
Abstract
Introduction
The possibility of a link between migraine and multiple sclerosis (MS) was suggested over half a century ago by Compston and McAlpine who observed that 2% of patients with MS experienced migraine within 3 months of MS onset. 1 Since then, nine case–control studies have been conducted with the aim of determining whether migraine prevalence is increased in MS patients. In five of these studies migraine was more common in MS patients than healthy controls or non-MS neurological controls,2–6 while the other four studies found no increase in migraines among MS patients.7–10 The prevalence of migraine among MS patients ranged from 21% to 69%. The relatively wide range and conflicting results are perhaps not surprising given differences in study methodology (e.g. lifetime prevalence versus point prevalence), case definitions, timing, location, patient and control selection, and small sample size.
The studies of migraine in MS suffer from two main limitations: they are cross-sectional surveys and thus do not yield information regarding the temporal relationship between migraine and MS; all but one of these studies 9 were tertiary clinic-based and are therefore subject to selection and Berkman’s biases. 11
A methodologically rigorous, large-scale, non-clinic-based, prospective study could help resolve the controversy of whether migraine is associated with MS and shed light on the temporal relationship between the two disorders. Therefore, we sought to examine the association between MS and migraine among women in the Nurses’ Health Study II (NHS-II), a prospective cohort of over 116,000 women that has been extensively used to investigate risk factors in MS.12–17
Materials and methods
Participants
The NHS-II is a cohort of 116,671 female, married, registered nurses, aged 25–42 years and living in one of 14 states across the US. The women completed an enrollment questionnaire in 1989 and updated their medical and lifestyle information via questionnaire every 2 years thereafter.
Ascertainment of MS diagnosis
The ascertainment of MS cases has been described previously. 16 In brief, women who self-report an MS diagnosis were asked for permission by study investigators to contact their treating neurologist and obtain a copy of medical records pertaining to the diagnosis. In a validation study of cases diagnosed before 2001, when study neurologists applied Poser criteria for diagnosis of MS to the clinical and laboratory data, 93% of all definite and probable diagnoses were confirmed. 16 Thus, women are considered as having definite or probable diagnosis of MS according to Poser criteria as reported by the neurologist or after review of medical records by the study neurologist if confirmed between 1989 and 2001. The McDonald criteria for MS were introduced in 2001, and consequently all cases of self-reported MS occurring between 2002 and 2005 were assessed by a study neurologist in order to determine whether they met the 2001 McDonald criteria. At baseline in 1989, 140 women had MS (‘prevalent cases’). Between 1989 and 2005, there were 402 new diagnoses of probable or definite MS (‘incident cases’). Among the incident cases, 244 had MS symptom onset after 1989 and 114 had symptom onset before 1989, but were diagnosed after 1989, while 44 had an unknown date of symptom onset. The subset of 244 incident cases who developed MS symptoms after the baseline will be referred to as ‘MS onset after baseline cases’.
Migraine status
In 1989 (baseline), 1993, and 1995, women were asked to report whether they ever had a physician-diagnosed migraine headache.
Covariates
Multivariate analyses were adjusted for latitude of residence age 15 (north, middle, south), ethnicity (Scandinavian, Southern European, other Caucasian, other), pack-years smoking (never, <10, 10–24, >24), body mass index (BMI) at age 18 (<18.5 kg/m2, 18.6–20.9, 21–22.9, 23–24.9, 25–26.9, 27–29.9, ≥30), and supplemental vitamin D intake in 1991 (0, <400 IU/day, ≥400 IU/day) as described previously.14,17
Statistical analysis
Comparisons of migraine prevalence in MS cases versus non-cases were performed using a chi-squared test. In the prospective analyses examining the risk of MS associated with history of migraine, women were followed from the date they returned the baseline questionnaire to the earliest of: date of MS diagnosis (or onset), date of death, or June 2005. Analyses were conducted using report of migraine at baseline and ever reporting migraine (1989, 1993, or 1995). Cox proportional hazards regression stratified by age (in months) and 2-year time periods (frequency of the questionnaires) was used to estimate rate ratios (RRs) and 95% confidence intervals (CIs).
We also conducted analyses examining whether women with MS were more likely to have migraine headaches. This analysis excluded any case of MS that onset after 1989 (n = 244) and any woman who reported having physician-diagnosed migraine in 1989 (n = 17,893). This restriction increased the likelihood that the MS preceded the migraine. Because we do not have information on the date of migraine diagnosis, we could not perform a prospective analysis using Cox proportional hazards regression. Instead, we used multivariate logistic regression, adjusted for the same variables as above (age, latitude of residence, ethnicity, smoking history at baseline [ever versus never], BMI at age 18, supplemental vitamin D) to estimate the odds ratio of being diagnosed with migraine in women with and without pre-existing MS.
Analyses were conducted using SAS software, version 9.1 (SAS Institute Inc, Cary, NC). A p-value <0.05 was considered significant.
The study has been approved by the institutional review board of Brigham and Women’s Hospital, Boston.
Results
Prevalence of migraine in the NHS-II
At baseline, 17,893 (15.4%) women reported having physician-diagnosed migraine. There were no differences between migraineurs and non-migraineurs with respect to age, BMI at age 18, latitude of residence at age 15, Scandinavian ancestry and smoking status (Table 1). By 1995 an additional 6407 women reported a physician-diagnosed migraine. ‘Cumulative migraine prevalence’ in the NHS-II through 1995 was 20.9%.
Characteristics of women with and without physician-diagnosed migraines
BMI, body mass index
Frequency of migraine among prevalent MS cases
At baseline, 140 women (0.1% of the sample) had a diagnosis of MS (‘prevalent MS cases’), and 27 of them (19.3%) had a co-existing diagnosis of migraine. As of 1995, the last available migraine status update in NHS-II, 10 additional prevalent MS cases reported being diagnosed with migraine by a physician. Thus, the number of migraineurs in the prevalent MS group rose to 37 (26%), which is higher than the cumulative prevalence of migraine among non-MS cases (21%), although the difference did not reach significance (p = 0.11).
The prevalence of migraine at baseline and at last migraine status follow-up (in 1995) in the non-MS, ‘prevalent MS’, ‘incident MS’ and ‘MS onset after baseline’ groups is shown in Figure 1.
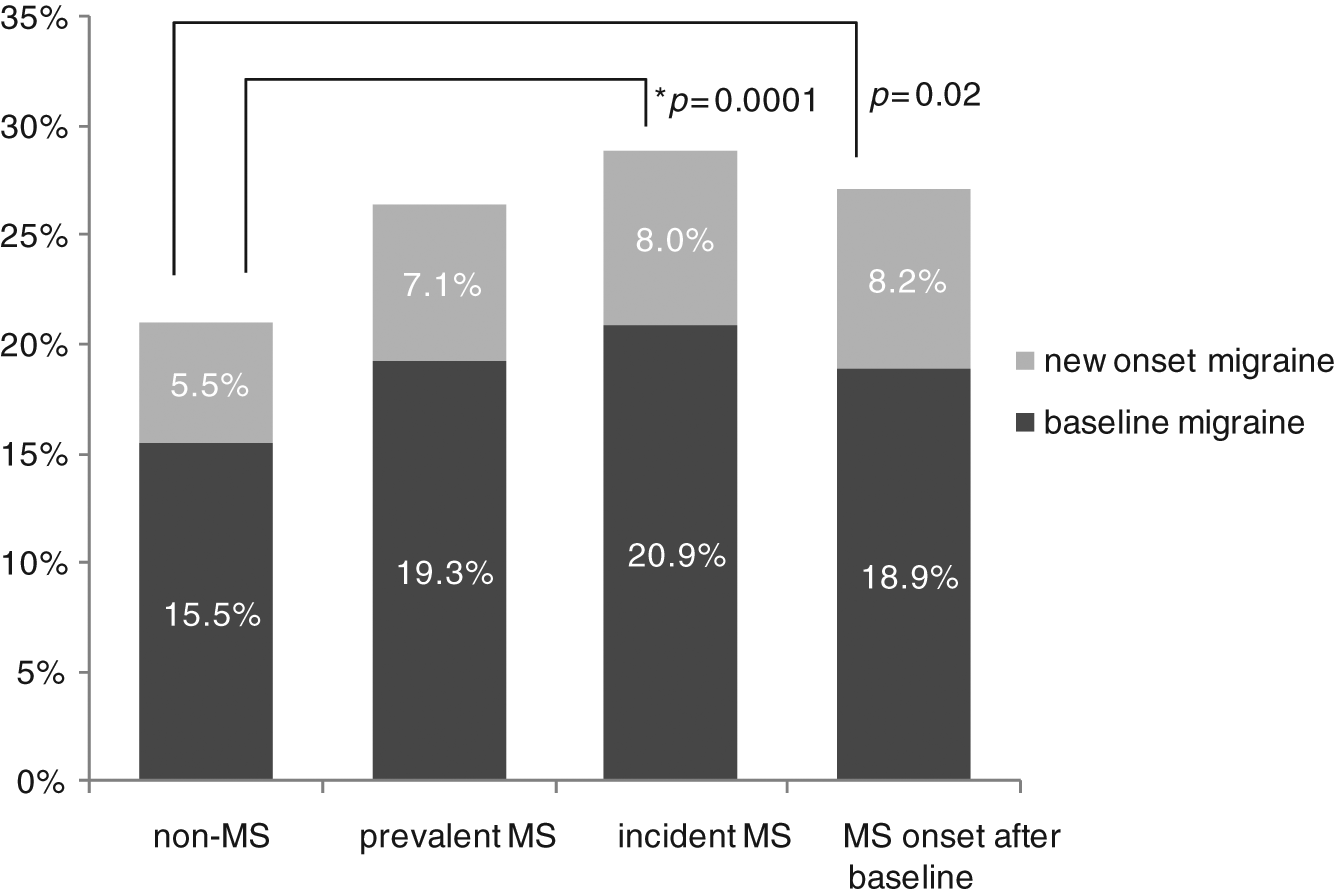
Baseline and cumulative migraine prevalence in multiple sclerosis (MS) patients and controls. ‘Baseline migraine’ (dark bars) represents migraine prevalence at the time of enrollment into NHS-II in 1989. ‘New Onset Migraine’ (lighter bars) represents percentage of enrollees who were diagnosed with migraine between 1989 and 1995. ‘Prevalent MS’ and ‘incident MS’ are two non-overlapping cohorts. ‘MS onset after baseline’ refers to subset of the incident MS cases with symptom onset after baseline.
Frequency of migraine among incident MS cases
There were 402 women who were diagnosed with MS after the baseline (‘incident MS cases’), of whom 84 (20.9%) had a pre-existing diagnosis of migraine. In analyses adjusted for age, BMI at age 18, smoking history, vitamin D intake, latitude of residence and ancestry, women who reported having a history of migraine at baseline had a 39% increased risk of MS (p = 0.008) (Figure 2). The difference in absolute risk of developing MS among women with migraine at baseline and those without was small: 0.47% (84 out of 17,893) in migraineurs versus 0.32% (318 out of 98,778) in non-migraineurs over 15.5 years of follow-up.
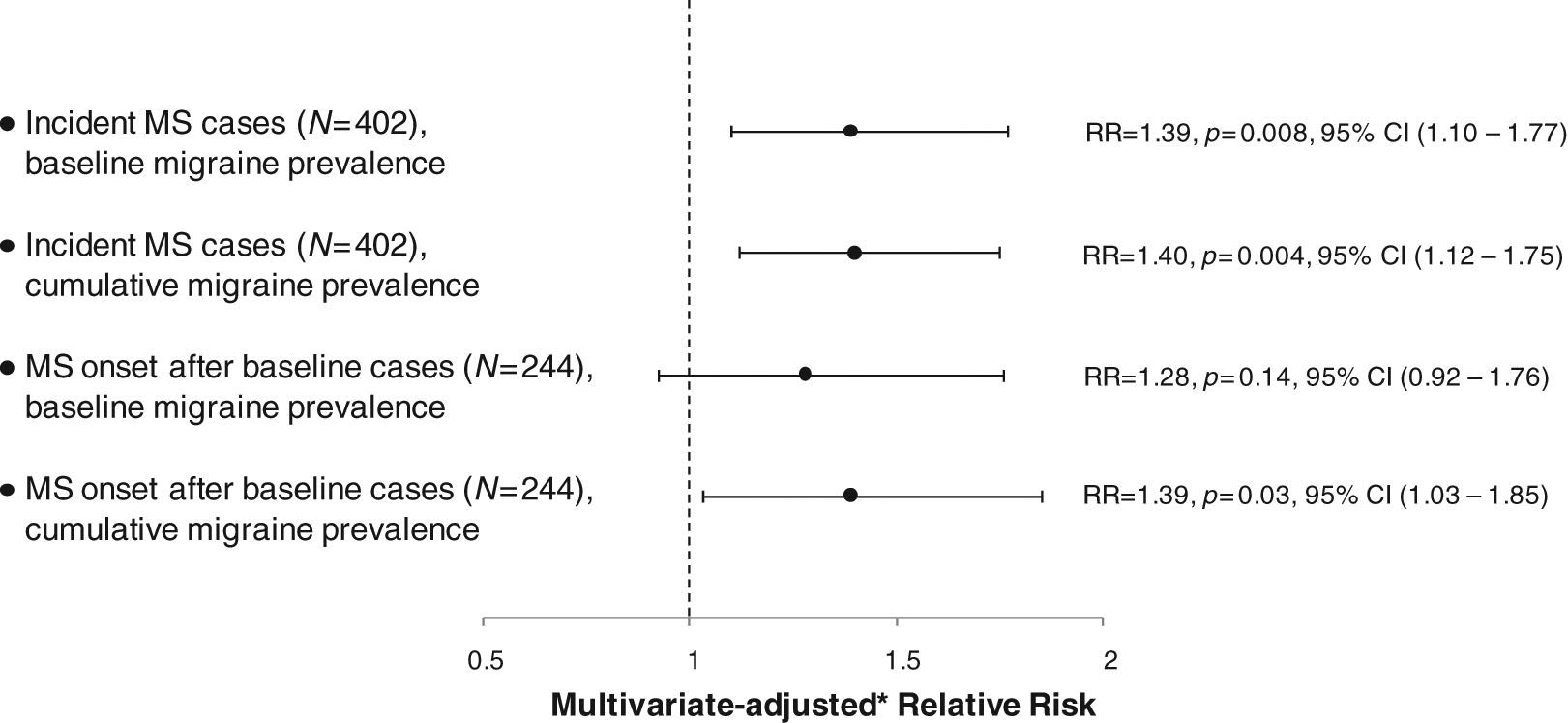
Relative risk of multiple sclerosis (MS) in women with pre-existing migraine. *Multivariate: age (months), latitude of residence age 15 (north, middle, south), ethnicity (Scandinavian, Southern European, other White, other), pack-years smoking (never, <10, 10–24, >24), BMI at age 18 supplemental vitamin D in 1991(0, <400 IU/day, ≥400 IU/day). RR, relative risk; CI, confidence interval.
In addition to the 84 cases in the incident MS group with a diagnosis of migraine at baseline, 32 new cases of physician-diagnosed migraine were reported as of 1995, for a total of 116 migraine cases, yielding a cumulative migraine frequency in the incident MS cohort of 28.9%.
Of the 32 de novo migraine diagnoses, 21 were reported prior to MS diagnosis and 11 after MS diagnosis. Thus, in the group of women with incident MS and migraine, 91% (105/116 women) were diagnosed with migraine before they were diagnosed with MS.
Frequency of migraine in the ‘MS onset after baseline’ cases
Of the 402 women in the incident MS cohort who were diagnosed with MS after baseline, 244 experienced their first symptom of MS after baseline (‘MS onset after baseline cases’). The remainder of the incident cohort, 158 cases, either had symptom onset before the baseline (114 cases) or an unknown symptom onset date (44 cases). In 1989, frequency of migraine among the cases with MS onset after baseline was 18.9% (46/244). During the period 1989–1995, an additional 20 women in the MS onset after baseline subset reported physician-diagnosed migraine, resulting in a cumulative migraine frequency of 27.1% (66/244). Of the 20 new migraine cases, 14 developed migraine before first MS symptoms and 6 after MS symptoms. Thus, among women with migraine and MS onset after baseline, 91% (60/66) received migraine diagnosis prior to the first symptom of MS.
In analyses adjusted for age, BMI at age 18, smoking history, vitamin D intake, latitude of residence and ancestry, women in the MS onset after baseline subset who reported having a history of migraine at baseline had a 28% increased risk of MS compared with non-migraineurs, which was not statistically significant (RR = 1.28; 95% CI 0.92–1.76, p = 0.14). However, when the analysis was carried out using updated migraine prevalence (as of 1995) rather than baseline migraine prevalence, the migraineurs had a 39% increased risk of MS as compared with women with no migraine history, which was a statistically significant difference (RR = 1.39; 95% CI 1.03–1.85, p = 0.03). The relative risks of MS among incident MS cases and MS onset after baseline cases using both baseline and cumulative migraine prevalences are shown in Figure 2.
Relative risk of new migraine diagnosis in patients with and without pre-existing MS
To better understand the interrelationship between migraine and MS, one needs to consider not only whether migraine occurs more frequently among women who will develop MS, but also the reciprocal question of whether women with MS are more likely to develop migraines. To address the latter question, we estimated the odds of having a physician-diagnosed migraine by 1995 in women with no migraine, but positive MS history at baseline. ‘Positive MS’ history was defined either as a diagnosis of definite/probable MS at baseline, or symptom onset before baseline.
In the subset of 113 patients with pre-baseline diagnoses of MS, but no history of migraine at baseline in 1989, ten women were diagnosed with migraine by 1995 (8.9%), while in the no MS/no migraine cohort of 98,099 women, 697 were diagnosed with migraine by 1995 (6.5%). Thus, women with pre-existing MS compared with women with no MS had a 33% increased odds of being diagnosed with migraine during follow-up, but this difference was non-significant (p = 0.4) (Table 2).
Multivariate* odds ratio of a first migraine diagnosis between 1989 and 1995 in women with and without pre-existing multiple sclerosis, among women who reported never having a migraine before 1989

Multivariate: adjusted for age (months), latitude of residence age 15 (north, middle, south), ethnicity (Scandinavian, Southern European, other White, other), smoking (never versus ever at baseline), BMI at age 18 (<18.5 kg/m2, 18.5 to <25, 25 to <30, ≥30), supplemental vitamin D in 1991 (0, <400 IU/day, ≥400 IU/day).
MS, multiple sclerosis; OR, odds ratio; CI, confidence interval; BMI, body mass index.
In the subset of cases with MS symptom onset before baseline, 9 out of 73 women were diagnosed with migraine between 1989 and 1995 (12.3%). Since in the no MS/no migraine at baseline group, 6.5% were diagnosed with migraines during 1989–1995 follow-up, the odds ratio of developing MS was 1.9-fold higher in the MS symptom onset group, which trended to, but did not reach statistical significance (p = 0.07) (Table 2). Combining the prevalent MS and ‘MS symptom onset before baseline’ groups, the odds ratio of new diagnosis of migraine among MS patients compared with non-MS patients was trending toward significance (p = 0.06) (Table 2).
Discussion
Analysis of NHS-II, a large cohort of women, provides the strongest evidence to date for an existence of an association between migraine and MS. The cumulative prevalence of migraine among two non-overlapping cohorts of MS patients in NHS-II, ‘prevalent MS cases’ and ‘incident MS cases’, was higher than in the non-MS cases. The relatively modest differences in migraine frequency in the MS and non-MS groups, 26–29% in the MS groups versus 21% in non-MS patients, may explain why previous, smaller studies of migraine in MS, being likely under-powered, yielded conflicting results. However, as migraine estimates in NHS-II are only current as of 1995, they should be considered as the ‘lower bound’ of cumulative prevalence. The true prevalence through the end of the follow-up period in 2005 would likely be higher in all groups, and would likely widen the gap between MS and non-MS groups.
The prospective nature of the NHS-II cohort allowed us to investigate the temporal relationship between migraine and MS. In this respect the most instructive results emerge from analysis of the ‘MS onset after baseline’ cases. These women developed MS during the follow-up period, and their migraine status was ascertained prior to the first symptom of MS. The women with pre-existing migraine had a statistically significant 39% higher risk of developing MS compared with non-migraineurs. It is important to emphasize, however, that the absolute risk of MS among women migraineurs was small, 0.47%, which was only 0.15% higher, in absolute terms, than in non-migraineurs over the 15.5 years of follow-up. Migraine can therefore be considered a predictor of MS, but a relatively modest one compared with the more established risk factors such as DRB1*1501 haplotype 12 or history of infectious mononucleosis. 18
What can account for the higher rate of MS among women with migraine compared with those without? One possible explanation is that the association is due to errors in diagnosis of MS in migraineurs: women with migraine may have been more likely to be seen by a neurologist, evaluated with brain MRI, and misdiagnosed with ‘MS’ on the basis of non-specific radiographic findings in combination with a history of transient (usually) visual or sensory neurologic deficits. We consider this scenario to be unlikely for two reasons: first, in an overwhelming majority of cases, all cases reported before 2001, the diagnosis of MS was made according to non-MRI-based Poser criteria, which are considered to be more specific for MS than the (partly) MRI-based McDonald criteria; secondly an association between migraine and MS was found also among women with a definite diagnosis of MS (data not shown). It could also be argued that the association may be due to detection bias: 19 abnormalities on brain MRI in a migraine patient would lead to greater scrutiny of the patient’s past neurologic history and subsequent symptoms, and would facilitate an earlier diagnosis of MS compared with non-migraineurs, who might not come to attention of a neurologist until more obvious signs of MS are manifest. We believe that this consideration is also unlikely to have significantly influenced the results since, as mentioned previously, most cases in the NHS-II were diagnosed using Poser criteria, which do not take into consideration MRI findings. Furthermore, the age at diagnosis of MS in migraineurs (42.5 years) and non-migraineurs (42.1 years) was similar in our cohort.
Another interpretation for the apparent higher risk of MS among migraineurs is that migraine-like headache may be the presenting symptom of MS, rather than a concurrent diagnosis. Headache is not usually considered an MS symptom, although it is the most common indication for brain MRI in ‘radiographically isolated syndrome’ 20 and has been reported at MS onset in 1–2% of patients.1,27 The available data does not allow us to determine whether migraine in a ‘pre-symptomatic’ MS phase is a primary or secondary headache, but the fact that migraine generally predates MS by many years, and the rarity of migraine at MS onset would seem to indicate that in most cases migraine is more likely to be a pre-existing diagnosis.
Our results that migraine increases the risk of subsequent MS are in line with two previous small case–control studies.5,6 A number of potential mechanisms may account for this observation. One possibility is that migraine, and specifically migraine with aura, may lead to subtle increase in permeability of the blood–brain barrier and neuroinflammation, 21 thereby exposing antigen in the privileged central nervous system compartment to circulating T cells and contributing to their sensitization to myelin products. This model might explain how a non-immune-mediated condition such as migraine might play a role in the pathogenesis of presumably autoimmune disease, such as MS. Unfortunately, we did not have information in this study on whether the migraine was with or without aura. This hypothesis, purely speculative at present, lends itself to experimental verification. It is also possible that migraine may skew cytokine profile in a way that may predispose to autoimmune reaction in CNS. In this connection it is interesting to observe that certain cytokines, such as interleukin 10 (IL-10) and tumor necrosis factor alpha (TNFα), tend to be elevated in both migraine attacks and during an MS relapse.7,26 Other possibilities will need to be considered as well, such as the existence of shared environmental and genetic risk factors. 22
We also observed a trend for migraine to be diagnosed more frequently in MS patients compared with non-MS cases, but this trend did not reach statistical significance. Various hypotheses have been put forth to explain how MS can predispose to migraine, 23 but the antecedent question of whether or not such a predisposition exists cannot be established with the evidence at hand.
Our study has a number of strengths compared with prior investigations of MS and migraine. The diagnoses of MS were validated through a study neurologist and review of records; the study involves a large, non-clinic-based sample; it employs a prospective cohort design, which allowed us to ascertain the temporal order of emergence of migraine and MS in a subset of enrollees. There are also several limitations. First, the NHS-II enrolled only women of similar professional and socio-economic background, nearly all of whom were White. Thus, our results may not be generalizable to MS patients with different demographic characteristics (men, non-Whites, older patients, etc.). On the other hand, the prevalence of migraine in our sample of women was nearly identical to that in the large Internet-based National Health and Wellness Study, in which migraine was reported by 29% of respondents with MS, a significantly higher rate than among non-MS cases. 24 The second limitation is that the diagnosis of migraine was based on self-report, but did not make use of a validated diagnostic tool for patient-reported migraine, such as the one used in the American Migraine Prevalence and Prevention (AMPP) study. 25 The detailed nature of the instrument used in the AMPP made impractical its inclusion in the NHS-II questionnaire, which asks targeted questions about wide range of medical conditions. It is hoped that the number of false-positive and false-negative responses has been kept to a minimum by restricting the study to medical professionals who would be expected to have increased awareness and better understanding of migraine and easier access to health care compared with the general population. It was reassuring that self-reported migraine prevalence in NHS-II among non-MS cases was within the range of what was reported by women in the general population in the AMPP: 28.1% in the 30–39 age group and 25.5% in the 40–49 age group. 25 Another limitation of our study relates to the lack of information about migraine onset and migraine type which precluded more in-depth analyses of the temporal interrelationship between various migraine types and MS.
In conclusion, our work confirms the existence of an association between migraine and MS that was previously reported by some,2–6,24 but not all investigators. It also supports the idea that migraine is a risk factor for, or at least a predictor of, MS as suggested by two small case–control series.5,6 Further research is needed to test the various hypotheses that may explain the association between migraine and MS.
Footnotes
Acknowledgements
The authors wish to thank Ms Tamar Bacon for her kind assistance in copyediting the manuscript and the preparation of tables and figures. Statistical analyses were carried out by Kassandra L Munger, ScD, Harvard School of Public Health, MA, USA.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ilya Kister, MD, received research support from EMD-Serono/Pfizer, Inc. and the National Multiple Sclerosis Society. Joseph Herbert, MD, has received personal compensation for activities with Biogen Idec, EMD Serono, Teva Neuroscience and Bayer as a consultant. Dr Herbert has received research support from Teva Neuroscience, Novartis, Biogen Idec, Bayer, EMD-Serono/Pfizer, BioMS and INC Research. Kassandra L Munger, ScD, has received travel expenses and honoraria for presentations from the Consortium of MS Centers and the National MS Society. Alberto Ascherio, MD, DrPH, receives research funding from the National Institutes of Health, the Department of Defense, the Michael J Fox Foundation, and the National Multiple Sclerosis Society. He received prior funding from Autism Speaks and honoraria for two scientific presentations to Merck Serono.