
Abstract
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and neurodegenerative disease of the central nervous system (CNS) characterized by destruction of myelin sheaths and axonal loss. 1 In industrialized countries, MS is the most common cause of neurological disability in young adults. The clinical features of MS reflect the complex interaction of inflammation, demyelination and axonal degeneration. 2 It is becoming increasingly apparent that axonal and neuronal degeneration start in the early stages of MS3,4 and that the accumulating clinical disability characteristic of secondary progressive multiple sclerosis (SPMS) reflects progressive neurodegeneration. 2 The focus of attention has turned to novel neuroprotective therapeutic strategies and to the development of biomarkers of neurodegeneration. 5 Olfactory disturbances are one of the most common early manifestations of certain CNS neurodegenerative diseases, such as Parkinson’s disease, 6 Alzheimer’s disease7,8 and Lewy body disease. 9 A diminished sense of smell in MS has also been reported.10-16 There are indicators that olfactory dysfunction in MS is related to lesion load in the olfactory brain regions (i.e. inferior frontal and temporal lobe regions),12,14 disability,14,17 and symptoms of anxiety and depression.13,14 To our knowledge, the only study 16 that has explored the association between olfaction and MS disease course did not find significant results. However, the study used a relatively small sample size (n = 50). A clear association between clinical MS features and olfactory deficits is yet to be established.
Our study goals were: 1) to characterize the olfactory identification capacity in MS, using the Brief Smell Identification Test (B-SIT); and 2) to explore possible associations between smell identification impairments and patients’ clinical characteristics.
Subjects and methods
The study included 153 patients with MS (according to the McDonald Revised criteria 18 ) recruited consecutively from the Neuroimmunology Outpatient Clinic from Hospital de Santo Antonio - Centro Hospitalar do Porto, between May 2009 and July 2010. All patients were recruited during their regular follow-up visits. The exclusion criteria were current or recent (within the previous 30 days) MS exacerbation, other CNS disorder or serious medical illness that could interfere with mood or olfaction (e.g. structural or inflammatory disease of the nose or sinuses, previous head trauma).
The healthy control group (HC) included 165 individuals recruited in the community, without neurological or psychiatric disorders or other known conditions that could cause abnormal olfaction (e.g. structural or inflammatory disease of the ear–nose and sinuses or previous head trauma).
All subjects provided informed written consent to participate in this study, as required by the Declaration of Helsinki.
Neurological assessment
On the testing day, MS patients underwent a detailed neurological examination and the following data were collected from the clinical chart: age at onset, disease duration, disease course, and current medication. Patients were grouped according to their disease course into relapsing–remitting (RRMS), SPMS and primary progressive (PPMS). 19
A brief assessment of cognitive status was obtained with Mini-Mental State Examination (MMSE). 20 The Expanded Disability Status Scale (EDSS) 21 and Multiple Sclerosis Severity Scale (MSSS) 22 were used to measure, respectively, physical disability and disease severity. The neurological assessment was conducted by neurologists blinded to the olfactory and psychiatric test results.
Olfactory and psychiatric assessment
All participants were given a questionnaire to ascertain subjective olfactory difficulties and smoking habits, and were asked to answer the B-SIT (commercially distributed by Sensonics. Inc., Haddon Heights, USA) and the Hospital Anxiety and Depression Scale (HADS). 23 The assessment instruments were administered and the performances were supervised by psychologists blinded to the patients’ clinical characteristics. B-SIT is a self-administered ‘scratch and sniff’ test that incorporates 12 different items. 24 The English version of the B-SIT was translated into Portuguese and the kits were adapted to accommodate the translation. Each item contains a microcapsulated odour strip from which an odorant can be released by scratching its surface with a pencil. Examinees were asked to identify each item from a forced-choice list, with four alternatives. The test score ranged from 0–12 and corresponded to the total number of correct choices.
Statistical analyses
Statistical analyses were performed using the PASW® Statistics 18. T-test for independent samples, Mann–Whitney test, Chi-square and Fisher’s exact were used as appropriate for group comparisons. Logistic Regression was applied to study the influence of demographic and clinical variables on impaired odour identification (0 = impaired vs. 1 = not impaired). For logistic regression analysis, variables age (0 = < 54 vs. 1 = ≥ 55 years old) and disease course (0 = RRMS or PPMS; 1 = SPMS) were dichotomized. For all statistical analyses, the p-value was considered significant when p < 0.05. Odds ratios (OR) and their 95% confidence intervals (95% CI) for each factor were calculated while adjusting for other covariates. Receiver operator characteristic (ROC) curve was used to identify sensitivity and specificity percentages.
Results
Demographic and clinical characteristics
MS and HC groups were not significantly different in terms of gender, age, education, and smoking habits (Table 1). MS patients’ raw scores on the depression subscale (MS: mean = 6.04, SD = 4.15 vs. HC: mean = 4.13, SD = 3.19) were significantly higher (p < 0.001) than HC subjects.
Groups’ demographic and clinical characteristics.
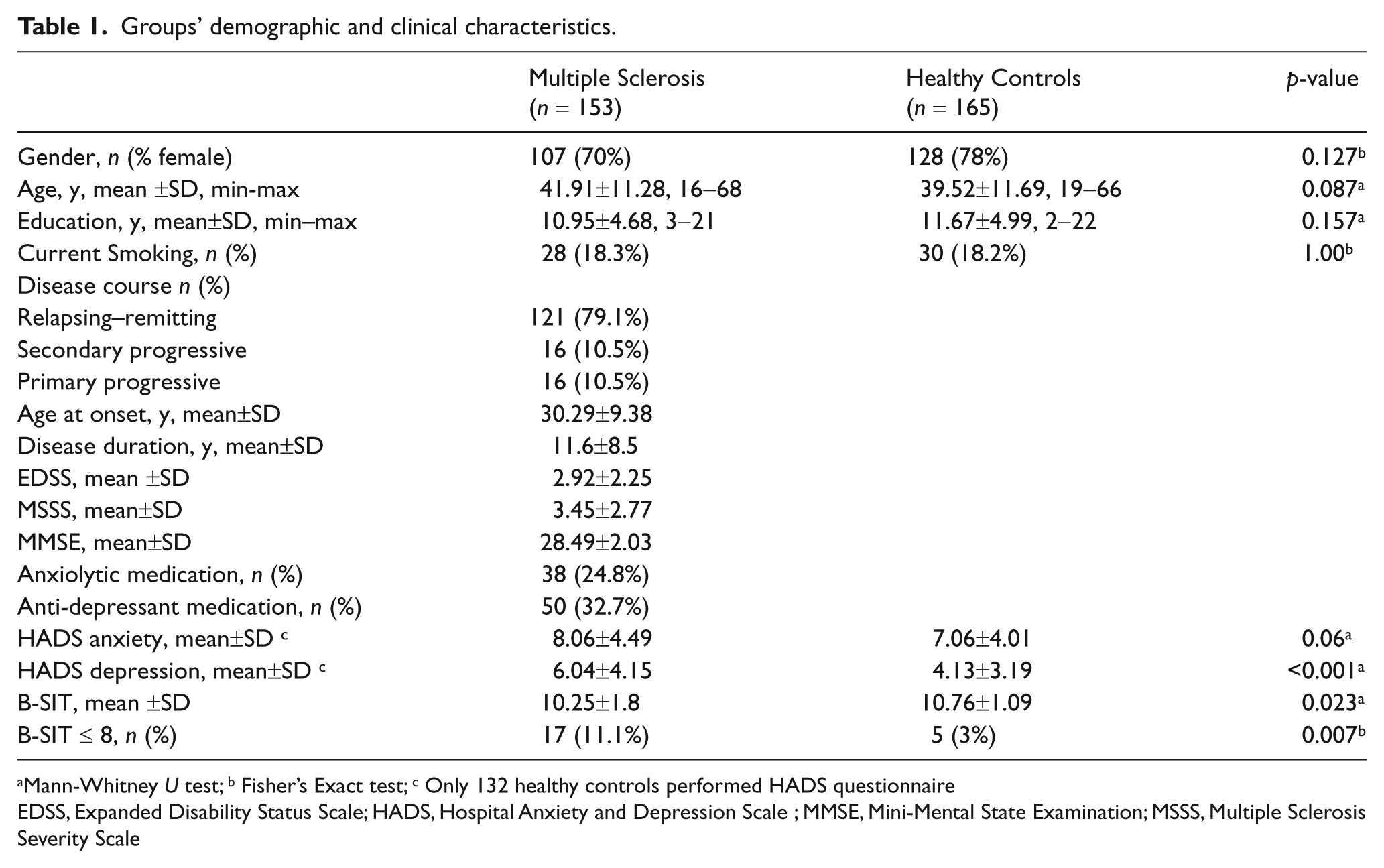
Mann-Whitney U test; b Fisher’s Exact test; c Only 132 healthy controls performed HADS questionnaire
EDSS, Expanded Disability Status Scale; HADS, Hospital Anxiety and Depression Scale ; MMSE, Mini-Mental State Examination; MSSS, Multiple Sclerosis Severity Scale
Olfactory assessment
The threshold B-SIT ≤ 8 was used to classify impaired smell identification. This cut-off corresponds to the second percentile (which is approximately 2 standard deviations below the mean) of the HC subjects. Overall, MS patients had significantly lower B-SIT score (p = 0.023) and higher frequency of impaired identification of common odours (p = 0.004) than HC subjects (Table 1). The comparison between MS subgroups with (n = 17; 11.1%) and without (n = 136; 88.9%) impaired odour identification revealed significant differences on the following variables: age (p < 0.001), disease duration (p = 0.004), education (p = 0.001), EDSS (p < 0.001), HADS depression (p = 0.002), and MMSE (p < 0.001). No significant differences were found concerning gender, smoking habits, current intake of anxiolytics or anti-depressants, and HADS anxiety scores (Table 2). Five HC subjects (3%) had impaired performance on the B-SIT. No significant differences were found between HC subjects with and without impairment, regarding gender, age, education, smoking habits, HADS anxiety and depression scores, and MMSE.
Odour identification impairment in multiple sclerosis.
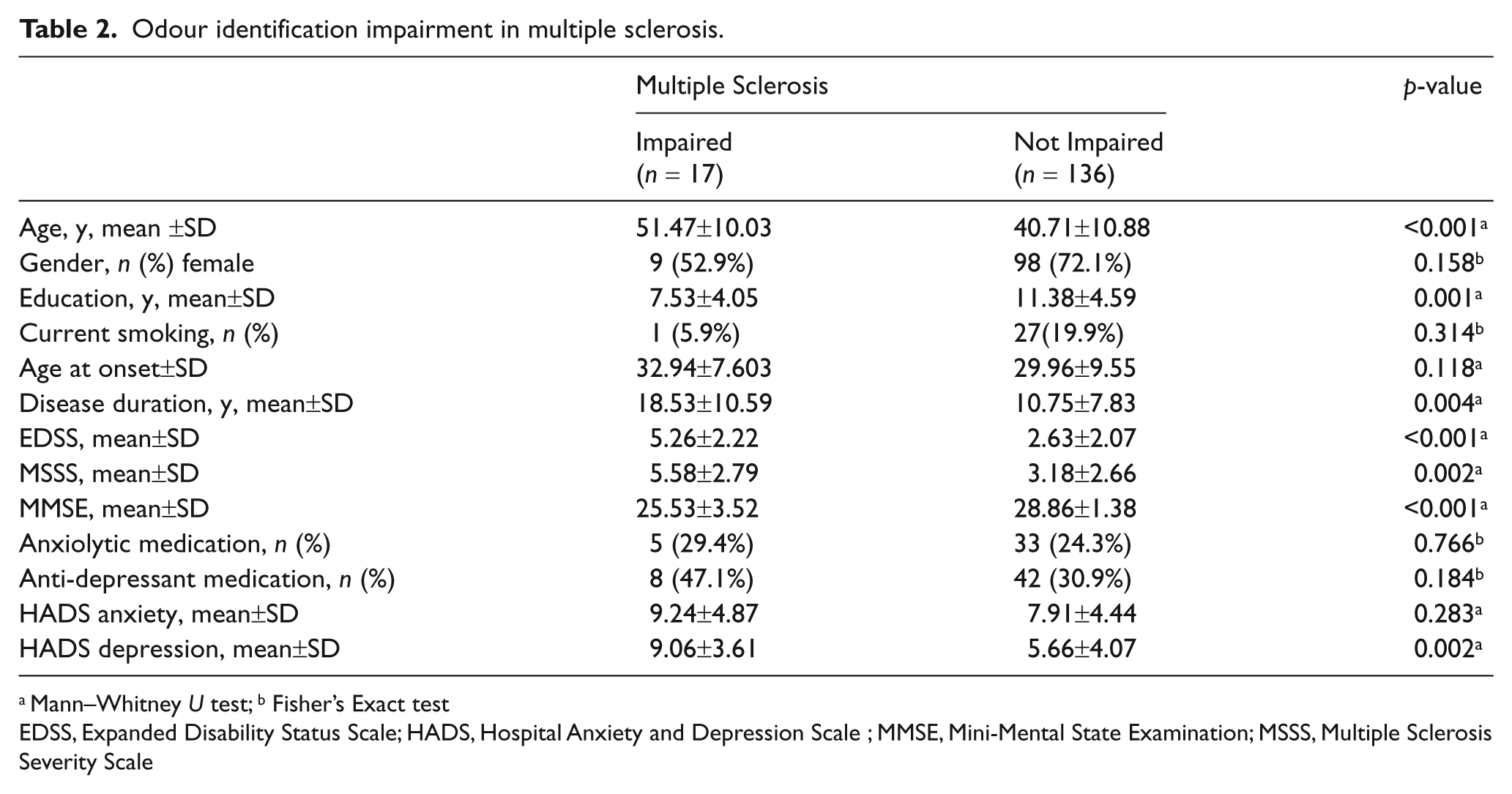
Mann–Whitney U test; b Fisher’s Exact test
EDSS, Expanded Disability Status Scale; HADS, Hospital Anxiety and Depression Scale ; MMSE, Mini-Mental State Examination; MSSS, Multiple Sclerosis Severity Scale
Odour identification impairment and disease course
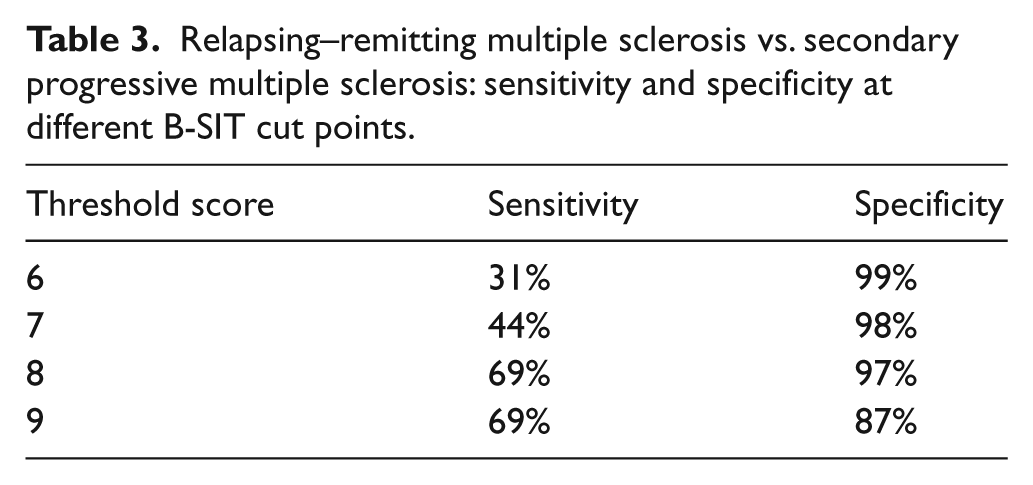
Concerning disease course, the frequency of odour identification impairment was significantly higher (p < 0.001) for MS patients with SPMS (11/16; 68.8%) than RRMS (4/121; 3.3%) or PPMS (2/16; 12.5%) courses. In comparison with the HC group, the frequency of impairment was significantly higher for SPMS patients (p < 0.001), but not for RRMS (p = 0.999) or PPMS (p = 0.119) patients. A threshold score of ≤ 8 on the B-SIT provided a sensitivity of 69% and a specificity of 97% (ROC area under the curve 0.812, 95%CI = 0.668–0.956) in the identification of SPMS among patients with relapsing onset. Sensitivity and specificity of other threshold cut-off points are presented in Table 3.
Relapsing–remitting multiple sclerosis vs. secondary progressive multiple sclerosis: sensitivity and specificity at different B-SIT cut points.
Due to strong collinearity between disease duration, EDSS and MSSS, two logistic regression models were analysed (Table 4). The first included the following independent variables: age, education, disease duration, EDSS, disease course, HADS depression, and MMSE. The second included age, education, MSSS, disease course, HADS depression, and MMSE. When a backward elimination procedure was applied to each model, the variables that remained significantly associated with odour identification impairment were the same, i.e. age (OR = 0.191, 95%CI = 0.042–0.865), disease course (OR = 0.043, 95%CI = 0.009–0.202), and MMSE (OR = 1.615, 95%CI = 1.128–2.312). In other words, higher age, SPMS course, and lower MMSE score were significantly and independently associated with impaired performance on the B-SIT.
Multivariate logistic regression analyses.
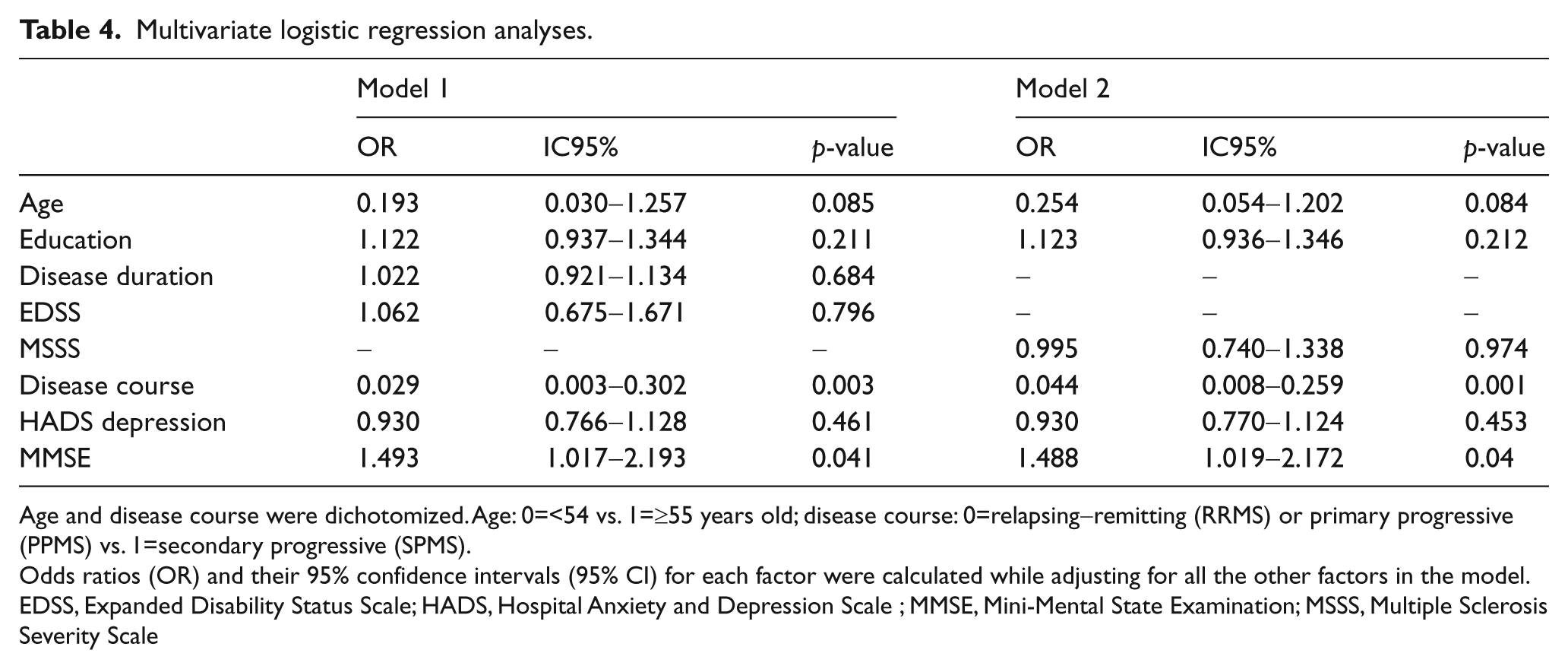
Age and disease course were dichotomized. Age: 0=<54 vs. 1=≥55 years old; disease course: 0=relapsing-remitting (RRMS) or primary progressive (PPMS) vs. 1=secondary progressive (SPMS).
Odds ratios (OR) and their 95% confidence intervals (95% CI) for each factor were calculated while adjusting for all the other factors in the model.
EDSS, Expanded Disability Status Scale; HADS, Hospital Anxiety and Depression Scale ; MMSE, Mini-Mental State Examination; MSSS, Multiple Sclerosis Severity Scale
Discussion
Olfactory deficits were found in 68.8% of patients with SPMS course. The association between impaired identification of common odours and SPMS course was not dependent on other clinical (disease duration, disability, and severity), demographic (age, education), psychopathological or cognitive features. The prevalence of impairment on the B-SIT was similar (~3%) between patients with RRMS and HC participants. Even though patients with PPMS were more impaired on the B-SIT (12.5%), the results were not statistically significant.
The pathological mechanisms underlying smell identification impairments in MS patients with SPMS course are unknown. Based on the neuropathological differences among MS subtypes,25,26 it is reasonable to think that more olfactory deficits in SPMS patients may reflect the combination of high density of demyelinated plaques and widespread neurodegeneration. Neuroimaging studies have provided evidence of a negative correlation between odour identification performance and extension of MS-related plaques in the frontal and temporal regions.12,14 So, it is plausible to speculate that additional neuroimaging examination would have revealed that olfactory deficits in SPMS are mediated by higher lesion load and more pronounced brain atrophy.
In our MS cohort, the frequency of smell identification impairment was detected in 11.1% of MS patients. This prevalence of impairment was somewhat lower than other studies with smaller sample sizes and/or with other olfactory assessment tests.11,12,15,16 Relative to other olfactory assessment tests (e.g. University of Pennsylvania Smell Identification Test), the B-SIT is less sensitive in detecting subtle alterations in smell function, 24 which may partly explain the relatively low frequency of deficit detected in the current study. Discrepancies in prevalence reports may also reflect different olfactory capacities observed in MS remission and exacerbation phases. 27 A relapse within the previous 30 days was used as exclusion criterion. Other reports13,14 of MS patients with 1–75 months since the last exacerbation have found an olfactory deficit prevalence of 12.5%. Studies that have not stated exclusion criteria based on current or recent relapses11,12,15 or have explicitly mixed patients in remission and exacerbation phases 16 have found higher frequency of deficit (15–50%).
Consistent with previous findings11-14,16 the prevalence of olfactory impairment in MS was higher than in the normal population. Hyposmia in MS was found to be related with more depression symptoms, longer disease duration, higher disability index, and faster disease progression index. These results corroborate previous published studies.11,13,14,16,17
The B-SIT does not measure odour detection threshold or discrimination abilities and may not be sensitive to detect mild odour identification deficits in young patient populations. Therefore, a more comprehensive and detailed assessment of olfactory functions may have revealed a higher prevalence of impairment.
MS patients’ odour identification impairment was also significantly associated with higher age, lower education, and lower MMSE scores. Smell identification tests are known to be cognitively more demanding than other olfactory tests. 28 It is reasonable to speculate that a lower level of functioning in other cognitive areas had a negative effect on the performance of B-SIT. The association between decreased olfactory functioning and higher age has been well documented in normative studies. 29 However, it has seldom been explored or accounted for in MS patients.
The B-SIT provided good discrimination between patients with RRMS and SPMS course. The high specificity (97%) attained by B-SIT is promising as a useful tool in everyday treatment decisions and patient selection for clinical trials. However, due to the retrospective nature of this study, it is not possible to use B-SIT to identify RRMS patients who will develop a SPMS course. The clear association between SPMS course and odour identification impairment lends evidence to the current idea that neurodegeneration contributes significantly to SPMS. This finding may have important implications in the future development of clinical markers capable of confirming and even predicting disease progression in patients with relapsing-onset MS. It could also be used in future to monitor the disease and its response to treatments, namely neuroprotective medications. Future research should investigate other complementary objective and sensitive measurements (e.g. olfactory evoked potentials) to follow-up prospectively early RRMS patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that they do not have any conflicts of interest.