
Abstract
Background:
Factors determining severity and recovery of early demyelinating events in pediatric multiple sclerosis (MS) patients are unknown.
Objective:
The objective of this study was to characterize the severity and recovery of early demyelinating events in pediatric MS.
Methods:
Multivariate logistic regression was performed to determine predictors of severe (versus mild/moderate) relapses and poor or fair (versus complete) recovery in patients aged 18 years or less with MS or clinically isolated syndrome (CIS).
Results:
Optic nerve involvement (OR 4.30, 95% CI 1.50–12.3, p = 0.007) was associated with a severe initial demyelinating event (IDE), while non-White race (OR 2.55, 95% CI 0.87–7.49, p = 0.088), localization to the cerebral hemispheres (OR 7.94, 95% CI 0.86–73.8, p = 0.068), or encephalopathy (OR 8.70, 95% CI 0.86–88.0, p = 0.067) showed a trend towards increased IDE severity. A similar association with race was found for severe second events. A severe IDE (OR 6.90, 95% CI 2.47–19.3, p < 0.001) was associated with incomplete IDE recovery, with similar trends for second and third events. Incomplete recovery from the first event predicted incomplete second event recovery (OR 3.36, 95% CI 0.98–11.6, p = 0.055).
Conclusions:
These results may help identify children at risk for a more aggressive disease course.
Introduction
While only a small percentage of individuals with multiple sclerosis (MS) have their initial demyelinating event (IDE) during childhood, 1 –4 these patients reach disability at a younger age because of earlier disease onset. 1 Although time to disability might be slower in White, non-Hispanic cohorts, 1 several findings in ethnically and racially diverse cohorts question the milder disease course in children. A substantial proportion of pediatric MS patients in a racially and ethnically diverse cohort developed some clinical disability in a relatively short mean follow-up period. 5 Furthermore, children may have a greater white matter lesion burden and brainstem and cerebellar involvement at MS presentation compared with adults, 6 both of which have been shown in adults to be associated with worse prognosis. 7,8
While factors affecting severity and recovery of early MS events in adults have recently been characterized, it is unknown what influences these processes in pediatric MS. 9 In adults, younger age, non-White race, and severe prior events predict event severity, while poor recovery is predicted by a severe concurrent event or poor recovery from a prior event. 9 The goal of our study was to characterize predictors of severity and recovery in the initial, second, and third demyelinating events in an ethnically and racially diverse cohort of patients with pediatric-onset MS. A better understanding of which patients are at the greatest risk for more severe attacks or poor attack recovery may help clinicians and families determine which children may benefit from closer follow-up or for early initiation of disease-modifying therapies approved for adult MS.
Methods
Patients
The UCSF Committee on Human Research approved this project. Data from 105 consecutive patients diagnosed with MS or clinically isolated syndrome (CIS), according to operational criteria, 10 were analyzed in this retrospective cohort study. Patients were evaluated at the UCSF Pediatric MS Center, which opened in 2006 and is one of six regional pediatric MS centers of excellence sponsored by the National Multiple Sclerosis Society. Patients with neuromyelitis optica (NMO) or acute disseminated encephalomyelitis (ADEM) or who had disease onset at 18 years or older were excluded.
Definition of outcomes
A demyelinating event, or relapse, was defined as symptoms referable to the central nervous system, lasting for at least 24 hours, in the absence of fever or concurrent illness, and occurring at least 30 days after a prior event. Pseudoexacerbations were excluded. Severity was scored as mild to moderate, or severe, based on prior definitions. 9 An event was considered mild if the Functional System Scores (FSS) were 0 to 1 in one to three FSS, visual acuity better than 20/40, or Expanded Disability Severity Score (EDSS) 0 to 1.5; moderate if the FSS were 2 in one or two FSS, or if there was a score of 1 in four or more FSS, visual acuity 20/40–20/190, or EDSS 2.0–2.5; or severe if scores exceeded those for moderate severity. Recovery was considered complete if all FSS had scores of 0 with EDSS of 0. Fair recovery required lingering subjective neurological deficit with score of 1 in at least one FSS, visual acuity 20/40 or better, and EDSS 1.0–1.5. Poor recovery involved a score of 2 in at least one FSS, visual acuity 20/50 or worse, and EDSS 2.0 or greater. For second and third exacerbations, if recovery from the prior episode was incomplete, severity was scored as mild if EDSS increased by 0.5 or FSS score increased by 1 in one to three FSS; moderate if EDSS increased 1–2 points or FSS of 2 in one or two FSS; and severe if EDSS or FSS criteria were greater than moderate. Likewise, recovery from a second or third attack was defined as complete if no residual symptoms or deficits remained compared with before the event; fair if EDSS increased up to 1 point or if FSS scores increased by 1 point in one or two systems; and poor if worse than the fair criteria. For recovery, we also explored models in which steroids had been given to determine whether it altered the associations between the other variables and recovery. We did not do so for severity, since severity likely determined in part whether steroids were given, which would lead to reverse causality.
Other definitions
Predictors that were considered include gender, self-reported race (White, non-White, and mixed) and ethnicity (Hispanic, non-Hispanic, and mixed), age at onset of MS, and insurance status (insured versus California Children’s Services[CCS]/MediCal/none). For the purposes of this study, non-White race means at least one out of four grandparents is non-White, and Hispanic ethnicity means at least one out of four grandparents is Hispanic. CCS is a part of the California Department of Health Services that covers children with certain medical conditions whose families have an income under US$40,000 per year or whose medical expenses account for more than 20% of a family’s gross income. Clinical variables analyzed included anatomical localization, treatment with disease-modifying therapy, severity, and recovery. Treatment was defined as any course of disease-modifying therapy lasting at least 90 consecutive days prior to the second or third demyelinating event.
Statistics
Data were analyzed using a multivariate logistic regression model, incorporating the predictors described above. Event severity was condensed into one of two categories, severe or mild-to-moderate, whereas event recovery was condensed into either complete or fair-to-poor. Encephalopathy was not included as a predictor in the second and third event recovery models, as the number of these exacerbations involving encephalopathy was too small. Multivariate analysis included all predictors with p < 0.2 in the univariate analysis. Data for first and second events were also analyzed with a Bayesian Information Criterion (BIC) 11 minimization model, which was used to identify the model with the best fit. All statistical analysis was performed with STATA 10.0 software (StataCorp, College Station, TX).
Results
Patient characteristics
We identified 105 patients with MS or CIS onset prior to 18 years of age. Patient characteristics are shown in Table 1. Data on race was not available for three patients, and ethnicity was not available for one patient.
Patient characteristics.
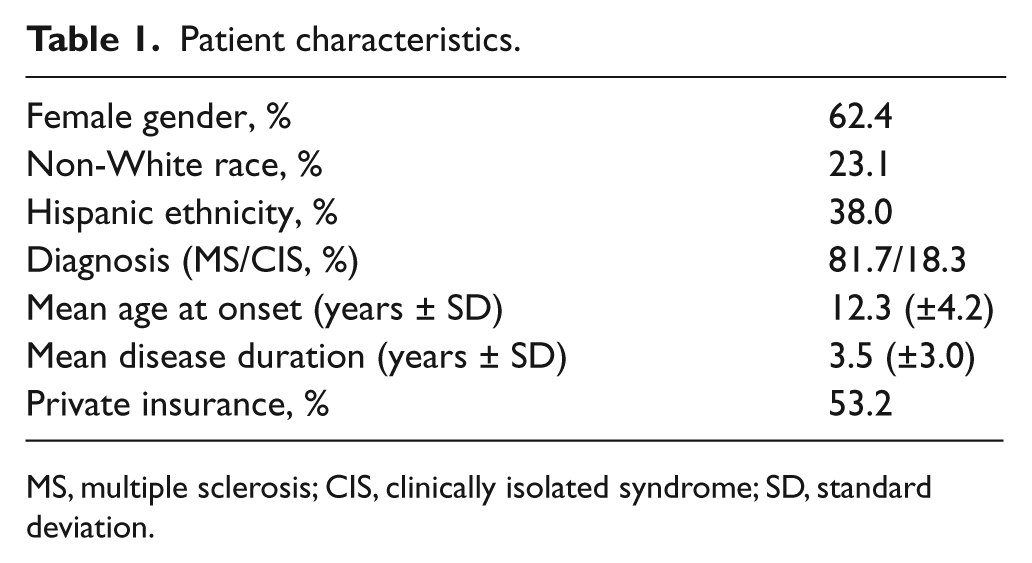
MS, multiple sclerosis; CIS, clinically isolated syndrome; SD, standard deviation.
Characteristics of first, second, and third demyelinating events
Characteristics for first (n = 109), second (n = 82), and third (n = 54) events are shown in Table 2.
Characteristics of first, second, and third demyelinating events.
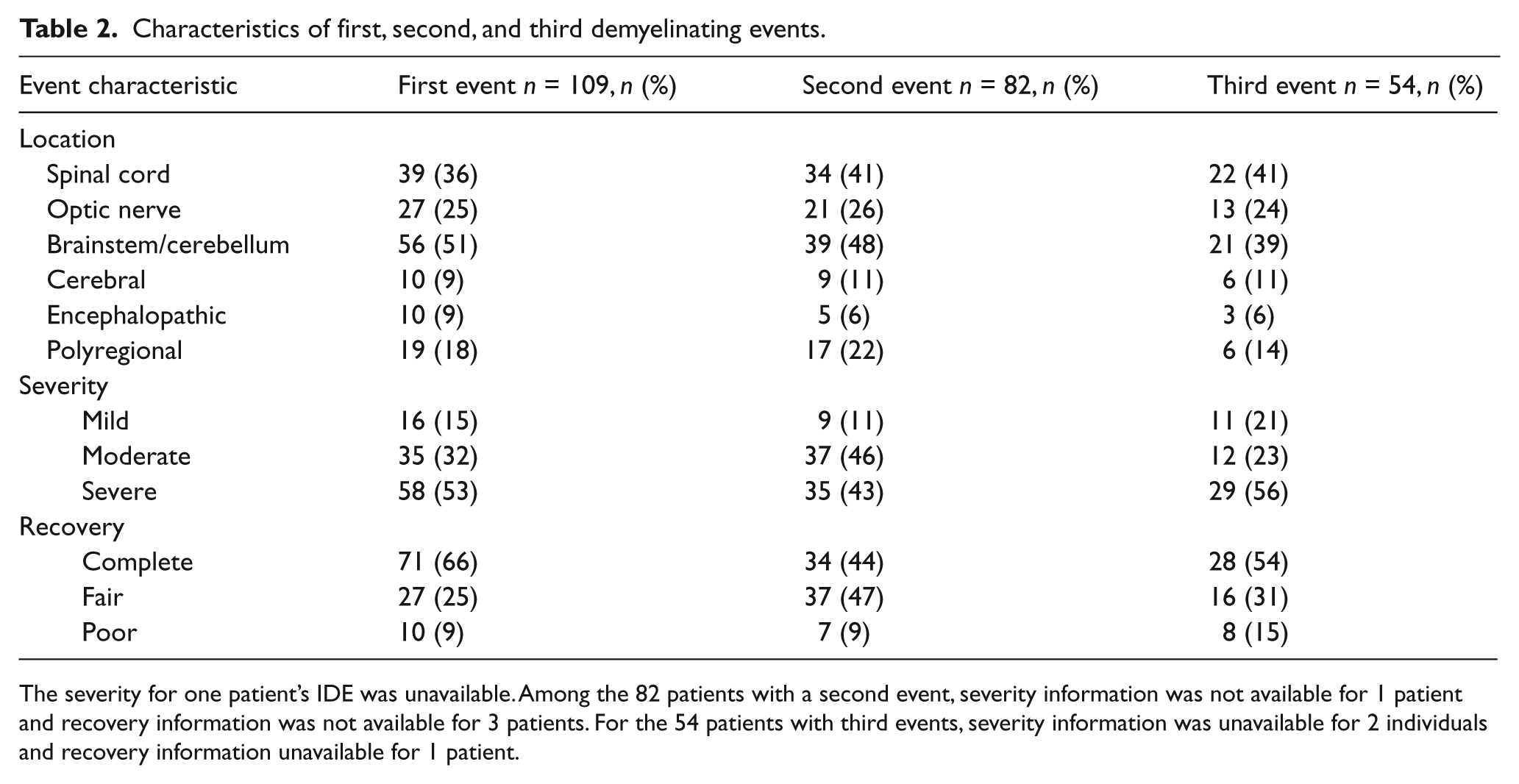
The severity for one patient’s IDE was unavailable. Among the 82 patients with a second event, severity information was not available for 1 patient and recovery information was not available for 3 patients. For the 54 patients with third events, severity information was unavailable for 2 individuals and recovery information unavailable for 1 patient.
Predictors of severe first, second, and third events
The results of the multivariate analyses for predictors of more severe first (a), second (b) and third (c) exacerbations are shown in Table 3. The model for second event severity did not include IDE severity as a predictor, as it did not have p < 0.2 in the univariate analysis. Non-White race was associated with greater risk of a severe first or second event. Localization within the optic nerve or cerebral hemispheres, or encephalopathy, was associated with more severe first events. Multivariate analysis with BIC minimization was largely consistent with analysis based on univariate predictors with p < 0.2 (Supplementary Tables).
Multivariate predictors of: (a) severe initial demyelinating events; (b) severe second events; (c) severe third events. Univariate analysis.
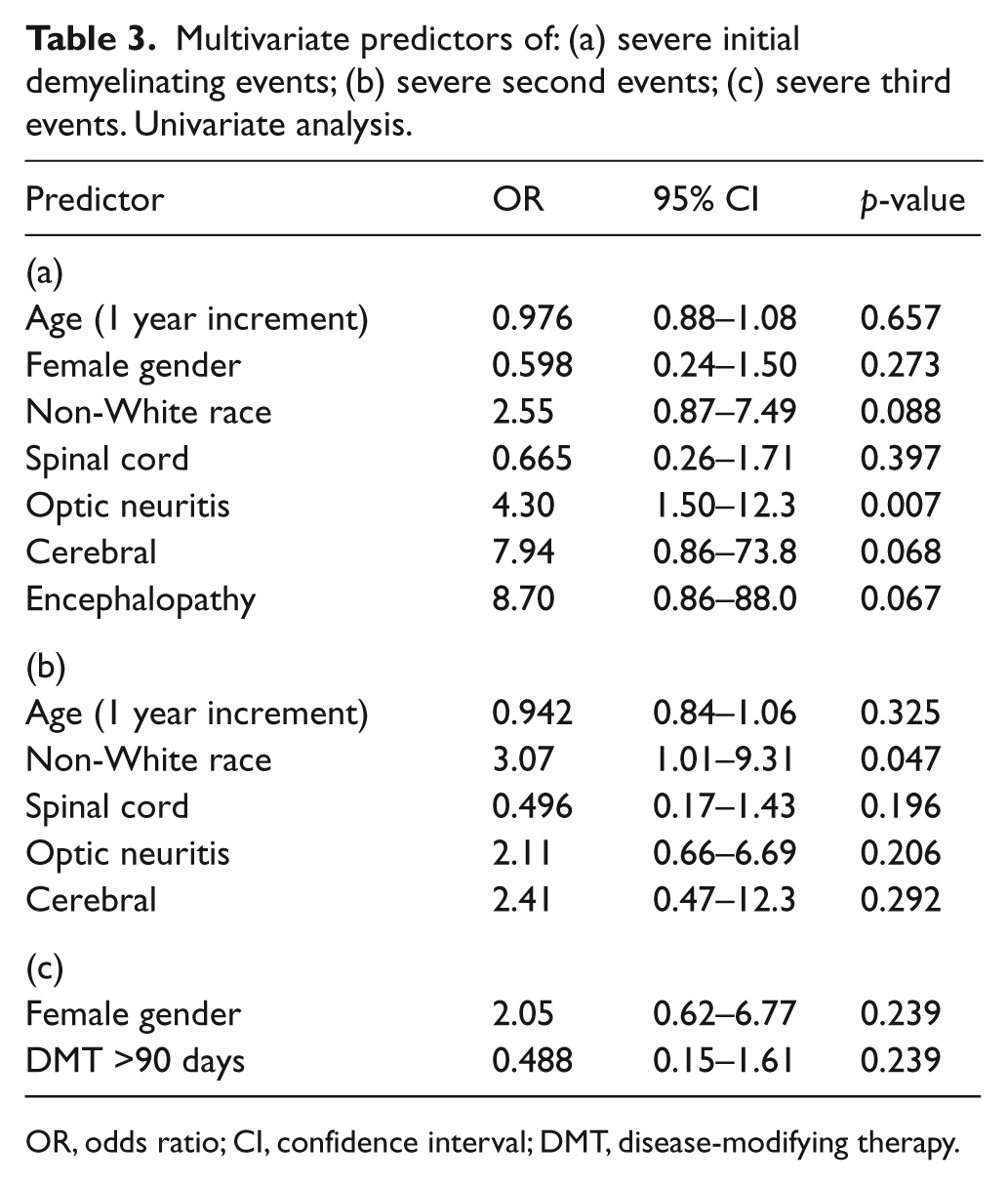
OR, odds ratio; CI, confidence interval; DMT, disease-modifying therapy.
Predictors of incomplete event recovery
Multivariate analysis of predictors of worse recovery for first (a), second (b), and third events (c), as identified by univariate screening, are presented in Table 4. Results of analysis using BIC minimization were consistent with the univariate analysis (Supplementary Tables). Severe events predicted incomplete recovery, and prior incomplete recovery predicted incomplete recovery from subsequent events. There was no meaningful change if steroid use was added to the model.
Multivariate predictors of (a) incomplete initial demyelinating event recovery; (b) incomplete second event recovery; (c) incomplete third event recovery. Univariate analysis.
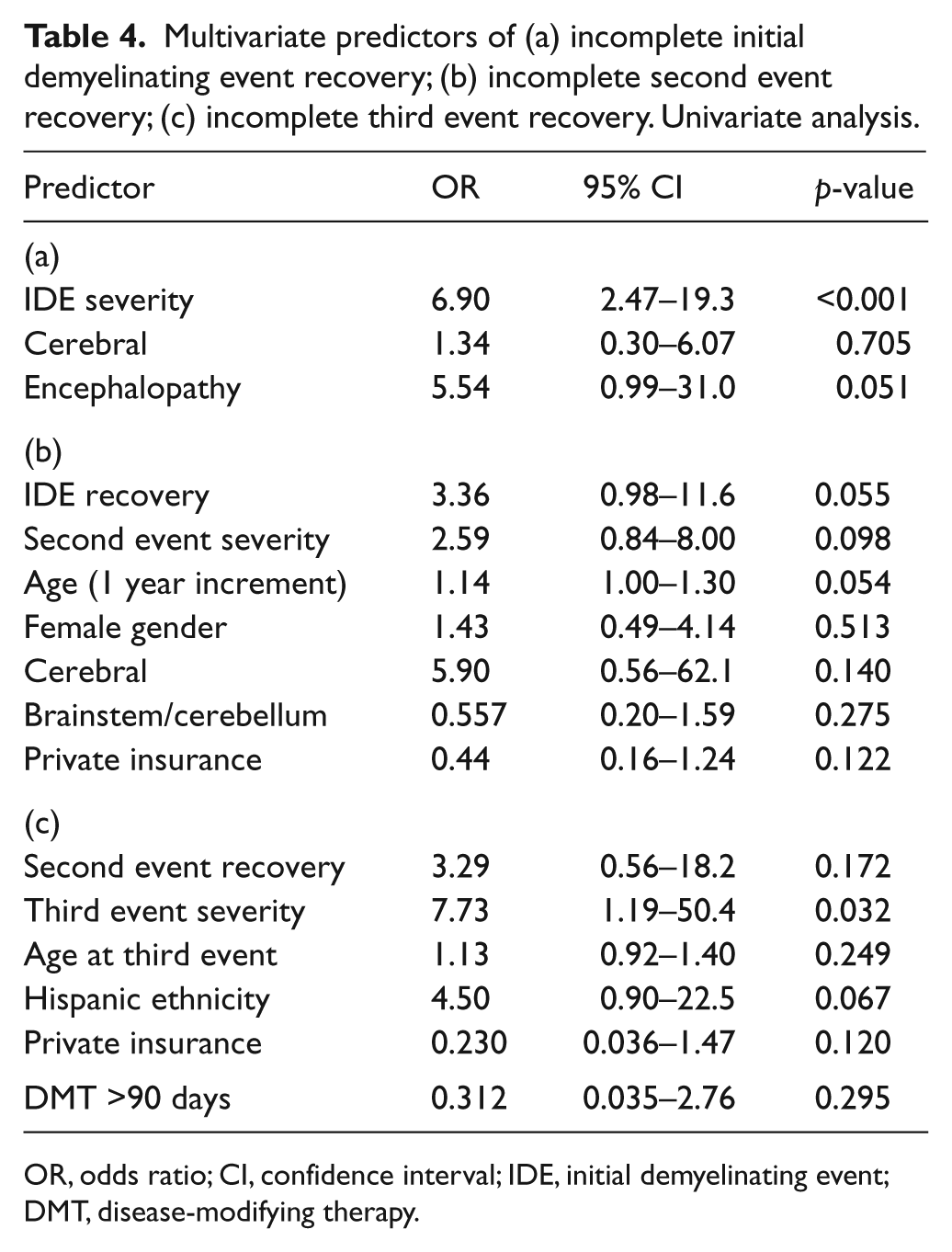
OR, odds ratio; CI, confidence interval; IDE, initial demyelinating event; DMT, disease-modifying therapy.
Discussion
Our findings revealed a number of similarities when compared with an adult study 9 of severity and recovery of early MS events. In particular, non-White race was associated with more severe initial demyelinating events, as was cerebral hemispheric localization. In our pediatric cohort, a severe demyelinating event predicted poor recovery, as in adults. These results indicate that there is some consistency across the age range of MS presentation, and that pediatric MS is likely on a continuum with adult-onset MS, rather than a distinct pathological entity.
There was a notable difference, however, in anatomical location of the events among the pediatric patients compared with the adult cohort. Unlike what was reported in adults, optic nerve involvement was associated with severity in children. Compared with the adult cohort, 9 the optic nerve may be more likely to be involved in children compared with adults after the IDE. It is also possible that various CNS regions have age-dependent immunogenicity 12,13 or accessibility of immune cells that could account for differential localizations and severities in adults versus children. For example, children have a higher proportion of events in the brainstem/cerebellum and cerebral hemispheres than do adults, and encephalopathy is exceedingly rare among adults.
Our data also indicate that children and adults may have differing intrinsic severity and recovery to their MS exacerbations. A prior study at UCSF in adults 9 found that 10–17% of attacks were severe among adults, compared with 43–56% of events in this study using the same scoring system. First, this is in line with our observation both in adult and pediatric MS that younger patients experience more severe early exacerbations. Second, this difference might be due, in part, to the greater proportion of non-White patients in the pediatric cohort. Greater event severity among children could also be due to more aggressive immune activation in children compared with adults, or perhaps to different levels of immune cells or cytokines in the brains of children. 14 However, we cannot exclude a referral bias, as the UCSF Regional Pediatric MS Center is the only such center in the Western United States, and may see patients with a more aggressive disease course.
Although children in our cohort experienced more frequent severe events, recovery from initial demyelinating events was complete in 66% of pediatric patients, compared to 46% of adult patients in the same prior study, 9 suggesting less irreversible injury or a greater repair potential in children. This finding is consistent with studies in animal models of CNS demyelination demonstrating that capacity for remyelination declines with age. This age-dependent remyelination is most likely related to impaired differentiation of precursor cells to myelin-producing oligodendrocytes with aging and poorer clearance of myelin debris by phagocytic macrophages in older animals. 15 –17 Recovery from third events also appears to be more complete in our pediatric patients compared with the adult cohort. The more complete recovery in pediatric patients may also be related to lesion edema, 18 which is a feature of the large, tumefactive lesions more common in children than adults, 6 rather than true demyelination. In addition, less irreversible neuronal damage may happen in MS lesions in children. In addition to the age-dependent capacity for more complete recovery, the degree of recovery from first and second demyelinating events tends to be consistent with the extent of recovery from subsequent events.
Limitations of the study are related to both the small sample size and study design. Although it was a moderately-sized cohort, given the rarity of pediatric-onset MS, the size may still have obstructed our ability to detect meaningful associations, especially for the second and third events. The retrospective study design may limit accuracy of scoring early MS events that occurred long before patients’ first evaluation at our center. The outcome measures of the study include severity and recovery scales, which rely on neurological examination done at the time of and after an MS event and thus are prone to inter-rater discrepancies. We would expect, though, that this would have biased the findings toward the null hypothesis. Our patient recruitment was not population-based, and thus our cohort might have been biased toward higher disease severity. This, however, would not have been expected to alter the direction of the associations described in our work. Finally, the short length of follow-up may have also over-represented those patients with more aggressive disease in our study, as not all patients had second and third events by the time of data analysis.
In summary, although pediatric-onset MS patients appeared to have more severe demyelinating events compared with adults, they also generally seemed to have more complete recovery than adults. Furthermore, the extent of recovery from early events predicts recovery from subsequent events. Our findings add a racially and ethnically diverse group of patients to the growing pediatric-onset MS literature and will be of value to clinicians treating such patients and to scientists who are attempting to unravel the age dependence of demyelination, remyelination and repair in MS.
Footnotes
Acknowledgements
We are grateful to Janace Hart, our wonderful clinic coordinator, for her relentless support of our pediatric MS clinic.
Funding
This work was supported by the National Multiple Sclerosis Society. Dr Mowry’s research is funded by the National MS Society (Sylvia Lawry Fellowship Award) and NIH (grant number NIHK23NS067055). Dr Waubant’s research is funded by the National MS Society and the Nancy Davis Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.