
Abstract
Glatiramer acetate (Copaxone®) is an immunomodulatory polypeptide used in patients with relapsing–remitting multiple sclerosis. It represents a safe treatment option with mild side effects. In this study, we look at a 39-year-old woman who received glatiramer acetate as subcutaneous injections for two months and developed contact dermatitis. The drug had to be stopped, and treatment with topical prednisone was initiated. Prick/scratch testing was negative but the lymphocyte transformation test was highly positive for glatiramer acetate. This is the first report on contact dermatitis induced by glatiramer acetate injections. The treatment consisted of local topical steroids and cessation of the drug.
Keywords
Introduction
Glatiramer acetate (GA; Copaxone®) is used for patients with relapsing–remitting multiple sclerosis as a disease-modifying agent. In general, it represents a safe treatment option. GA is the acetate salt of synthetic polypeptides containing four amino acids (L-alanine, L-glutamatic acid, L-lysine, L-tyrosine). The mechanism of action is not yet fully understood. Several mechanisms of action have been described including competition with antigen for major histocompatibility binding, 1 inhibition of sensitization of lymphocytes to myelin basic proteins in vitro, 2 and induction of Foxp3 expression thus affecting T regulatory (Treg) lymphocytes. 3 T lymphocytes reactive to basic myelin protein were inhibited in terms of proliferation and interleukin-2 (IL-2) production and protective Th2 lymphocytes producing IL-4, IL-6 and IL-10 have been shown to be induced by GA. 3
Common local side effects include immediate reactions with rash, erythema, edema, and pruritus upon injection. In some cases fat tissue necrosis and concomitant lipoatrophy has been described and may lead to discontinuation of the drug. General side effects include transient flush, chest pain, dyspnea and tachycardia a few minutes after injection.
Case report
A 39-year-old female had the first manifestation of demyelinating symptoms 13 years ago. This spring, she experienced a severe relapse caused by myelitis (Expanded Disability Status Scale [EDSS] 3.0). MRI demonstrated two lesions in the cervical spine, one of which showed gadolinium enhancement. Relapsing remitting multiple sclerosis was diagnosed and a disease-modifying therapy with interferon-β (IFN-β) 1b subcutaneously (s.c.) every second day was initiated. After 4 weeks, IFN-β treatment had to be stopped due to liver enzyme elevation exceeding five times the upper normal limits (liver enzymes were normal before IFN-β initiation). The treatment was switched to GA s.c. daily. The patient was not on any medication other than GA.
After 2 weeks of s.c. self-injection without any adverse effects the patient noticed that 2–3 days after each injection, an erythema with maculopapular rash and scaling occurred. Subsequently, the lesion increased in size and eczema developed at nearly every injection site. The clinical picture showed symmetric erythemato-squamous plaques 6–10 cm in diameter of size on abdomen, thighs and buttocks which occurred at nearly every injection area (depicted in Figure 1). A skin biopsy was taken and showed an eczematous epidermis with acanthosis, spongiosis and parakeratotic keratosis. Subepidermally, a perivascular inflammatory infiltrate with some neutrophils could be observed. Some eosinophils presented in the dermis (depicted in Figure 2).

Skin changes at the injection sites of glatiramer acetate: Sharply demarcated eczematous lesions with palpable infiltrate on each injection side corresponding to contact dermatitis.
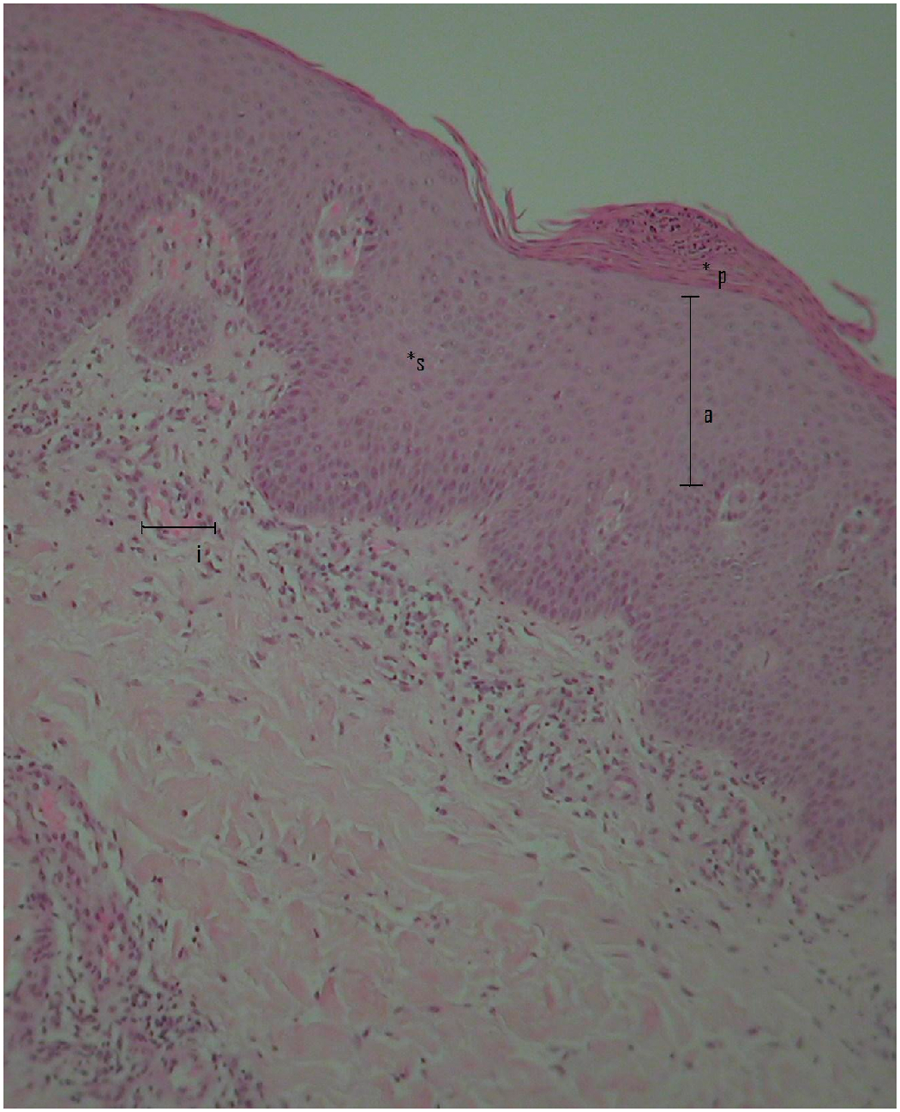
Histological picture with acanthosis (a), spongiosis (s) and parakeratotic keratosis (p). Subepidermally, perivascular inflammatory infiltrate (i) (hematoxylin–eosin staining; magnification × 100).
Initially, topical steroids (Class II) and a topical H1 blocker were given but the skin changes did not improve. GA was stopped and treatment with local class IV corticosteroids and a moisturizing product as well as a systemic H1 blocker against the pruritus were initiated. This course of treatment led to fast improvement of the skin.
Allergologic evaluation included a scratch/patch test with the drug as well as a lymphocyte transformation test (LTT) with GA (Copaxone®), as there was no other suspected medication. The scratch/patch testing 2 months after the drug reaction showed no reaction except for positive histamine control.
Positive scratch tests might become negative with more time passed. It is however highly unlikely that a scratch test that was negative 2 months after the drug reaction will become positive after a year. Thus, scratch testing was not repeated since negative scratch tests rarely turn positive after a longer interval after the drug reaction.
The LTT was performed 9 weeks after the onset of the skin reaction and 6 weeks after stopping the drug intake. It was performed after 6 days of stimulation with GA concentrations of 0.001–500 µg/ml. At the concentration of 100 µg/ml GA, a stimulation index of 17.7 (cut-off SI < 2) was measured, at 10 and 1 µg/ml the SI was 37.2 and 30.1, respectively.
An extremely strong increase of the lymphocytic proliferation was documented at 500 µg/ml GA with a stimulation index of 45.8. These values were even higher when proliferation assays were performed with AB serum with SI up to 107.8.
GA is known to induce T-cell stimulation in GA-naive patients. 4 Farina et al. 5 showed stimulation indices of a mean of 3 (ranging from 1 to 9) in healthy donors after 5 days of stimulation for GA concentrations of 6.25–100 µg/ml. On the other hand GA-treated patients (mean duration of treatment 25 months) showed a decreased SI to a mean of 1 (range 0.7–3). Brenner et al. 6 measured stimulation after 5 days at doses of 5 µg/ml GA and showed a slight increase of SI 1 month after treatment (from SI 11.3 to SI 13) followed by a subsequent decline to an SI of 8.5 after 3 months which further decreased in the subsequent months.
The LTTs performed here are comparable with respect to stimulation time and concentration. Even though a slightly elevated SI in the LTT would not be relevant for Copaxone®, the stimulation indices detected here of up to 45.8 and 107.8 are quite remarkable.
Discussion
This is the first report of contact dermatitis induced by GA. It represents a T-cell-dependent type IVc drug reaction which after sensitization to the drug leads to an inflammatory lymphocyte-dependent reaction. T lymphocytes migrate to the injection-site express perforin, granzyme B, and Fas Ligand, which are cytotoxic molecules and induce apoptosis in keratinocytes. 7 This may be the underlying process behind the contact dermatitis observed in our case.
To the best of the authors’ knowledge this is the first case of contact dermatitis induced by GA. There is only one previous report describing another delayed-type hypersensitivity reaction induced by GA which presented as subcutaneous nodules. 8 In this case, the scratch/patch and intracutaneous test were positive and the histology showed a lymphocytic and eosinophilic infiltration. More commonly, GA induces immediate transient general side effects such flush chest pain and dyspnea a few minutes after injection. 9 Dermatological side effects include immediate local side effects such as rash, erythema, edema, and pruritus. These can be minimized by application of ice 30–60 seconds before application, or by the use of topical anesthetics. 10 Rarely, necrotizing cutaneous lesions after injection of GA have been seen with ischemic cutaneous necrosis comparable to local thrombotic microangiopathy induced by interferon injections. Furthermore, a lobular, localized panniculitis and concomitant lipoatrophy has been described and single case reports exist on urticaria vasculitis, erythema nodosum, Jessner Kanof infiltration, primary cutaneous CD + 30 T-cell lymphoma and a livedo-like dermatitis (Nicolau’s syndrome) which all occurred after the GA injections. A reversible alopecia has also been described.
Interestingly, in our patient an extreme increase in lymphocyte proliferation was observed upon stimulation with GA. This is in contrast to previous publications which have shown a significant decrease of lymphocyte proliferation upon stimulation with GA.5,6
GA is used in patients with relapsing–remitting multiple sclerosis. In clinical trials it reduced the relapse rate and the affecting disability and is generally considered a safe treatment option. In this patient the drug had to be discontinued due to the contact dermatitis induced.
Conclusion
Contact dermatitis is a rare side effect of GA and may lead to a discontinuation of treatment. Oral treatment options of multiple sclerosis might be helpful in these patients.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None of the authors have a potential conflict of interest with any of the content of this article.