
Abstract
Natalizumab is a humanized monoclonal antibody directed against the alpha-4 integrin subunit of very late activation antigen-4 (VLA-4). Natalizumab neutralizing antibodies (NAB) have been found to significantly reduce beneficial effects of natalizumab treatment in multiple sclerosis. We investigated interactions of NAB with natalizumab by serial measurements of alpha-4 integrin levels on peripheral blood mononuclear cells using flow cytometry. In addition, serum concentrations of soluble vascular cell adhesion molecule-1 (sVCAM-1), the endothelial ligand of VLA-4, and serum NAB were serially determined. Natalizumab infusion led to a transient reduction in alpha-4 integrin levels on immune cells and serum sVCAM-1 levels along with serum negativity of NAB lasting for a few days post-infusion. Apparently, the high-dose effect of freshly infused natalizumab resulted in a transient neutralization of NAB possibly involving a transient therapeutic effectiveness.
Introduction
Natalizumab is the first humanized monoclonal antibody approved for treatment of relapsing–remitting multiple sclerosis (RRMS) and is directed against the alpha-4 integrin subunit of very late activation antigen-4 (VLA-4). Natalizumab inhibits migration of immune cells across the blood–brain barrier into the central nervous system (CNS) by blocking the interaction of leukocyte VLA-4 with its endothelial ligand vascular cell adhesion molecule-1 (VCAM-1). 1 An impressing efficacy in reducing relapse rates and preventing disability progression has been shown.2,3 However, similar to other protein therapeutics, neutralizing antibodies (NAB) against natalizumab might develop during therapy. NAB have been detected in 9% of natalizumab-treated patients, of whom 3% were transiently and 6% were persistently positive. 4 As reported by Calabresi et al., high-titre NAB are highly indicative for persistent NAB. Patients with persistent NAB were seen to have a reduced benefit from natalizumab therapy, presumably to interference with drug binding to the alpha-4 integrin subunit and an increased drug clearance. Moreover, these patients have been reported to develop infusion-related allergic reactions more frequently. 3 In particular, if an individual patient seems to benefit from natalizumab therapy, it is difficult to decide to stop natalizumab treatment. On the other hand, it is questionable whether the individual benefit exceeds the higher risk of allergic adverse events.
In previous studies we have shown that natalizumab therapy significantly reduces alpha-4 integrin levels on immune cells as determined by flow cytometry. 5 Here, we approached the question whether natalizumab has any effect on immune cells despite the presence of NAB by serial determinations of alpha-4 integrin levels on peripheral blood mononuclear cells (PBMC) and serum concentrations of soluble VCAM-1 (sVCAM-1) levels between two natalizumab applications in a patient with RRMS who had developed NAB. Results were compared with those of a natalizumab-treated RRMS patient without NAB and a healthy control person.
Patients and methods
Two patients were diagnosed with clinically definite MS according to the revised McDonald criteria. 6 Patients received the standard dose of natalizumab (300 mg i.v.) every 4 weeks. PBMC from both patients were collected prior to the first, fourth and seventh natalizumab infusions and at days 1, 2, 4, 8, and 11 post-infusion (patient with NAB) or days 1, 4, 8, and 11 post-infusion (patient without NAB), respectively. PBMC from a healthy volunteer were collected serially at about 4-day intervals. All participants gave written informed consent and the study was approved by the local ethics committee.
Venous blood was collected in commercial PBMC enrichment tubes (Becton Dickinson AG, Basel, Switzerland) and stained with saturating amounts of fluorescence-conjugated monoclonal antibodies CD3+ (clone UCHT1, PE), CD19+ (clone J4-119, PE), CD14+ (clone RM052, PE), and CD49d (clone HP2/1, FITC). Isotype-matched and CD45+ (clone J33, FITC/PE) antibodies were used as negative and positive controls, respectively. With the exception of IgG1-FITC/PE (Exalpha, Watertown, MA, USA) all antibodies were obtained from Beckman Coulter, Vienna, Austria. Relative fluorescence intensity levels were calculated from median fluorescence intensities of all leukocyte subpopulations as previously described. 7
Serum levels of sVCAM-1 were determined by fluorescent bead immunoassay using the Human Adhesion 6-Plex Kit FlowCytomix Kit (eBioscience, Vienna, Austria).
Determination of anti-natalizumab NAB was performed from sera collected before infusions and at days 0,1, 4, and 11 post-infusion at the Department of Neurology, Innsbruck Medical University, Austria. 8
Results
A highly active clinical course despite immunomodulatory therapy with interferon beta-1a necessitated a switch to natalizumab in a 35-year-old female patient with RRMS. In addition to routine clinical examinations of patients during natalizumab treatment, we determined alpha-4 integrin expression on PBMC and serum levels of sVCAM-1 before the first, fourth, and seventh natalizumab infusions. In the 35-year-old patient, cellular alpha-4 integrin levels and serum levels of sVCAM-1 apparently were not affected by natalizumab treatment as they resembled baseline levels even before the fourth and seventh infusion (Figure 1A, 1C). This was highly indicative for NAB, which were confirmed to be high-titre positive (> 1:100) by anti-natalizumab NAB testing.
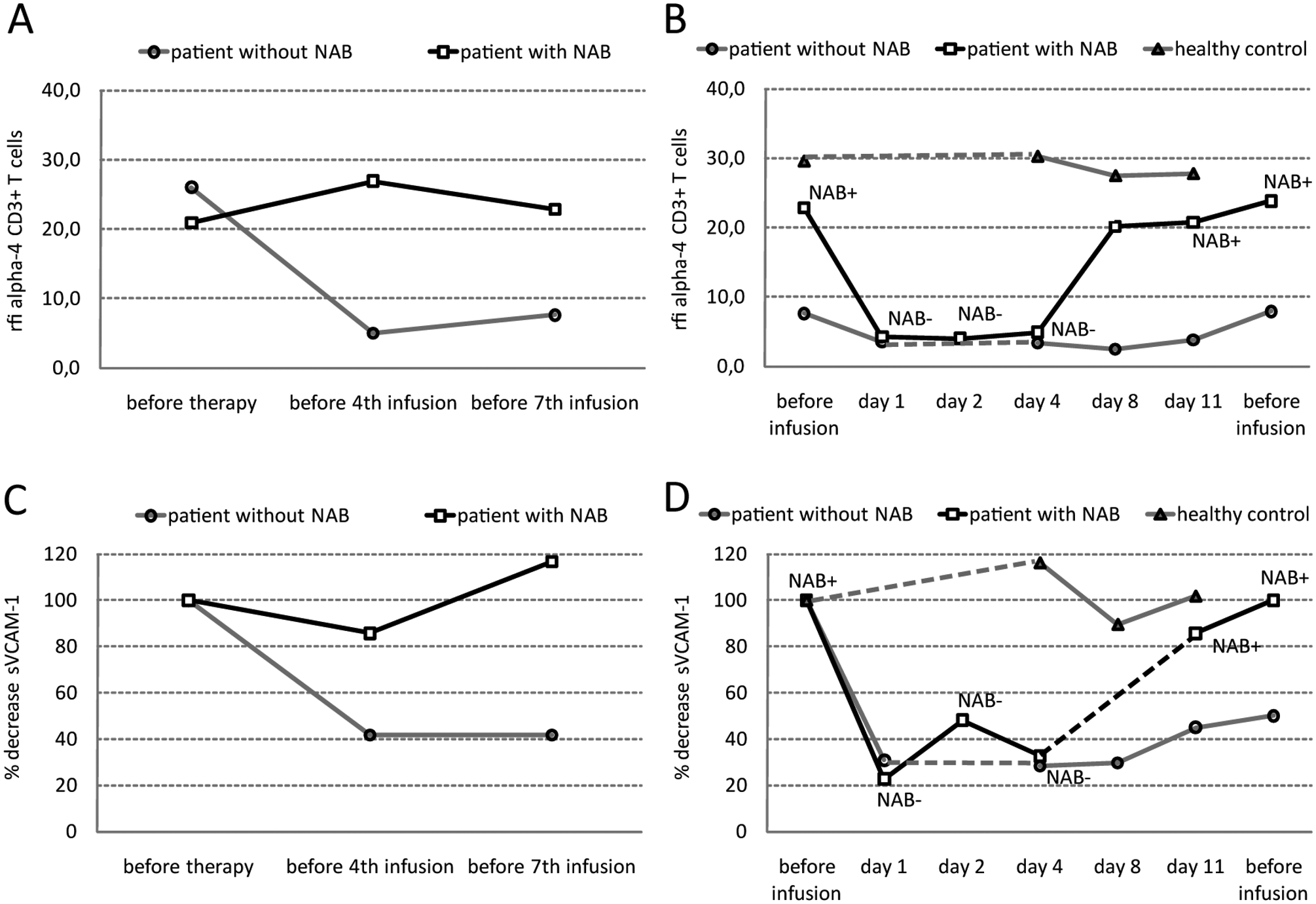
Effects of natalizumab treatment on immune cell alpha-4 levels and serum concentrations of sVCAM-1 in natalizumab-treated RRMS patients with (open squares) and without (open circles) NAB and a healthy control person (open triangle). Left panel: detectability of alpha-4 integrin levels on CD3+ T cells (A) and % decreased serum concentrations (baseline = 100%) of sVCAM-1 (C) before the first, fourth and seventh natalizumab application. Right panel: serial determination and short-term changes of post-infusion alpha-4 integrin levels on CD3+ T cells (B) and % decreased sVCAM1 serum concentrations (baseline = 100%) (D). Dashed lines represent skipped measurements between two time-points. Abbreviations: rfi, relative fluorescence intensity; NAB, anti-natalizumab neutralizing antibodies; RRMS, relapsing–remitting multiple sclerosis.
We decided to continue natalizumab therapy after comprehensive information of the patient because natalizumab applications were well tolerated and the patient was relapse free. To obtain a better understanding of the chronology of the interactions of natalizumab and NAB, we serially studied alpha-4 integrin levels, serum concentrations of sVCAM-1 and NAB between two consecutive natalizumab infusions (Figure 1B, 1D). One day post-infusion we found significantly decreased alpha-4 integrin levels on all investigated PBMC subsets (T cells, B cells and monocytes) and significantly decreased serum sVCAM-1 levels in the patient who was NAB positive. This effect was still observed after the fourth day post-infusion. However, at days 8 and 11 after infusion, alpha-4 integrin levels were back at the baseline levels. Consistent with these findings, NAB were below the detection limit at days 2 and 4, and reached high titre levels (> 1:100) again at day 11.
Serial alpha-4 integrin and sVCAM-1 levels were also examined in a natalizumab-treated MS patient without NAB, showing the expected sustained decreases in alpha-4 integrin levels on PBMC (Figure 1B) and in serum sVCAM-1 levels (Figure 1D) between two consecutive infusions. In contrast, serial determination of alpha-4 integrin and sVCAM-1 levels from a healthy control showed only slight fluctuations (Figure 1B, 1D).
Discussion
Introduction of natalizumab in MS treatment raised new hope due to its impressive effectiveness in reducing relapse rate and disability progression. Unfortunately, about 6% of natalizumab-treated patients develop persistent NAB, associated with less efficacy and a higher risk of adverse events. 4 Usually, natalizumab therapy is stopped in patients with persistent NAB. With the introduction of fingolimod, it is now possible to offer patients with persistent NAB an additional effective treatment option.
The aim of our study was to investigate whether natalizumab has any effect on immune cells despite the presence of NAB. The interaction between natalizumab and anti-natalizumab NAB was determined by analysing surface alpha-4 integrin levels and serum sVCAM-1. These two adhesion molecules represent a receptor–ligand pair with a major role in lymphocyte transmigration into the CNS. Blocking of the alpha-4 integrin subunit by natalizumab results in reduced surface detectability of alpha-4, as evidenced by several studies using flow cytometry5,9,10 and in decreased serum concentrations of sVCAM-1. 8 In our opinion, it is necessary to distinguish between therapeutically effective (‘alpha-4 binding’) natalizumab and therapeutically ineffective (‘NAB-neutralized’) natalizumab, and between ‘free’ NAB (ELISA-detectable NAB), and ‘natalizumab-aggregated’ NAB (ELISA-undetectable NAB). To elucidate natalizumab–NAB interactions, we serially investigated cell surface levels of alpha-4 integrin and serum concentrations of sVCAM-1 between two natalizumab infusions in a NAB-positive patient and observed transiently decreased alpha-4 and sVCAM-1 levels and a transient negativity of NAB.
Our data suggest that the standard 300 mg dose of freshly infused natalizumab changes the ratio between natalizumab and NAB in favour of therapeutically active natalizumab. Besides the widely accepted fact that NAB neutralize natalizumab, in our case it can also be seen the other way around. A probable explanation for these findings is that in the first days after a natalizumab infusion, free NAB aggregate with natalizumab and are functionally ‘neutralized’ and below the detection limit of ELISA, whereas excess of natalizumab allows therapeutic blocking of the alpha-4 integrin. However, this effect is transient and dose-dependent: after a few days the natalizumab effect could no longer be determined, as alpha-4 integrin and sVCAM-1 levels were back at baseline levels and high-titre NAB were detected again. In particularly, our findings are interesting regarding the dynamic shifts of serum sVCAM-1 levels, which concur with surface detectability of alpha-4 on immune cells. In a recent study it was shown that endothelial cells react to a natalizumab-induced shortage in alpha-4 levels by reduced shedding or down-regulation of VCAM-1. 8 Our results imply that endothelial cells are immediately responsive to alpha-4 availability, hence natalizumab therapy. Moreover, sVCAM-1 is not subject to neutralization by NAB, although it possibly shares a similar binding structure to alpha-4 like natalizumab.
The fact that ‘free’ NAB were not detectable for the first few days post-infusion implies that a second application shortly after the first could provide a longer-lasting blockade of alpha-4 integrin. It remains open to question whether individual patients with NAB might benefit either from divided and/or clustered natalizumab applications (e.g. days 1 and 2) or from higher infusion frequencies. However, a potential increase of adverse events such as allergic reactions and a potential increase of NAB titres, in particular of high-affinity NAB, might occur.
We must state here that our findings are limited by the number of patients, but we think that these data provide new insights into short-term molecular changes during natalizumab treatment in the presence of NAB. Above all, our data show that evaluation of alpha-4 integrin expression levels on mononuclear cells by flow cytometry can provide early information on presence of NAB and efficacy of natalizumab therapy.
Footnotes
Funding
This study was supported by an investigator initiated research grant of Biogen Idec Austria.
Conflict of interest statement
Dr. Kraus received personal compensation from Bayer, Biogen-Idec, Merck-Serono, Sanofi-Aventis, Novartis for consulting services and financial support for research activities from Bayer, Biogen-Idec, Genzyme, Merck-Serono, Novartis, Sanofi-Aventis.