
Abstract
Introduction
The incidence of multiple sclerosis (MS) most accurately portrays the variability of disease severity 1 and study results at diagnosis. In recent years, MRI has assumed a greater role in the evaluation of patients with suspected MS. We are aware of only one recent population-based 2 incidence study of MS where ‘the majority’ had an MRI study done, but the exact proportion was not specified.
Two studies from Iceland have reported the incidence of MS to be 4.98–5.28 per 100,000 (1981–1990) 3 and 1.94 per 100,000 (1956–1965). 4 We determined the incidence of clinically definite MS and the results of the principal diagnostic studies used in the diagnosis of MS. The study included the entire population of Iceland over a 6-year period.
Materials and methods
Iceland is an island in the North Atlantic, between latitudes 64° and 66° north, and the mean all-year temperature in Reykjavík, the capital, is 4.6°C. 5 The population is well defined and was 296,835, on average, during the study period. 5 Approximately 62% of the population lives in the area of the capital. 5
The Icelandic healthcare system is modern and easily accessible to all residents. There is one neurology department in Iceland and three radiology departments with MRI equipment. During the study period there were, on average, 17 neurologists practicing in the country, or 6 per 100,000 population.
The 6-year study period was from 1 January 2002 through 31 December 2007 and, for the first time, made an effort to identify all residents of Iceland diagnosed with MS during the study period. We only included individuals who met the Poser criteria for clinically definite and primary progressive MS 6 and these are the index cases of this study. All the index cases were diagnosed by a neurologist and many were seen by more than one neurologist. The time of diagnosis was set at the second observed attack or when fulfilling Poser criteria for primary progressive MS. Individuals who only had a single clinical attack (clinically isolated syndrome) are not included in the study and are not further considered.
Affected individuals were identified from the records of: (1) the neurology department at the Landspitali University Hospital; (2) all practicing neurologists in Iceland; (3) smaller hospitals and rehabilitation centres; (4) the results of visual evoked potential (VEP) studies; (5) all MRI studies done in Iceland because of suspected demyelinating disease; and (6) all those approved for treatment of MS with interferon, glatiramer acetate or natalizumab, which need approval by a centralized agency. Many affected individuals were identified in two or more ways. We reviewed the records of the index cases to verify the diagnosis and determine gender and age at diagnosis, time of diagnosis and results of diagnostic studies. We determined the incidence rate for MS in Iceland by calculating the total person-years of observation during the 6-year study period (2002–2007). We determined the age- and gender-specific incidence. We used the mid-year population for each year as provided by Statistics Iceland. 5 We calculated the incidence, adjusted to the year 2000 US standard population. The study was approved by the Icelandic National Bioethics Committee and Data Protection Authority.
Results
We identified 136 individuals who met the inclusion criteria; these are the index cases of this study. All had clinically definite MS according to the Poser criteria. The majority (93%) (126/136) had relapsing–remitting MS and 7% (10/136) had primary progressive MS, according to the Poser criteria 6 (at least a 6-month progressive course with no remissions or exacerbations). None had secondary progressive MS at diagnosis. All were native-born Icelanders, except one individual who was of Danish origin.
The diagnosis of MS was based on a historic relapse in nine (6%) of our index cases. Their initial symptoms had occurred prior to the study period and included typical sensory-level symptoms (4 patients), gait ataxia (3), sensory impairment in one arm and Lhermitte’s sign (1) and hemidysesthesia (1). All nine had second and third relapses, both verified by a neurologist, during the study period. Eight individuals had a single verified relapse during the study period and gave a history of prior poorly described transient symptoms, not verified as a relapse. They were considered by us to have clinically isolated syndrome and were not included in the study.
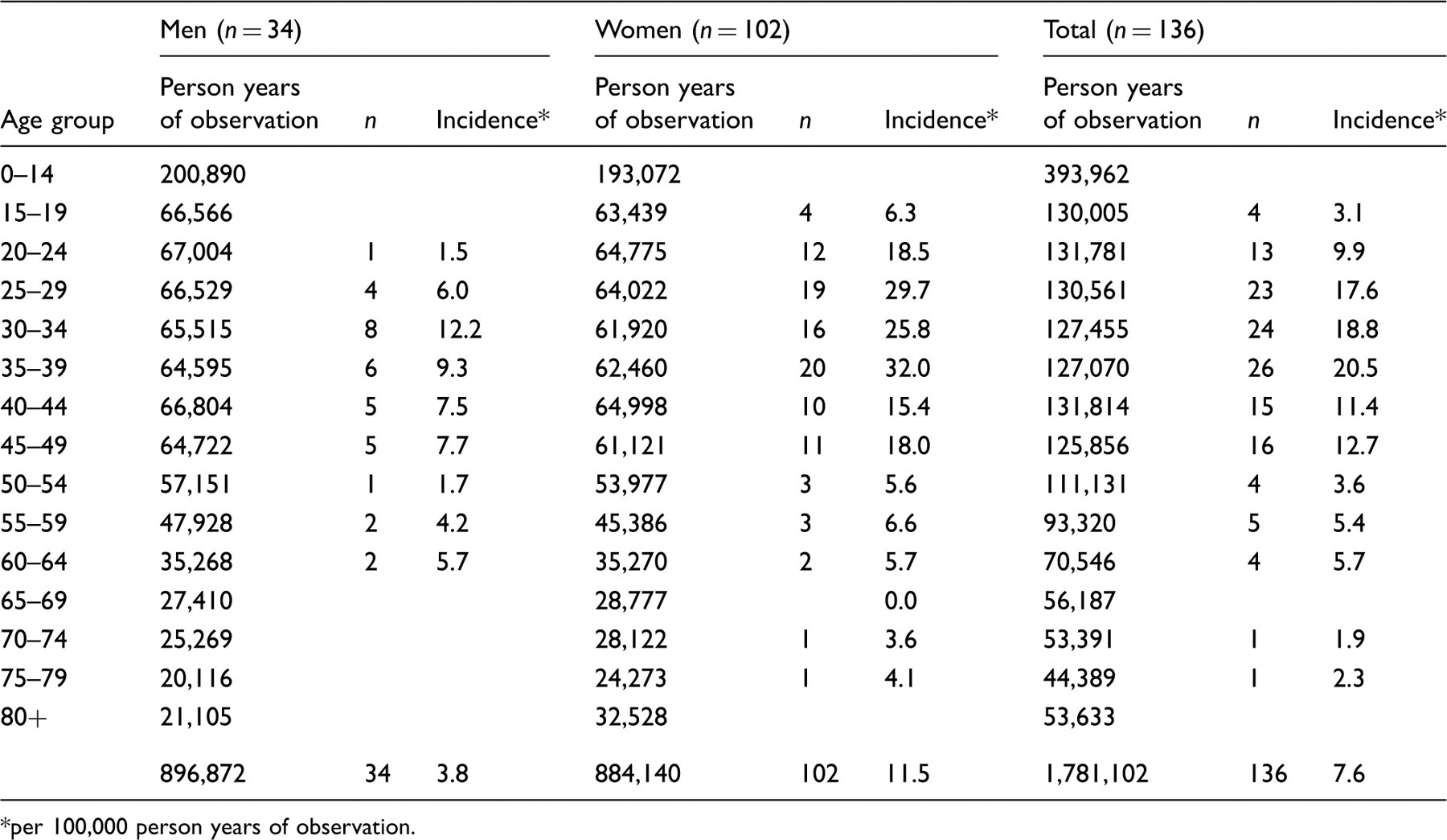
The average annual incidence for MS (Table 1) during the 6-year study period was 7.6 per 100,000 population (95% CI 6.4–9.0) and 8.2 per 100,000, when adjusted to the 2000 US white population. The incidence peaked between 30 and 34 years for men and 35 and 39 years for women. The two eldest index cases were diagnosed after 70 years of age (Figure 1). There were 102 women (75%) and 34 men (25%).
Age-specific incidence of multiple sclerosis in Iceland, 2002–2007. Age and sex-specific incidence of multiple sclerosis in Iceland, 2002–2007 per 100,000 person years of observation.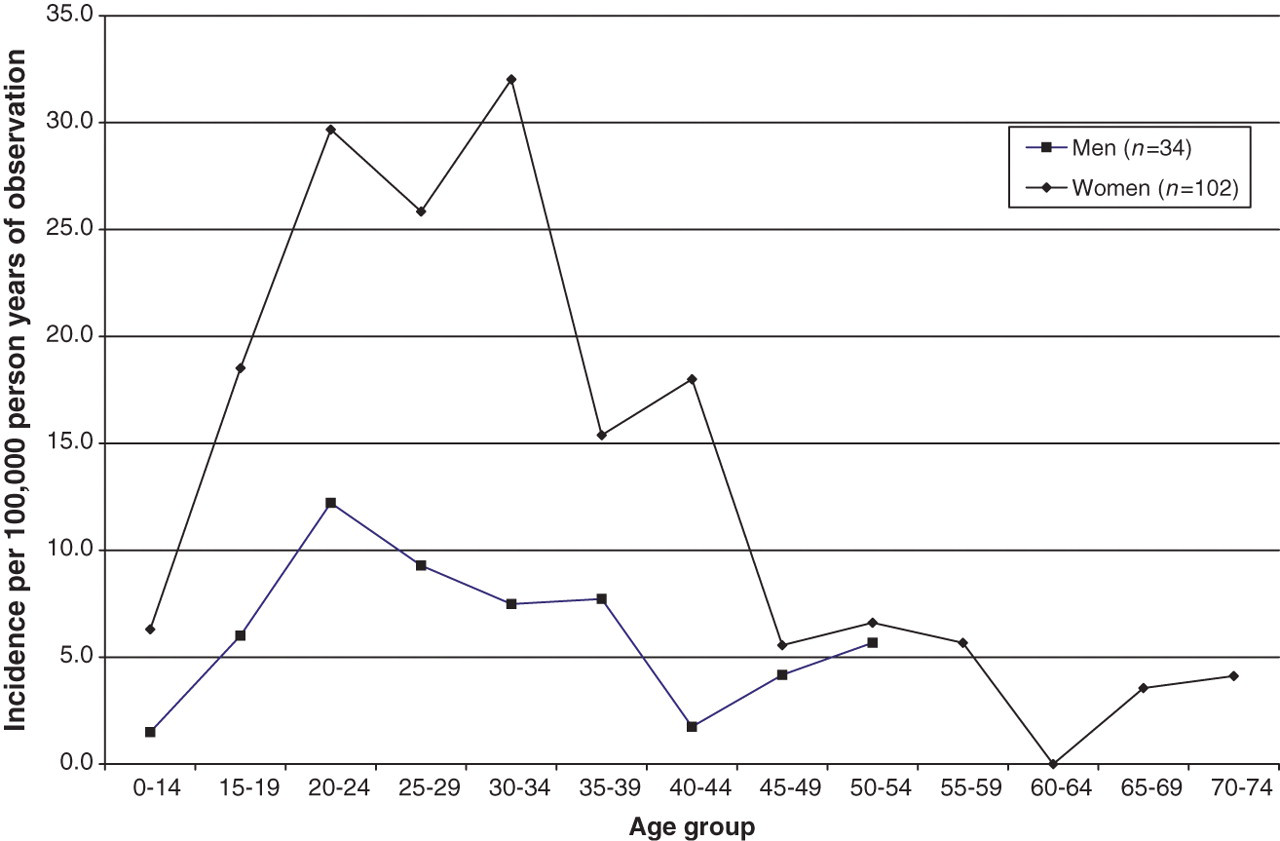
The overall mean age at diagnosis was 36.3 years (median 35; range 16–75), the mean age for women was 35.7 years (median 34.5) and the mean age for men was 38.3 years (median 40.0). The overall mean age at onset was 32.0 years (30.7 for women and 35.8 for men).
MRI was done in 99% (135/136) at the time of diagnosis and 61% (83/135) of these fulfilled the Barkhof criteria. 7 One index case had a normal MRI scan and one did not have an MRI study done (73-year-old woman with typical MS symptoms and oligoclonal bands in the CSF). Seventy percent (94/135) of the patients had MRI of both head and spinal cord, but 13% (12/94) only had MRI of the cervical spine.
Spinal fluid analysis was done in 78% (106/136). Oligoclonal bands were found in 75% (80/106) and 65% (52/80) fulfilled the Barkhof MRI criteria, compared with those without oligoclonal bands, of whom 63% (15/24) fulfilled the Barkhof criteria (p = 0.82).
VEPs were measured in 68% (92/136) and abnormally prolonged VEP, consistent with optic neuritis, were found in 43% (42/92). An MRI scan was done in all those with normal VEP (N = 50), and 66% (33/50) of them fulfilled the Barkhof criteria. All those with abnormally prolonged VEP (N = 42) had an MRI scan, and 60% (25/42) of them fulfilled the Barkhof criteria (p = 0.52).
Discussion
Our incidence of 7.6 per 100,000 is similar to several reports from northern Europe and North America. A population-based study from Oslo, Norway found an incidence of 8.7 per 100,000 for clinically definite MS. 8 A population-based study from Finland 9 (1979–1993) reported the incidence of clinically definite MS in three separate and defined populations to be 9.4, 6.0 and 5.1 per 100,000, respectively. The investigators concluded that the difference between the three populations was caused by ‘unknown environmental factors’. A population study from Scotland 10 in 1989–1992 found a higher incidence of 12.2 per 100,000 population. The study included both probable and definite MS and is consequently not directly comparable with our results.
A study from Olmsted County, MN, USA 11 for the period 1985–2000 reported an incidence of 7.3 per 100,000 population for probable and definite MS, when age and sex were adjusted to the 2000 US population. This compares with the higher incidence of 8.2 per 100,000 population for definite MS in the current study, when adjusted to the 2000 US population. A population study 2 from Saskatoon, Canada (1970–2004) reported an incidence for definite and probable MS of 8.1 per 100,000 population (7.8 per 100,000 when adjusted to the 2000 US population). The differences in incidence between the various studies may be explained by differing inclusion criteria.
The annual incidence in the present study (7.6 per 100,000 population) is considerably higher than the 5.3 per 100,000 population reported from Iceland 3 for the period 1986–1990. We do not know the explanation for this difference. The availability of MRI (first introduced in Iceland in 1991), the increased emphasis on early MS diagnosis, because of the availability of effective treatment, and the heightened awareness of MS among physicians and the public may all have led to earlier diagnosis of MS.
All the index cases were diagnosed by a neurologist and most were extensively studied. All but one (99%) had at least one MRI study done. Cerebrospinal fluid (CSF) was examined in 78% (106/136) and VEPs in 68% (93/136). The McDonald criteria 12 became available during the study period but were not used in this study. We included only those who also fulfilled the time-honoured Poser criteria for definite diagnosis. This was done to avoid the impact of the diagnostic uncertainty sometimes associated with a single clinical episode. Due to the difficulty in accurately timing the first symptoms of MS by the medical history, we used the date of the second confirmed attack as the reference point in calculating the incidence of MS.
Presumed MS symptoms may precede the diagnosis of MS by decades (up to 37 years in Olmsted County 11 and 61 years in Wales). 13 Patient identification in incidence series of MS is based on the diagnosis, but several authors have also determine the so-called onset adjusted incidence. We believe that determining onset of MS retrospectively is difficult for many reasons (e.g. recall bias) and can be hard to interpret (e.g. not population-based) and therefore we have not calculated this parameter.
We found that 75% of patients were women, compared with 70% in the Oslo study 1 and 71% in Olmsted County. 8 Older studies from Iceland found the proportion of women to be 58% (1956–1965) 4 and 69% (1986–1990). 3 This apparent increase in the proportion of women with MS in Iceland is comparable with several studies that have reported an increasing proportion of women 2 being diagnosed with MS.
The overall mean age at diagnosis in our study was 36.3 years. This is similar to the 38.3 years reported in Oslo, Norway 8 and 36.2 years in Olmsted County. 11 The highest age- and gender-specific incidence is among women aged 35–39 years of age or 32.0 per 100,000 years. Iceland has a modern healthcare system and one of the lowest infant mortality rates in the world. 5 There is a relatively easy access to neurologists and to MRI. We believe we identified the great majority, probably all, who fulfilled the inclusion criteria for diagnosis of clinically definite MS during the study period.
We find the incidence of MS in Iceland comparable with recent studies from Scandinavia and higher than previously reported from Iceland. Most studies from Europe and North America are not directly comparable because we included only clinically definite cases, as defined by the Poser criteria.
Our results are generally comparable with most population-based studies 8,11 from Western Europe and North America, even if these studies vary as to whether they include only clinically definite MS or also probable MS cases. There are only a few incidence studies available from the MRI era 2,8 – 11,14 and our study describes the MRI results. MRI was done for 99% of the individuals in this study, and 61% of them met the Barkhof criteria at the time of diagnosis; this proportion was comparable regardless of the presence of abnormal VEP or oligoclonal bands.
Footnotes
Acknowledgment
Mrs Eiríka Urbancic helped with retrieving patient files.
Funding
The study was supported by a competitive research fund at the Landspitali University Hospital in the amount of 100,000 ISK (approximately US$800).
Conflict of interest statement
The authors report no conflicts of interest.