predict individual patient prognosis is a major challenge. 3 There is lack of a reliable prognostic marker in MS, especially for those patients with relapsing episodes of neurological dysfunctions who are generally those eligible for disease-modifying treatment. The new drugs with higher efficacy but potentially serious side effects increase the need to carefully select the most suitable treatment for each patient. Finding a reliable prognostic marker for the patients with MS would therefore be of importance. 4
Many attempts have been made to identify a prognostic marker for MS. The most reliable marker so far might be the elevated levels of neurofilament light in cerebrospinal fluid (CSF) collected at diagnostic lumbar puncture. This marker seems to be associated with an unfavourable prognosis and has been suggested as a prognostic marker in early relapsing–remitting MS (RRMS) 4 reflecting neuron/axon damage. 5
With regard to markers for inflammatory aspects of MS a large number of other studies have so far have been focused on characterization and involvement of T cells in the autoimmune attack to the CNS and the possibility to use their related mediators as biomarkers or prognostic marker for MS. 6 – 8 However, a role of B cells in MS pathogenesis has been suggested by the presence of oligoclonal immunoglobulin bands (OCBs) in the CSF that represent a hallmark of MS. 9,10 The cellular B-cell response, as measured in the CSF, was clearly more pronounced in acute inflammation (i.e. in patients with clinically isolated syndrome (CIS) suggestive of MS and RRMS) than in chronic progressive MS or in individuals with other neurological diseases (ONDs). In addition, CSF B cells were correlated with markers of acute brain inflammation such as high numbers of T2 lesions shown by magnetic resonance imaging (MRI), the presence of gadolinium (Gd)-enhanced lesions shown by MRI, the total number of CSF cells, intrathecal IgM and IgG synthesis and intrathecal MMP-9 and CXCL13 production, indicating a direct involvement of B cells in acute brain inflammation. 11 In concordance with this a recent phase II clinical trial, depleting the number of B cells has shown efficacy in MS. 12
MS disease activity can be detected by MRI using Gd to enhance the lesions, a measure of disruption of the blood–brain barrier with associated infiltration of leucocytes from the blood. 13 Leucocyte recruitment is tightly regulated and involves sequential interactions between adhesion molecules, chemotactic factors (chemokines) and chemokine receptors. 14 B cells in CSF from patients with MS and neurological control subjects express the chemokine receptor CXCR5. 15 The CXCR5 ligand CXCL13, the most potent B-cell chemoattractant, is evident in active MS lesions and its concentration is elevated in CSF from patients with MS. 11,16,17 CXCL13 in the CSF of MS patients was correlated with the presence of B cells, plasma blasts and T cells. 16 In human peripheral blood the source of CXCL13 is follicular dendritic cells, 18,19 but in the CNS it is expressed by cells having macrophage morphological features in the perivascular, inflammatory lesions and in scattered parenchymal cells. 16
CXCL13 was recently demonstrated to be up-regulated in pooled CSFs from patients with Lyme neuroborreliosis, but not in patients with non-Lyme meningitis or other inflammatory neurological disorders. It was therefore suggested as a possible early diagnostic marker in acute Lyme neuroborreliosis. 20,21 However, elevated levels of CXCL13 are also evident in CSF during MS relapses, 17 neurosyphilis, 22 herpes encephalitis and Epstein–Barr virus encephalitis (present study) indicating that CSF CXCL13 is thus not a disease-specific diagnostic marker. Elevated serum levels of CXCL13 have also been reported in several human diseases, as reviewed by Festa and colleagues. 23 It is thus very important to determine whether specific viral, bacterial or fungal agents underlie a neurological disorder or a non-infectious process early in the course of a disease.
CXCL13 was recently considered as an important prognostic marker in CIS and its level was reported to predict CIS conversion to MS. 24 The aim of the present study was to measure the CSF concentration of the B-cell chemokine CXCL13 and to determine its relationship with MS disease activity. If correlated, it could be employed as a reliable biological prognostic marker for prediction of the relapse rate years after disease onset in patients with RRMS. CSF from patients with CIS suggestive of MS, primary progressive MS (PPMS), and secondary progressive MS (SPMS) were also included. CSF samples from individuals with OND, either with or without signs of inflammation or viral/bacterial infections, and from healthy subjects were used as controls.
Subjects and methods
Demographic data of the patients with multiple sclerosis, clinically isolated syndrome and controls
Age (in years) refers to age at sampling time point.
Disease duration (in years) refers to years from disease onset to the diagnosis.
The number of MRI lesions corresponds to the brain MRI (not spinal cord MRI).
CIS: clinically isolated syndrome, CSF: cerebrospinal fluids, EDSS: Expanded Disability Status Scale, iOND: other neurological diseases with inflammation, MS: multiple sclerosis, N/A: not available. MRI: magnetic resonance imaging, OND: other neurological diseases, PPMS: primary progressive MS, RRMS: relapsing–remitting multiple sclerosis, SPMS: secondary progressive MS.
Study of cerebrospinal fluid samples
CSF samples were centrifuged immediately after sampling to isolate the cells and larger particles and stored frozen at −80°C until analysis. CXCL13 levels were measured using commercially available ELISA kits (Quantikine; Human CXCL13/BLC/BCA-1; R&D Systems, Abingdon, UK) according to the manufacturer’s instructions. Measurements were performed in duplicates using 50 µl undiluted cell-free CSF.
Statistical analysis
Differences in levels of CXCL13 in patients with MS and controls were analysed using either the non-parametric Kruskal–Wallis and Dunn’s post-test or the non-parametric Mann–Whitney t-test. Correlations between CXCL13 and quantitative clinical measures, genders and ages were analysed using Spearman’s rank test and linear regression for curve fit (GraphPad Prism 3.0; GraphPad Software, Inc., San Diego, CA, USA).
Results
CXCL13 in clinically isolated syndrome, multiple sclerosis and controls
The concentration of CXCL13 protein was determined in cell-free CSF from CIS (n = 79), MS (n = 387), OND (n = 181), iOND (n = 153), viral/bacterial infections (n = 23) and healthy subjects (n = 14) using enzyme-linked immunosorbent assay (ELISA). Apart from infectious conditions, CXCL13 levels were generally higher in the MS cohort compared with the other controls (Figure 1A). When comparing CXCL13 within subgroups of MS, including CIS, the levels of CXCL13 were much higher during clinical relapses compared with the RRMS during clinical remission, PPMS, SPMS and CIS (Figure 1B). However, the majority of samples from individuals with viral/bacterial infections had far higher CXCL13 concentrations than the inflammatory condition, MS and controls (Figure 1C). Examples of viral/bacterial infected samples included are Epstein–Barr virus infection, herpes encephalitis, borreliosis and meningitis.
CXCL13 in clinically isolated syndrome (CIS), multiple sclerosis (MS) and controls. (A) CXCL13 levels were higher in the MS cohort compared with the other groups. (B) CXCL13 was increased during clinical relapses (n = 52) when compared with clinical remission (n = 271), primary progressive MS (PPMS; n = 24), secondary progressive MS (SPMS; n = 40) and CIS (n = 79). (C) Samples taken from individuals with viral/bacterial infections (n = 23) rather than inflammation had much higher CXCL13 levels than in all MS (n = 387). Significance was determined using a Kruskal–Wallis test followed by a Dunn’s post-hoc test. *p < 0.05; **p < 0.01; ***p < 0.001.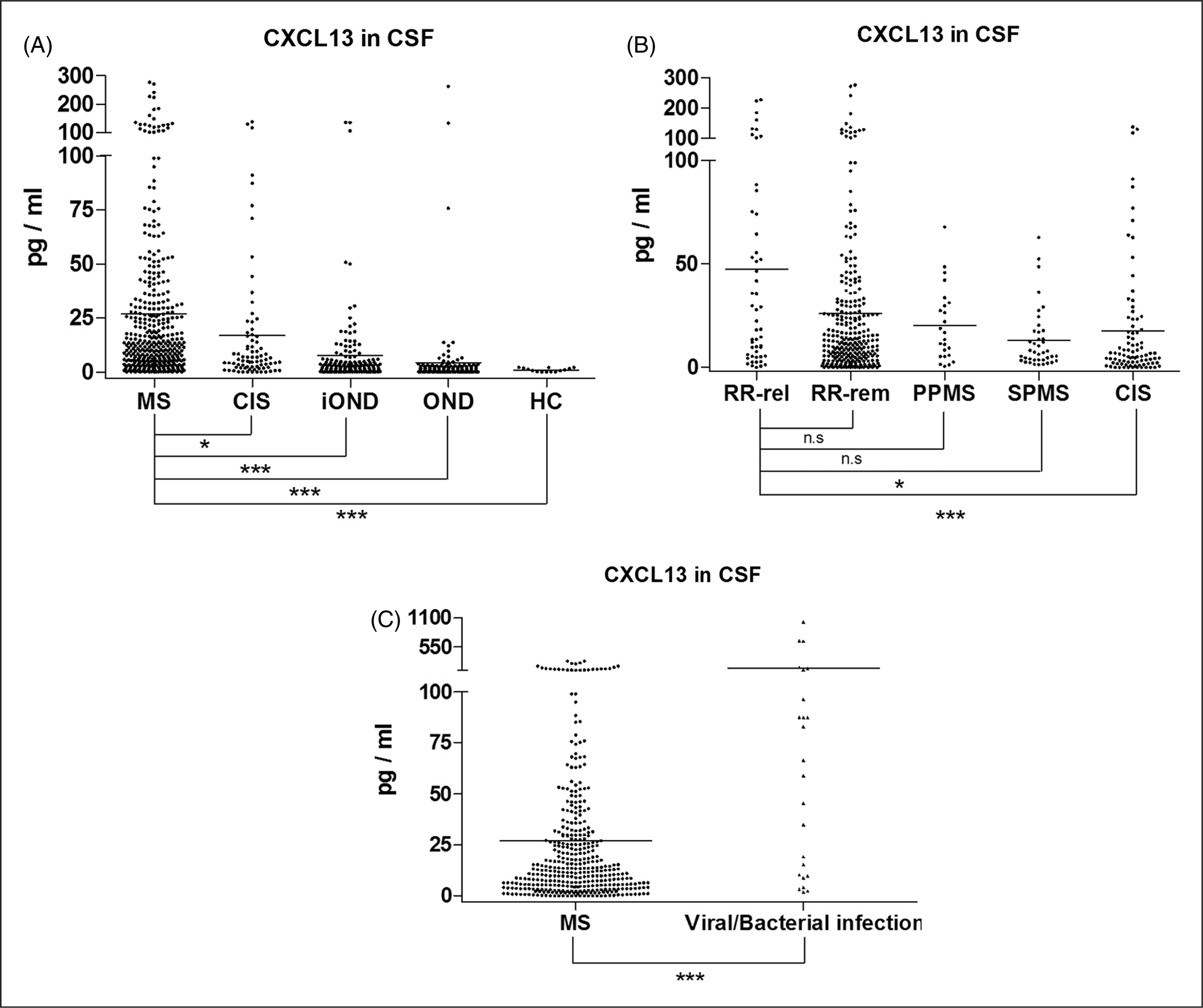
CXCL13 levels are related to relapse rate, Expanded Disability Status Scale and number of lesions detected by magnetic resonance imaging
The levels of CXCL13 were analysed in RRMS patients (n = 323) and their relapse rates were analysed by dividing the number of relapses by the number of years starting from the year when they were clinically diagnosed for definite MS until their latest score. Patients with the highest relapse rates exhibited the highest CXCL13 concentrations in their CSF (Figure 2A). The levels of CXCL13 were also analysed in RRMS patients who had been followed for at least five consecutive years and from whom CSF samples had been taken during the first year from their MS disease onset. The RRMS patients fulfilling these criteria were limited to 52 individuals. Patients in this subgroup with the highest number of relapse during a 5-year period had the highest CXCL13 concentrations in their CSF (Figure 2B). The total RRMS cohort revealed a trend to an increased disease disability with increased CXCL13 in their CSF, but this trend was not statistically significant (Figure 2C). The numbers of brain lesions detected by MRI in these patients were also related to the levels of CXCL13, meaning that those with the highest CXCL13 levels in their CSF had more than nine brain lesions detected by MRI (Figure 2D).
CXCL13 was related to the relapse rate, Expanded Disability Status Scale (EDSS) and number of lesions detected by magnetic resonance imaging (MRI). (A) Relapsing–remitting multiple sclerosis (RRMS) patients with the highest relapse rates had highest CXCL13 levels in their cerebrospinal fluid (CSF). (B) A sub-cohort of RRMS (n = 52) with the highest number of relapses during 5 years showed highest CXCL13 levels in their CSF. (C) All RRMS (n = 323) had a positive trend (not statistically significant) to an increase disease disability with increased CXCL13 in their CSF. (D) Numbers of lesions detected by MRI in the RRMS cohort were related to the levels of CXCL13. The MRI-detected lesions analysed here correspond to the brain MRI. Significance was determined using a Kruskal–Wallis test followed by a Dunn’s post-hoc test. *p < 0.05; **p < 0.01; ***p < 0.001.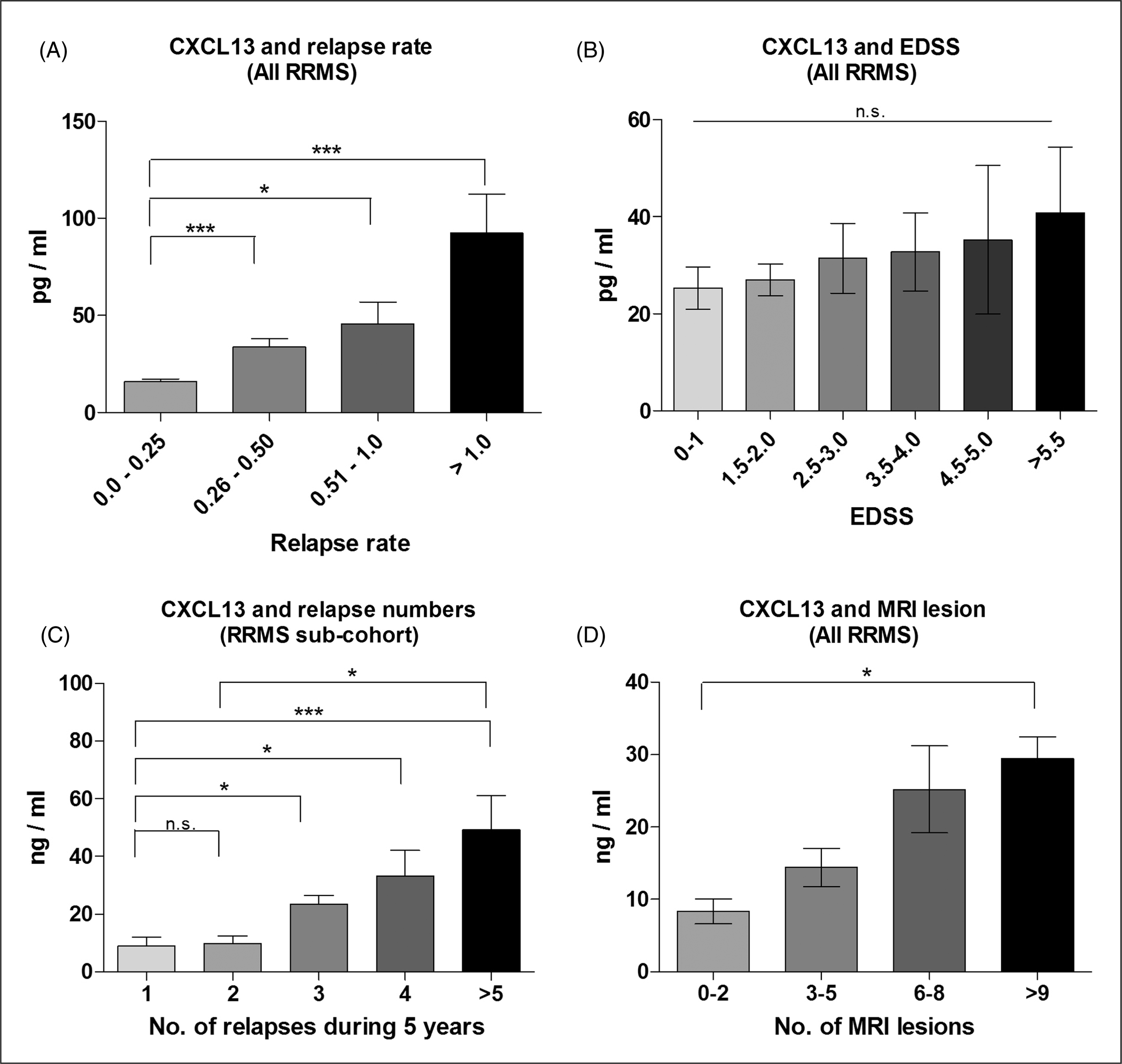
CXCL13 levels are correlated with cerebrospinal fluid cell counts and IgG index
The CXCL13 concentrations had a significantly positive correlation with CSF mononuclear cell counts (Figure 3A) and IgG index (Figure 3B). The iOND subgroup with infections had an even stronger correlation of CXCL13 with CSF mononuclear cell counts (Figure 3C). A negative correlation between levels of CXCL13 and disease duration (calculated from the year of onset until sampling date) or disease progression was observed, and CSF cells were significantly less numerous in SPMS compared with RRMS (data not included).
CXCL13 was correlated with CSF cell counts and IgG index. (A) The CXCL13 concentrations showed a significant positive correlation with the cerebrospinal fluid (CSF) mononuclear cell counts and (B) IgG index in all patients with multiple sclerosis (MS; n = 387). (C) A significant positive correlation between CXCL13 and CSF mononuclear cell counts was also evident in other neurological diseases with viral/bacterial infections (iONDs; n = 23). Significance of correlations was analysed using Spearman’s rank test and linear regression for curve fit.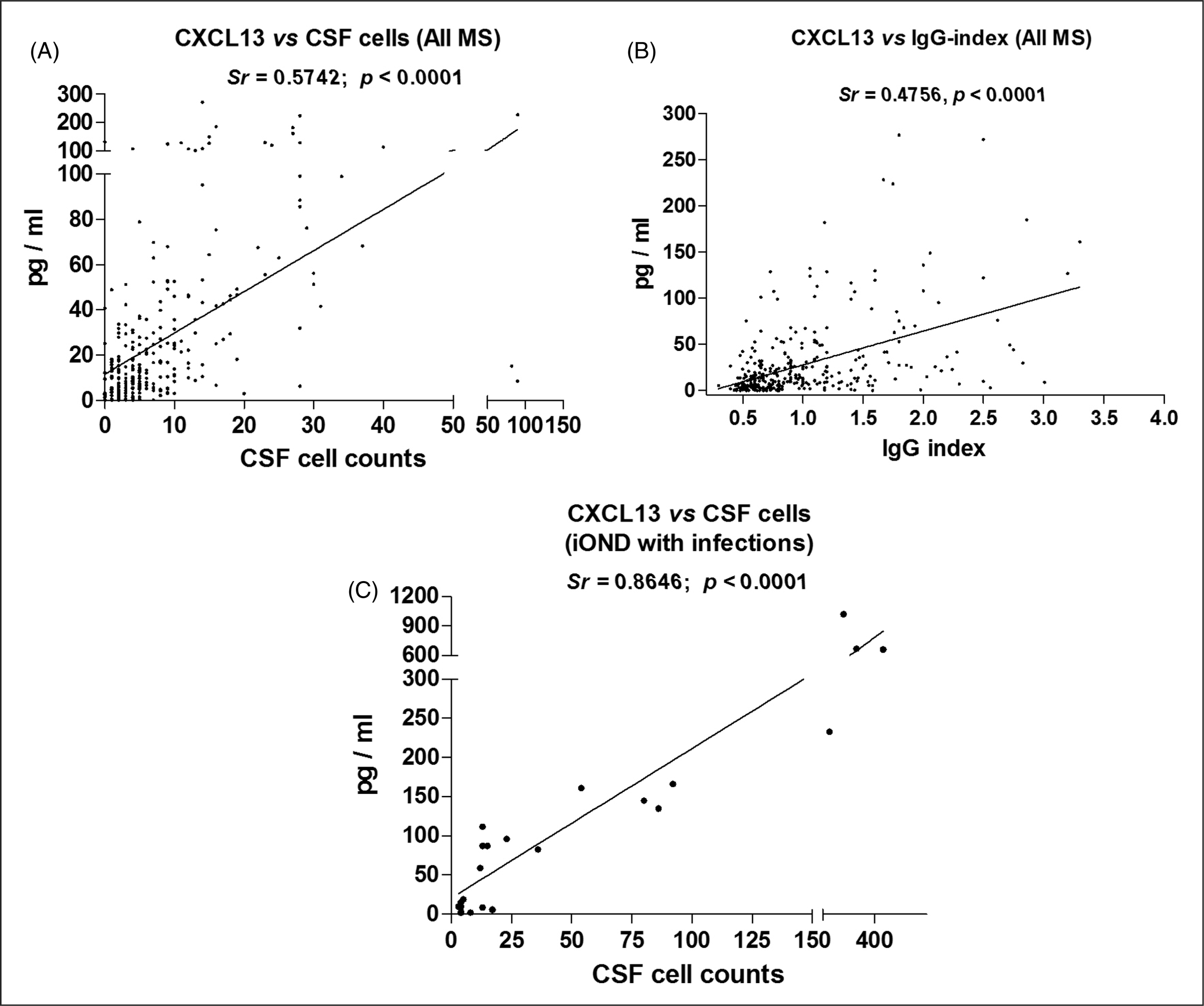
CXCL13 and oligoclonal immunoglobulin bands in cerebrospinal fluid
The majority of the patients with high levels of CXCL13 in their CSF were OCB-positive. Interestingly, this phenomenon was also the same for patients with CIS (Figure 4A).
CXCL13 and oligoclonal immunoglobulin band (OCB) in cerebrospinal fluid (CSF), and conversion of clinically isolated syndrome (CIS) to multiple sclerosis (MS). (A) The majority of the patients with high levels of CXCL13 were OCB positive (84%). This observation was almost the same for patients with CIS (72%). (B) CXCL13 levels were significantly higher in patients with CIS conversion (n = 31). (C) Patients with higher CXCL13 levels within the conversion group experienced a trend to earlier conversion to MS than those with lower CXCL13. Significance was determined using a Kruskal–Wallis test followed by a Dunn’s post-hoc test. *p < 0.05; **p < 0.01; ***p < 0.001.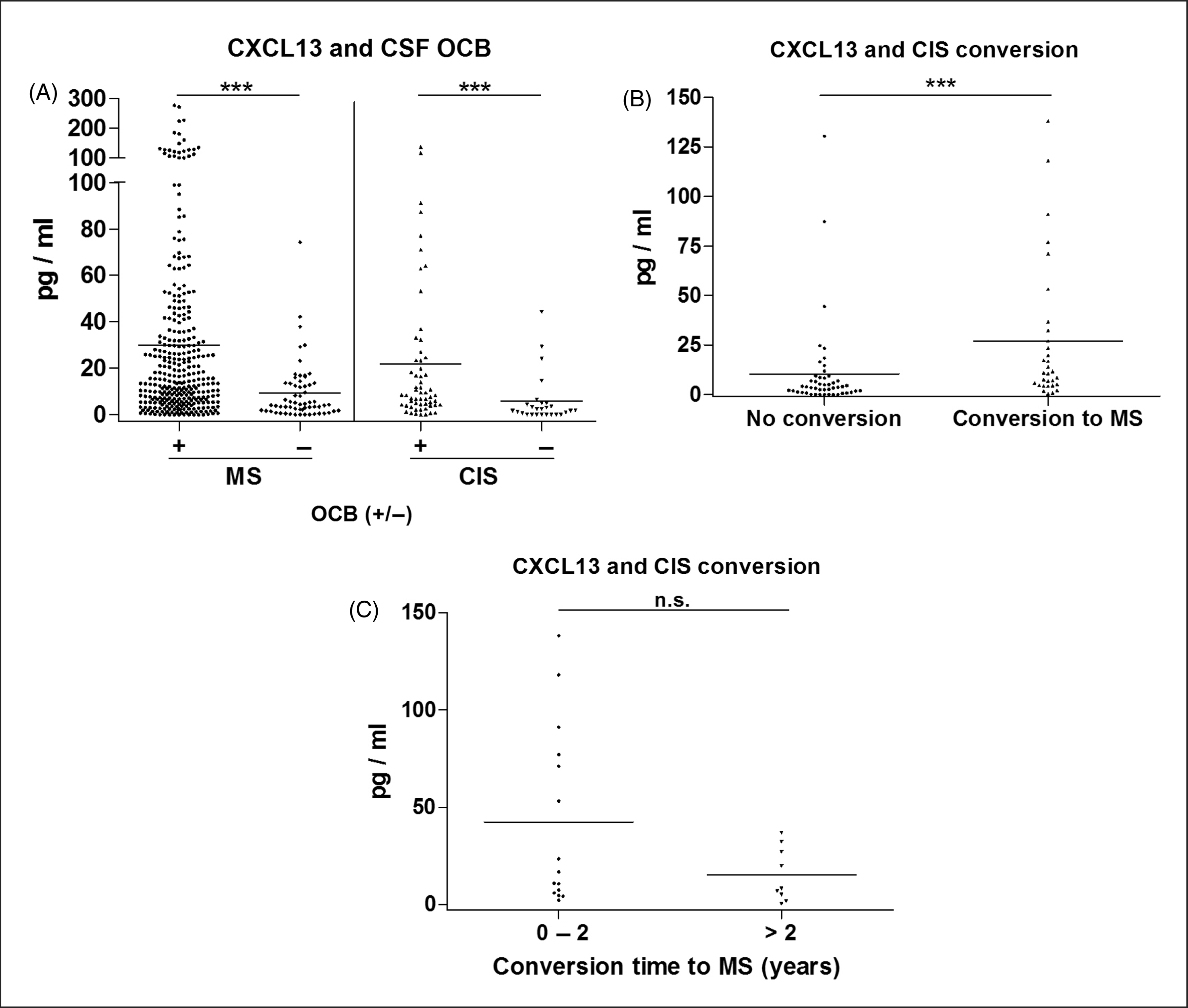
CXCL13 and clinically isolated syndrome conversion
The levels of CXCL13 in patients with CIS were also higher than in controls (Figure 1A). Herein we analysed the levels of CXCL13 in patients with CIS who converted to MS and those who showed no CIS conversion within 2 years from their first episode. The CXCL13 concentration was significantly higher in patients with CIS conversion (Figure 4B). Moreover, patients with higher CXCL13 levels within the conversion group exhibited a trend to earlier conversion to MS than those with lower CXCL13, but this trend was not statistically significant (Figure 4C).
Discussion
Studies of CXCL13 levels, the most potent B-cell chemoattractant, in MS serum and CSF seem to emphasize that this particular chemokine might be a very important marker for MS inflammatory activity. 11,16,17 To be accepted as a biomarker replication studies are important. We confirm the potential role of CXCL13 as a MS disease activity marker in a large clinical case–control cohort, including the whole spectrum of MS forms, as well as large numbers of inflammatory and non-inflammatory subjects with other neurological diseases. In addition to the previous finding that CXCL13 is a good marker of treatment response, 17 we provide data on prognostic aspects indicating that high levels of CXCL13 correlate to CIS conversion into clinically definite MS and relapse rate years ahead from the time of diagnostic lumbar puncture. Moreover, we demonstrate that there is a striking relation between high levels of CXCL13 and the presence of OCB in CSF.
High CXCL13 levels were thus related to the MS disease activity and a future worse outcome as indicated by relapse rate. A positive trend for high CXCL13 was also associated with EDSS and the number of brain lesions detected by MRI. Despite years of treatment with available immunomodulatory drugs, in the majority of these patients the association of CXCL13 levels with unfavourable prognosis was unavoidable. This was clearly observed when levels of CXCL13 were analysed in a subgroup of RRMS patients for whom relapse rate was followed for at least five consecutive years and had CSF samples taken during the first year of disease onset. Patients with highest CXCL13 concentrations experienced the highest numbers of relapses (more than five relapsing episodes of neurological dysfunctions during their first 5 years of disease). However, we found it difficult to differentiate possible relapses in the SPMS group from symptom fluctuations or pseudo-relapses. The occasional ‘true’ relapses in this group were therefore not included in the study. The spinal cord lesions, which also reflect the disease process, were not analysed by MRI in this study because of a lack of this information for most of the patients.
Up-regulation of CXCL13 in patients with acute neuroborreliosis was suggested as a possible early diagnostic marker for this condition. 20,21 In our study we also measured CXCL13 in samples from patients with infections such as herpes simplex encephalitis, Epstein–Barr virus infections and neuroborreliosis. The CXCL13 levels were much higher in these samples compared to all other included samples and the levels were strongly correlated with CSF cell counts. Moreover, elevated levels of CXCL13 in serum were also reported in several human diseases including MS, infectious conditions, neoplastic and rheumatic conditions as recently described. 23 Taken together the high CXCL13 levels associated with infections indicate that the marker is not specific for the disease.
We demonstrated that the levels of CXCL13 were highly correlated with CSF cell counts, which almost correlated with CXCL13 levels regarding the clinical measures mentioned above (data not included). There is a paucity of recent studies of such a simple measure as CSF cell number and its relation to prognosis or therapies. However, it has been reported that CSF white blood cell counts correlated with subsequent clinical and radiological activity in the placebo arm of a phase III trial of Avonex, 27 corroborating our findings with CSF cell counts and levels of CXCL13. Because CSF cells were significantly less numerous in SPMS, and levels of CXCL13 were negatively correlated with the disease duration, the measurement of CXCL13 in the early phase of the disease could be more informative for prediction of the disease course than in the later phase of the disease.
We also demonstrated that patients with MS who were OCB positive had much higher CXCL13 concentrations in their CSF compared to OCB-negative patients. However, this phenomenon is difficult to discuss in relation to any relative value of the two measures in relation to prognosis since CXCL13 is a continuous variable while the OCB are recorded as presence or absence.
Another important observation from this study was the notion that the CIS cohort with higher levels of CXCL13 in their CSF experienced higher rates of conversion to MS and that conversion occurred faster (within 2 years from disease onset) than in those with lower CSF CXCL13 levels. Since most such patients will develop a second event during subsequent months or years, 28 this finding may help the neurologist to predict early MS in individuals with CIS. This will consequently support their decision for early administration of a more effective MS treatment such as natalizumab or rituximab which, indirectly, dampen CSF levels of CXCL13 in RRMS. 17,29 While revising this paper we identified a recently published article with partly similar results regarding levels of CXCL13 in CSF and prediction of CIS conversion to MS. 24 This will, of course, increase the reliability of our work when already confirmed by an independent research group.
In conclusion, our study confirms other reports of increased CXCL13 levels in active MS and, in addition, provides data which support the use of CXCL13 as a candidate prognostic marker for MS as high CXCL13 levels at disease onset correlate with high relapse rate. It may be used for assessing treatment responses 17 and be of help in treatment decisions in early MS when a series of new drugs appears on the market, all with different levels of efficacy and hazards.
Footnotes
Acknowledgements
We would like to thank all the patients, healthy donors, the staff of the neurology clinic at the Karolinska University Hospital, especially Farshid Rafatnia for his assistance, and Dr Robert A. Harris for linguistic advice.
Funding
This work was supported by grants from the Swedish Research Council (project number 11220), Neuropromise (LSHM-CT-2005-018637), the Swedish Society of the Neurologically Disabled, and the Bibbi and Nils Jensens Foundation.
Conflict of interest statement
Dr. Olsson has received research support from Biogen Idec., Bayer-Schering Pharma, Sanofiaventis and Merck Serono.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.