
Abstract
Keywords
Introduction
To date there is no cure for multiple sclerosis (MS) and little evidence that pharmacological solutions can help the muscle weakness and gait problems commonly experienced by people with this condition. 1 Research has shown that there is a direct and primary correlation between muscle strength and the performance of many everyday activities, such as walking, in people with MS.1–4 For this reason, it has been argued that using progressive resistance training (PRT) to increase muscle strength might help improve the performance of physical activities such as walking and thereby increase the health-related quality of life5,6 of people with MS. The key principles of PRT in healthy individuals are to perform sets of a small number of exercise repetitions (usually 8–12) with relatively high loads until muscle fatigue is reached, and to increase the load as muscle force develops over time. 7
Although there is a rationale for implementing PRT, the role of this intervention for people with MS remains uncertain because relatively few studies of satisfactory quality have examined its effects in this population. One of the few available studies 8 used a randomized controlled research design to determine the effects of a home-based program conducted three times a week for 8 weeks on 19 adults with MS. Compared with a wait-list control group, the resistance group significantly increased leg extensor muscle power by around 37% without negative effects. However, no changes were detected in more functional outcomes such as in the timed up-and-go test. No attempts were made to determine how long improvements were maintained after training was finished.
Another randomized controlled trial9,10 investigated the effects of a supervised resistance training program conducted twice a week for 12 weeks with 19 participants training in small groups using pin-loaded weight machines. Results were again compared with a wait-list control group. Participants in the training group, measured immediately after completing the program, significantly increased muscle performance, functional outcomes (including walking), improved quality of life related to physical function, and reduced general fatigue. Reassessment of this group 12 weeks after completing the supervised program showed all improvements were maintained. However, because after finishing the supervised program participants were encouraged to continue training unsupervised, it remains unknown if improvements in physical function persist if participants stop exercising. This is important to investigate because in reality most people are not willing to continue high-intensity exercise programs indefinitely, particularly without evidence available to support the need to continue. Also, PRT might have a differential effect on people with MS compared with people who have no physical impairments. In people without impairment, muscle strength tends to reduce to pre-training levels relatively quickly after they stop exercising. This is probably because their pre-training strength exceeds that required for everyday functional activities. However, because muscle weakness in people with MS can impact on the performance of everyday activities, increases in muscle strength from PRT might lead to more permanent changes in everyday physical activities that in turn might lead to the maintenance of strength and other beneficial outcomes without the need to keep exercising. A previous randomized controlled trial of PRT in young people with cerebral palsy 11 provides some support for this idea.
Other studies of lesser quality have reported improvements in muscle strength12–16 and endurance, 13 walking speed12,13,15,17,18 and endurance, 16 stair climbing speed, 15 timed up-and-go 15 and chair transfers, 17 as well as general fitness, 17 self-reported disability13,15 and self-reported fatigue. 16 However, apart from one, 17 all of these studies used a single-group pre-post research design and so their results must be interpreted cautiously. The remaining study 17 was described as a randomized controlled trial, but analyses were only done for within-group changes and so, like the single-group studies, conclusions were not based on comparisons against control data.
Together this literature provides preliminary evidence that PRT might have physical and psychological benefits for adults with MS, and that these might persist for some time after completing a supervised program so long as people keep exercising independently. However, due to the use of relatively small samples, non-blinding of assessors, lack of effective control data, and insufficient control of potentially confounding factors such as the impact of increased attention and social interaction during the training programs, the effects of PRT need further investigation.
Given these considerations, the primary aim of this randomized controlled trial was to examine the immediate effects of a supervised PRT program on walking function in people with relapsing–remitting MS who had difficulty walking. The secondary aims were to determine the effects of the exercise program on muscle performance (strength, endurance, stiffness and spasm), fatigue, and health-related quality of life, and to determine if any improvements were maintained 12 weeks after a complete break from training. It was hypothesized that compared with a control group, people with MS who participated in PRT would:
walk further over 2 min, and their maximum walking speed over 10 m would be faster;
demonstrate increased leg muscle strength and increased leg muscle endurance;
demonstrate less physical fatigue and greater health-related quality of life;
demonstrate no change in muscle stiffness and muscle spasms, and there would be relatively few adverse events during the exercise program; and,
any changes observed in the training group immediately after completing the program would have dissipated if participants had a complete break from training for 12 weeks.
Methods
Participants
Participants were recruited through a statewide organization providing education and support to people with MS, and a large specialist MS outpatient clinic. To be included, people had to be aged 18 years or more, have a confirmed diagnosis of relapsing–remitting MS, have an Ambulation Index score 19 of 2, 3 or 4 (mild to moderate walking disabilities), and have received medical clearance to participate. Volunteers were excluded if they had an acute exacerbation of MS within 2 months of starting the program, had benign or progressive/relapsing types of MS, had a serious unstable medical condition, had any concurrent condition, for example stroke, or had participated in a PRT program in the 6 months before training started. Recruitment information flyers were sent by mail to all potential participants registered on the mailing lists of both organizations. If interested, volunteers were asked to contact one of the researchers (KD) by telephone, during which volunteers were screened to ensure they satisfied the inclusion criteria.
The University Human Ethics Committee approved this trial, and written informed consent was obtained from each participant. This trial was registered at the Australian New Zealand Clinical Trials Registry (ACTRN 12607000101482).
Procedures
Participants were randomly allocated to either the experimental or the control group. Consistent with the CONSORT guidelines, 20 a separate randomization procedure was prepared for each stratum (Ambulation Index 2, 3 or 4) using permuted blocks. For each stratum, the block allocation sequence was generated by the research coordinator (KD) from a random-numbers table, and assignments sealed in sequentially numbered opaque envelopes. After enrolment, participants were allocated to either ‘progressive resistance training’ or ‘control’ by opening the next envelope in the sequence.
The experimental group completed a 10-week (two times per week), PRT program in one of four community gymnasiums in metropolitan and regional areas. The exercises targeted the key lower limb muscles for supporting body weight and for generating and absorbing power during walking (Table 1). 21 While these were the core exercises, they could be individualized. For example, if any exercise caused discomfort, the starting position was modified or the exercise was replaced. All exercises were completed on weight machines. The training intensity was based on recommendations of the American College of Sports Medicine (2009) 7 and consisted of two sets of 10–12 repetitions of each exercise, at a training intensity of 10–12 repetition maximum (that is, only 12 consecutive repetitions of each exercise could be completed before muscle fatigue was reached). The weight lifted was increased when two sets of 12 repetitions of an exercise could be completed. Two-minute rest periods were given between each exercise set. Each participant had a logbook detailing each exercise, the weight lifted, the number of repetitions, and the number of sets completed. This was filled in at the end of each session.
Basic Progressive Resistance Training Program
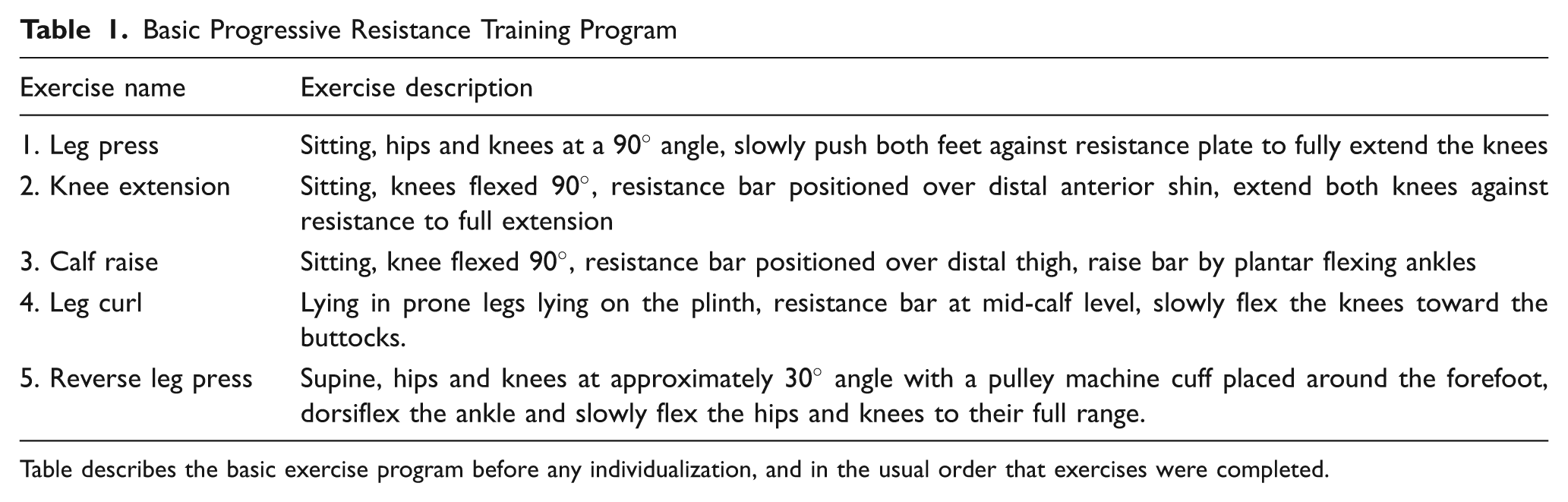
Table describes the basic exercise program before any individualization, and in the usual order that exercises were completed.
Each program was attended by a group of up to 12 participants, and they were supervised by up to three experienced trainers (physiotherapists and registered personal sports trainers). Each trainer directly supervised a sub-group of three or four participants. Each exercise session was completed in around 45 min, and at the end of each session there was a 30-min recovery period when the participants had refreshments and time to socialize.
Participants in the control group received ‘usual care’ plus a social program. ‘Usual care’ could include habitual exercise participants engaged in, or therapy, provided it did not include PRT. In addition, to control for the increased attention and social aspects of the resistance training program, the control group participated in an attention and social program conducted for 1 h each week for 10 weeks. The program comprised leisure and social activities not expected to have a fitness or training effect, such as massage, luncheons and educational sessions, including some that enabled participants to experience a single session of different physical therapies such as Bobath therapy and yoga. In developing the control program careful consideration was given to optimizing participant attendance. Pilot work we completed earlier suggested that a program perceived by participants as being ineffective, such as simple muscle stretching, or one that required participants allocated to a control intervention to attend several sessions each week, was unlikely to be adhered to. Therefore, to balance the need to maximize control group adherence against the need to provide adequate control for the potentially confounding active ingredient of attention and social interaction, the control program we developed: 1) took into consideration participant choices about content; 2) included some minimal exercise attention control activities (e.g. yoga, Bobath therapy) provided they would not be expected to provide a sufficient stimulus to increase muscle strength; and, 3) minimized the total number of attendances for control participants’ convenience while matching the approximate total duration (in minutes per week) of attention and social interaction between the control and experimental programs.
Outcome measures
Outcome measurements were taken three times: at baseline, after 10 weeks to determine the immediate effects of the intervention, and after a further 12 weeks (week 22) to determine if any benefits from the program had been sustained. After completing their 10-week intervention programs, participants were asked to return to their usual activities and not to continue or commence resistance training until after the follow-up assessment session. Outcome measures were taken by a registered physiotherapist blinded to group allocation, and experienced in musculoskeletal evaluation.
Primary outcome measures
Changes in walking endurance were measured with the 2-minute walk test (2MWT). 22 Participants were instructed to walk at their preferred speed using their usual assistive device up and down a 10-m walkway for 2 min, with the distance walked measured. Changes in maximal walking speed were measured by recording the time taken to walk the middle 10 m of a level 14-m walkway using a stopwatch. 22 If relevant, the participant used their normal assistive device. For both walking performance outcomes, the assessor provided standardized instructions to each participant and the assessor answered any questions and provided a demonstration of the test. For both tests, participants’ performed only one trial with no practice trials.
Secondary outcome measures
Changes in muscle strength were determined by the amount of weight that could be lifted in a single seated leg press (1RM, 1 repetition maximum) and a single reverse leg press (resistance of the combined movement of hip flexion, knee flexion and ankle dorsiflexion) (1RM). In adults with MS, a single 1RM leg press has been measured with high levels of retest reliability (r > 0.93). 13
Changes in muscle endurance were measured by counting the repetitions that could be completed when the weight on the seated leg press and reverse leg press was lowered to 50% of 1RM. There is evidence of construct validity for this measure in that this method detected hypothesized changes in adults with MS for the leg press. 13 The baseline weight lifted (50% of 1RM at baseline) was used for the 10-week and 22-week measurement as recommended. 23 Changes in muscle performance were measured using the same equipment that participants used in their exercise training sessions, but to reduce learning effects, the 1RM and muscle endurance assessment protocols were not practiced during training sessions.
Changes in self-reported fatigue were assessed using the Modified Fatigue Impact Scale (MFIS). 24 The MFIS consists of 21 items that assess how fatigue affects an individual’s physical, psychological and psychosocial functioning. It has demonstrated evidence of validity with moderately high correlations (r = 0.69) with the vitality subscale of the Short Form-36. 25 Participants were categorized as being fatigued if they scored more than 38 on the MFIS total score. 26
Changes in health-related quality of life were quantified using the WHOQoL-Bréf. 27 This scale contains 26 items that measure the domains of physical health, psychological health, social relationships, and environment. The scale has been found to have high internal consistency and test–retest reliability in adults with neurological disabilities. 28
Possible adverse changes in muscle stiffness and spasm were measured with the muscle stiffness and muscle spasm subscales of the Multiple Sclerosis Spasticity Scale-88 (MSSS-88). 29 This disease-specific instrument has high internal reliability (coefficient > 0.93), and moderately high concurrent validity with other scales such as the physical domain of the MSIS-29 (Multiple Sclerosis Impact Scale). 29 Other possible adverse events that might occur during training were recorded at the end and at the start of each exercise session by the exercise trainers. Any incidents during the intervention phase of the study, including relapses, were described in detail and recorded in the participant’s logbook.
Data analysis
To determine sample size, power analysis was completed using data from a pilot study. 13 Based on the most conservative of the walking performance effect sizes from that study (d = 0.75, the 2MWT), with power of 0.80, a sample size of 35 participants was required in each group to detect a difference between groups.
To determine whether the PRT group improved more than the control group immediately after the 10-week program, data were analyzed with analysis of covariance using the baseline measures as covariates, a method that has been recommended for the analysis of continuous data measured at baseline and follow-up in randomized controlled trials.30,31 Categorical outcome variables were analyzed with relative risk ratios. To determine if the PRT group improved more than the control group 12 weeks after the program had finished and participants had been advised to not train, a separate analysis of covariance was completed on follow-up data at 22 weeks using baseline measures as covariates. Standardized mean differences (effect sizes) and 95% confidence intervals (CI) were calculated from post-intervention means and standard deviations (SD). 32 To interpret the clinical significance of any statistically significant between-group differences, half the SD of the control group at baseline was accepted as representing the minimally important difference. 33 Analysis was completed without Bonferroni adjustment because we decided that this would have resulted in a risk of missing real effects (type II errors) and the consequences of any type I errors would not lead to any negative effects on participants. 34 Intention-to-treat analysis was applied, with all participants who were allocated and commenced their program included in analysis. Where data were missing, the carry forward technique was used. 35 Analysis was repeated after a small number of extreme outliers were omitted. Since omission of these outliers did not change the outcome of any of the statistical tests, only the results from the complete data sets are presented.
In addition to the primary analyses and to compare the results to other previous relevant trials that have not conducted intention-to-treat analysis, we conducted a per protocol analysis for participants who completed more than 18 of the scheduled 20 training sessions. The relationships between any significant changes in outcomes were explored using Pearson product moment correlations.
Results
Figure 1 summarizes the flow of participants through the study. People in the training program attended a mean of 18.4 (SD 2.9, range 6–20) of their 20 scheduled sessions, while people in the social program attended a mean of 6.2 (SD 3.1, range 0–10) of their 10 scheduled sessions. Baseline data indicated that the groups were well matched for demographic factors such as age, gender, height, weight, severity of MS symptoms, gait aid use and fatigue (Table 2).
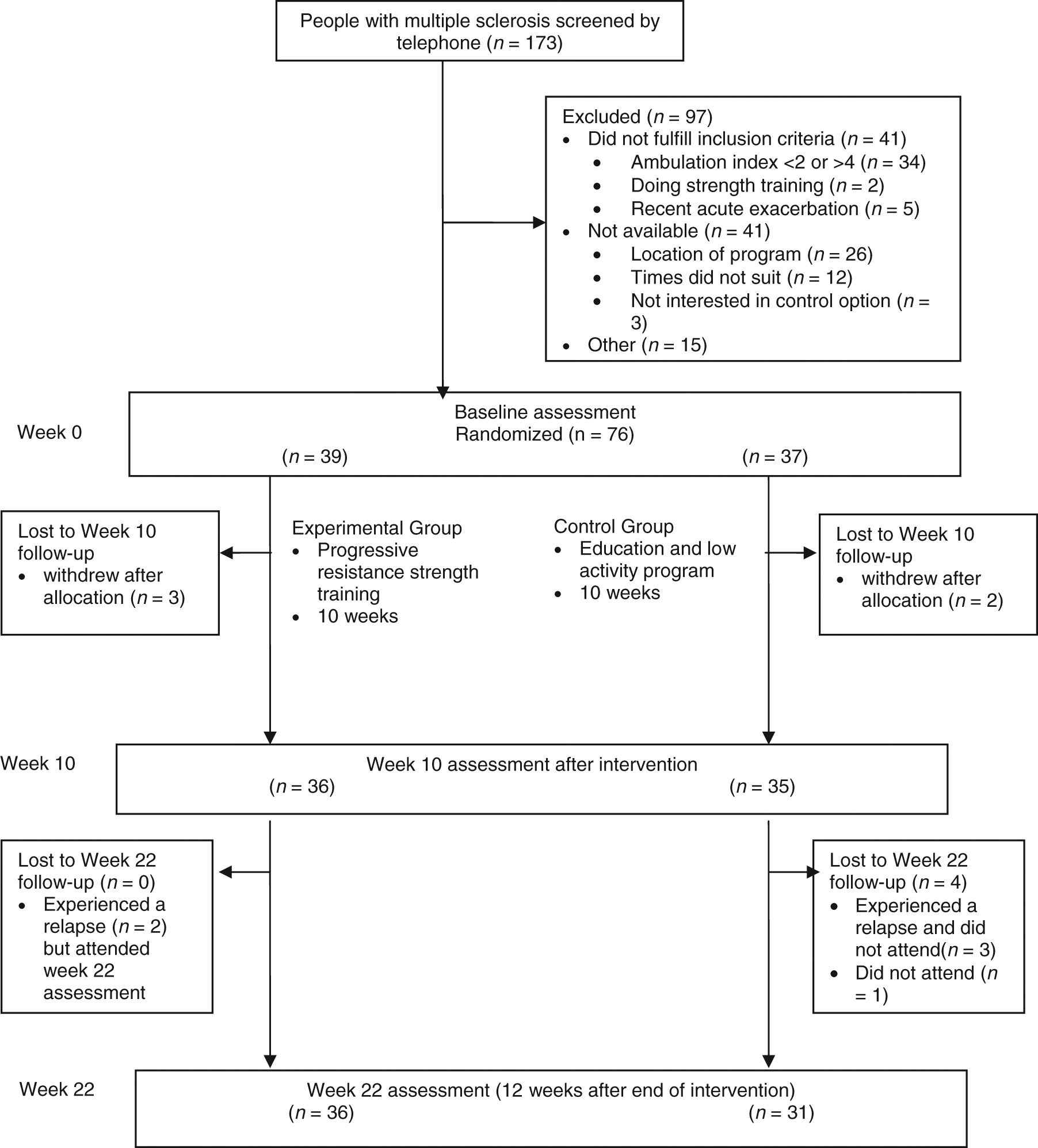
Flow of participants through the trial.
Baseline demographic data
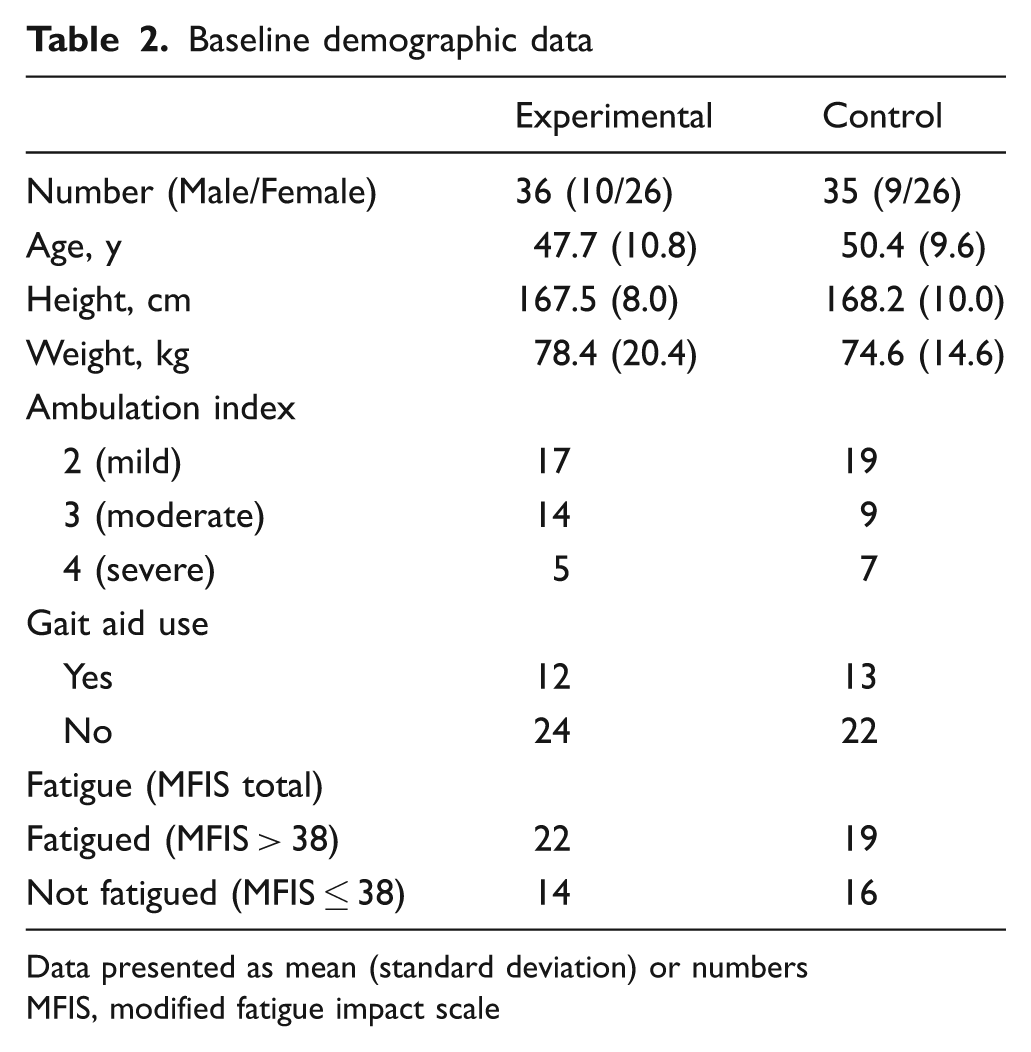
Data presented as mean (standard deviation) or numbers
MFIS, modified fatigue impact scale
Effects of strength training after 10 weeks
Primary outcomes
Walking performance
As Table 3 shows, at the end of the 10-week program, participants in the PRT group did not significantly increase the distance they walked over 2 min (2.6 m, 95% CI -4.0–9.1), or increase their maximal walking speed (0.04 m s−1, 95% CI -0.05–0.13) compared with the control group. A per protocol analysis of the 26 participants who attended more than 18 training sessions also demonstrated no significant increase in the distance they walked over 2 min (5.1 m, 95% CI -2.0–12.1) or increase in their maximal walking speed (0.05 m s−1, 95% CI -0.05–0.14) compared with the control group.
Primary outcomes: Walking performance. Mean (SD) of groups, mean (SD) difference within groups, and mean difference and effect size (d) (95% CI) between groups
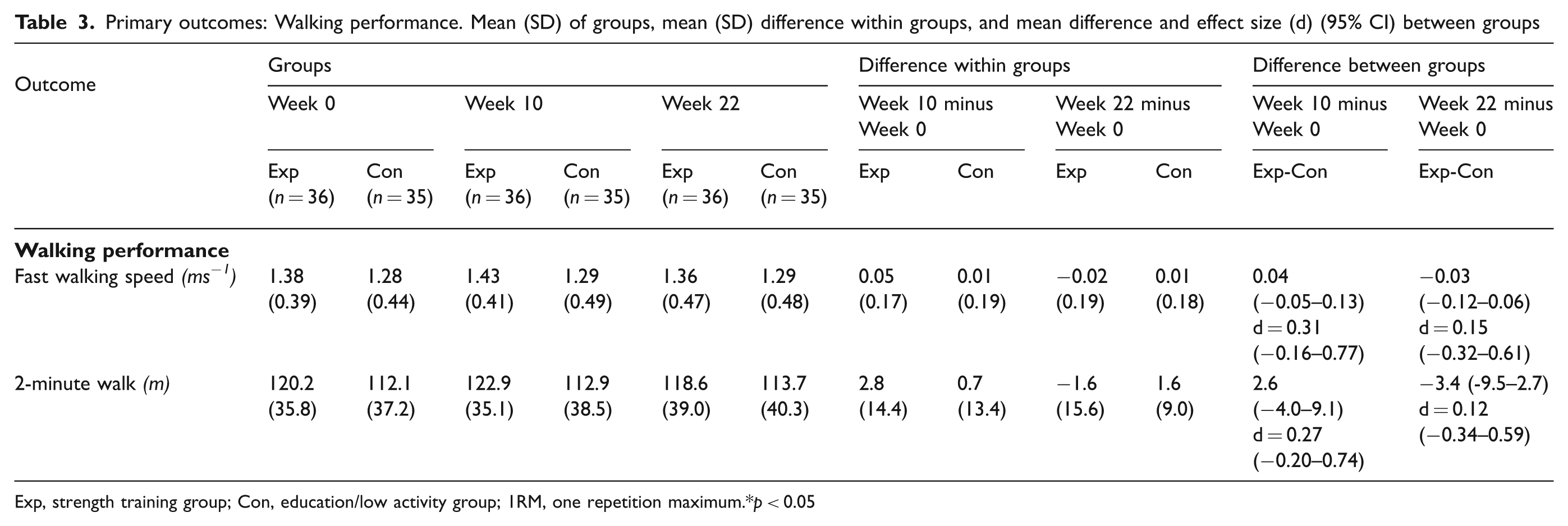
Exp, strength training group; Con, education/low activity group; 1RM, one repetition maximum. *p < 0.05
Secondary outcomes
Muscle performance
As Table 4 shows, at the end of the 10-week program, participants in the PRT group significantly increased leg press 1RM (10.8 kg, 95% CI 4.9–16.7) and reverse leg press 1RM (5.7 kg, 95% CI 1.9–9.5) compared with the control group. These changes represented average strength increases of 16.8% (SD 4.5) and 29.8% (SD 12.7), respectively. The increase in reverse leg press strength exceeded the minimally important difference of 29%, but the increase in leg press strength was less than the 26% increase required to be considered a minimally important difference. Participants in the training program also increased the muscle endurance of the reverse leg press (8.3 repetitions, 95% CI 3.0–13.6) compared with the control group, representing an average increase in muscle endurance of 39.7% (SD 32.8), in excess of the minimal important difference of 32%. Between-group changes in leg press muscle endurance approached but did not reach significance in favor of the PRT group (26.0 repetitions, 95% CI −1.7–53.8) (F (1,68) = 3.495, p = 0.07).
Secondary Outcomes: Muscle performance, fatigue, quality of life, stiffness, and spasm. Mean (SD) of groups, mean (SD) difference within groups, and mean (95% CI) difference and effect size (d) between groups

Exp, strength training group; Con, education/low activity group; MFIS, modified fatigue impact scale; MSIS-88, multiple sclerosis spasticity scale; WHOQOL-BREF=World Health Organization Quality of Life – shorter version. * p < 0.05.
Fatigue and quality of life
As Table 4 also shows, at the end of the 10-week program, participants in the PRT program had significantly reduced symptoms of physical fatigue (−3.9 units; 95% CI −6.6– −1.3) and total fatigue (−5.9 units; 95% CI –11.3– −0.5), compared with the control group (Table 3). The reduction in physical fatigue exceeded the minimally important difference of 3.85 units, but total fatigue reduction was less than the minimally important difference of 7.9 units. After 10 weeks, nine of 36 participants in the PRT group were categorized as fatigued, compared with 16 of 35 participants in the control group (relative risk ratio = 1.38, 95%CI 0.97–1.98).
At the end of the program, participants in the PRT program had improved in the physical health domain of the quality of life scale compared with the control group (1.5 units; 95% CI 0.1–2.9). The improvement in the physical functioning domain of quality of life was less than the minimally important difference of 2.3 units. There were no differences between the two groups at 10 weeks for cognitive and psychosocial symptoms of fatigue, or for other measures of quality of life.
No further significant between-group differences were identified in any of the per protocol analyses of the secondary outcomes, and very similar estimates of the magnitude of any differences were found. Exploration of the association between change in muscle performance in completers (n = 26) with change in fatigue (MFIS total) and change in the primary outcomes of walking performance (2MWT and fast walking speed) demonstrated a moderate positive correlation between the increase in leg press strength and the increase in fast walking speed (r = 0.47, p = 0.015). There was also a positive correlation between increase in reverse leg press endurance and the increase in the 2MWT (r = 0.42, p = 0.03), and the increase in reverse leg press strength 2MWT (r = 0.39, p = 0.052) approached significance. The increase in reverse leg press endurance was correlated with a reduction in fatigue (r = 0.40, p = 0.04). None of the other correlations between muscle performance and walking performance or muscle fatigue approached significance.
Effects of strength training after 22 weeks
Twelve weeks after training stopped (week 22), participants in the PRT group had not significantly increased the distance they walked over 2 min (–3.4 m, 95% CI –9.5–2.7) or increased their maximum walking speed (0.03 m s−1, 95% CI –0.12–0.06) compared with the control group (Table 3).
At week 22, there appeared to be a significant between-group difference in favor of the PRT group for muscle endurance (reverse leg press endurance 7.3 repetitions, 95% CI 1.9–12.6) (Table 4). However, there were no between-group differences detected for any of the other measures of muscle performance, fatigue and health-related quality of life (Table 4).
Safety and adverse events
No between-group differences were detected after 10 weeks or 22 weeks for symptoms of muscle stiffness or muscle spasm (Table 4). However, compared with the control group, participants in the PRT group demonstrated reductions in symptoms of muscle spasm (−2.8 units, 95% CI −5.6–0.3) (F(1,68) = 3.90, p = 0.052) and muscle stiffness (−2.4 units, 95% CI −5.2–0.5) (F(1,68) = 2.651, p = 0.11) that approached but did not reach significance.
Analysis of the participants’ logbooks showed there were no reports of increases in any sensory symptoms characteristic of MS or of any injury that required participants to miss a training session. The only musculoskeletal problems were short-term muscle soreness reported by most participants (25 out of 36). All cases of muscle soreness were resolved within a few days. No relapses were identified in the training group during the intervention phase of the study serious enough to warrant exclusion of the participant, or for them to miss a training session.
Discussion
Our results suggest that contrary to our predictions, PRT did not improve walking performance in adults with relapsing–remitting MS and mild to moderate walking disabilities. This finding differs from that of a previous high-quality randomized controlled trial 9 which reported that functional outcomes including walking speed over 10 m and walking endurance measured over 6 min improved after completing a supervised 12-week PRT program. The reasons for this disparity in findings are unclear. However, it is possible that the PRT progression model used in the previous randomized controlled trial which applied higher training intensities of up to 8RM (compared with 10–12RM), and larger training volumes of up to four sets of each exercise (compared with our two sets) over a slightly longer duration (12 weeks versus our 10 weeks) than our program could perhaps explain the different findings. On the other hand, it is possible that our research design, which included a comparison group to control for the effects of the increased attention and social interaction inherent in the training program, may have resulted in smaller effect sizes from PRT than that found in the previous trial 9 which examined the effects of PRT simply using a comparison of wait-list control participants.
This latter idea is supported by our per protocol analysis of participants who completed the PRT intervention (attended ≥18 sessions). The per protocol analysis demonstrated moderate positive associations between measures of muscle strength and fast walking speed, and between measures of muscle endurance and walking endurance. In addition, inspection of the between-group differences in walking performance suggested a small, non-significant trend in favor of PRT, as indicated by how close the lower 95% confidence bands were to zero. In combination, these results suggest that if the effect sizes of the current study were maintained and the sample size was larger we may have observed a statistically significant systematic improvement in walking performance in the PRT group. In other words our study may have been underpowered to detect the relatively small effects due to the exercise component of the training program without the added elements of increased attention and social interaction.
The sample size calculation for our study was based on an effect size of d = 0.75 reported in a pilot study. 13 A recent meta-analysis 36 on the effect of exercise on walking ability in people with MS suggested an overall effect size of d = 0.19 (95% CI 0.09–0.28), suggesting our pilot data may have overestimated this effect. Effect sizes calculated from the current experiment (fast walking speed d = 0.31, 95% CI −0.16–0.77; 2-minute walk distance d = 0.27, 95% CI −0.20–0.74) are consistent with this meta-analysis. It is reasonable to expect only small changes in walking ability after a PRT program, particularly from a relatively short program, because muscle strength is only one component that contributes to walking. Therefore implementing PRT to improve walking might be best suited for patients for whom muscle strength is the primary limitation affecting their walking ability.
Despite not observing any changes in walking performance, our results showed that PRT can lead to clinically and statistically significant changes in physical fatigue and in muscle endurance in people with MS. Further, there was a moderate correlation between changes in fatigue and muscle endurance. In addition, PRT can lead to small significant changes in muscle strength and quality of life. These changes are relevant as physical fatigue, poor muscle endurance and muscle weakness are some of the primary symptoms reported by people with MS. In the current study 58% of our participants (41/71) were categorized as being fatigued at baseline. This supports the findings of a previous study that reported 68% of people with MS rated fatigue as one of their worst symptoms, and 44% said they experienced fatigue every day. 37 Also, compared with people without impairment, people with MS demonstrate reduced muscle strength of up to 26%, and have muscles that fatigue about 10% more quickly with repeated contractions. 38
The finding that physical fatigue was improved by PRT and was associated with changes in muscle endurance is important to people with MS, clinicians, and to health services. First, there is no other effective intervention (pharmacological or psychosocial) for fatigue in people with MS. A recent systematic review concluded that the effectiveness of both pharmacological and psychosocial interventions for the treatment of fatigue in adults with MS were modest at best. 39 Our data confirm the results of a smaller randomized controlled trial showing that PRT can reduce fatigue, 10 and therefore it can be used as a viable treatment option for a debilitating symptom. Second, fatigue has a negative effect on the quality of life of people with MS, 40 therefore PRT has the potential to make a significant difference to this key aspect in the everyday lives of this group. Third, people with MS who complain of fatigue are reported to use more hospital outpatient care and primary care services, including rehabilitation, compared with people with mild MS with no fatigue, 41 therefore reducing fatigue in this group has the potential to also reduce health care costs. It is important to note there are different aspects to fatigue: lassitude or feelings of reduced energy, and muscle fatigue or a decline in motor performance during sustained muscle activity. 42 Our results suggest that PRT reduced physical fatigue but had no effect on psychosocial or cognitive fatigue. Therefore, a PRT program is appropriate if people with MS have symptoms of physical fatigue.
There were no adverse events from the program, indicating that it is a relatively safe form of exercise for adults with MS. Most participants experienced muscle soreness during the early weeks of training, but this is expected for participants who had not previously participated in a PRT program. There was no increase in the symptoms of muscle spasms or muscle stiffness; in fact, there was a trend for the symptoms of muscle spasms to improve with training. These findings are consistent with the conclusions of a previous study 43 that showed PRT was a relatively safe intervention for people with a broad range of health conditions.
The training program conducted in this trial is typical of those that members of the community might undertake if they attended their local gymnasium. This is noteworthy because people with disability (including people with MS) may have restricted opportunities to participate in exercise programs taking place in community settings. 44 The training also took the form of small group-based training; this is important because it made exercising a more social activity, and it was more cost effective and time efficient than individual training. Our results suggest a community-based group program, as implemented in this trial, is feasible for people with MS as a therapeutic intervention and as a recreation option. There was good adherence with the training program (92%), compared with the control group’s adherence with the increased attention and social activities program (62%). No participants withdrew from the experimental group once training had started, indicating that PRT was an acceptable form of exercise. However, the follow-up data found that the benefits of the program declined once the program was stopped. This suggests that people with MS need to continue to train to maintain the benefits.
The strengths of our trial were that it was a high-quality randomized controlled trial that assessed the effects of a PRT program conforming to the training guidelines of the American College of Sports Medicine. 7 We used concealed allocation, blinded assessment, random allocation and intention-to-treat analysis to control for many potential sources of bias. Particularly important is that we controlled for the increased attention and social component of the exercise program. This is a limitation of previous studies in this area8–10 and is a common concern with exercise programs. This study adds to the small number of high-quality studies that have investigated if PRT programs are beneficial for adults with MS.8–10
The limitations of this study include that the study only included participants with relapsing–remitting MS who had mild to moderate walking impairment. Therefore, the results may not be generalizable to people with other forms of MS and those with more severe disability. Another limitation is that in designing the trial, we were conscious of selecting only a reasonable number of outcomes for assessment; therefore it is possible that there are other positive or negative outcomes from the program that we did not measure. A further possible limitation is that muscle performance outcomes were assessed using the same equipment participants trained on, therefore improvements in muscle strength and endurance are likely to contain a component of learning. For example, a recent study 9 that measured the maximal isometric knee extensor muscle strength of a group of 15 participants with MS using a dynamometer, and the leg press 1RM using a leg press machine reported pre–post-intervention percentage changes in strength of around 16% (95%CI 4–27) for the isometric measures and 37% (95%CI 27–48) for the 1RM measures. It is possible that learning, together with other components such as the differences in the type of muscle strength measured (isometric versus isotonic strength), differences in the number of exercises that would be expected to influence a composite outcome measure versus a single muscle group outcome measure, and measurement variability inherent in each of the measurement procedures may contribute to these observed differences. Despite this consideration, in the current study a decision was made to use isotonic measures because they better met the principle of specificity of measurement than alternative measures such as dynamometers. In other words isotonic outcome measures better measured the type of strength and endurance the program was trying to improve – a dynamic through-range composite measure of strength and endurance similar to that needed during functional activities such as walking – than dynamometric measures. To minimize possible learning effects, the 1RM and muscle endurance protocols were not practiced during training sessions. Finally, the intervention program was not individualized to the participants’ primary impairments and all the participants completed a similar program targeted at strengthening the major muscles of the lower limbs. It is possible that a program that targets the specific deficits of an individual might be more effective.
Conclusion
PRT performed in a community gymnasium did not lead to improved walking performance, but was effective in the short term in reducing physical fatigue and increasing muscle endurance in people with relapsing–remitting MS and mild to moderate walking difficulty. It also appears to be a feasible and safe fitness option for people with MS that can also lead to small improvements in muscle strength and quality of life. However, benefits do not appear to persist if training is completely stopped.
Footnotes
This work was supported by Multiple Sclerosis Research Australia.
The authors declare that they have no conflicts of interest.