
Abstract
Objective:
The aim of this study is to report the clinical profile and outcome of longitudinally extensive transverse myelitis (LETM).
Methods:
We prospectively studied adult patients who presented with LETM from January 2008 to December 2011. Information on demographic, clinical course, magnetic resonance imaging (MRI) and outcome was collected. HLA-DRB1 genotype was compared with those of 225 normal controls and patients with MS (228) and neuromyelitis optica (NMO) (22).
Results:
In total, 23 patients (16 female) with a median age of 44.5 years (range: 20–77 years) were included. Most (74%) had moderate–severe disability at nadir (48% non-ambulatory), normal/non-multiple sclerosis (MS) brain MRI (96%) and a median MRI cord lesion of 5 vertebral segments (range: 3–19). Laboratory analysis showed cerebrospinal fluid pleocytosis (45%), NMO-IgG (9%), antinuclear antibodies (70%), and genotype HLA-DRB1*13 (57%). The frequency of DRB1*13 genotype was higher compared with controls (p=0.002), MS (p=0.001) and NMO (p= 0.003) patients. After a median follow-up of 32 months, one patient converted to MS, two had relapsing LETM with NMO-IgG, and 20 remained as idiopathic with recurrences in four (20%). Twelve (52%) patients recovered with minimal disability (Expanded Disability Status Scale (EDSS)
Conclusions:
Inflammatory LETM is mostly idiopathic with a good outcome. It includes a relatively homogenous group of patients with an overrepresentation of the HLA-DRB1*13 genotype. EDSS at nadir is a predictor of the final outcome and extension of the myelitis of the recurrence risk.
Introduction
Transverse myelitis (TM) refers to an inflammatory lesion of the spinal cord that usually is not transverse in radiological or pathological studies. TM is classified as post-infectious, due to systemic connective tissue disease, as part of multiple sclerosis (MS) or neuromyelitis optica (NMO), or ‘idiopathic’. 1,2 Evidence-based guidelines on the management of TM have been recently published. 3 Except for NMO-IgG antibodies which were useful to determine the cause and the risk of TM recurrence, no other clinical, epidemiological or radiological factors reached similar or higher levels of recommendation for the diagnosis or prognosis of TM. 3
The term longitudinal extensive transverse myelitis (LETM) refers to a lesion that extends at least three vertebral segments. LETM has not been recognized as a particular type of idiopathic TM until recently. Patients with LETM may represent a particular subgroup of TM different from those with shorter lesions who have a high risk of evolution towards MS. 1 –3 Prospective series of LETM which could provide new insights regarding this entity have been limited to one study that suggested that LETM was an initial or limited form of NMO in a high percentage of patients. 4
In this prospective study we analyzed the clinical, radiological, immunological and genetic characteristics of a series of patients with inflammatory LETM. We focused on clinical and laboratory features that could be useful for diagnosis or prognosis.
Methods
Case selection and data collection
From January 2008 to December 2011, adult patients who presented with isolated LETM, as first episode or as recurrence of a remote isolated LETM event, were included in the study. Patients met the following criteria: presentation of symptoms and signs of spinal cord involvement and no evidence of symptoms and signs attributable to extra spinal involvement; progression to nadir within 21 days after the onset of the symptoms; spinal cord magnetic resonance imaging (MRI) lesion extending at least three contiguous vertebral segments; and appropriate studies to reasonably exclude diagnoses of compressive, vascular, infectious, metabolic, paraneoplastic or radiation myelopathy. The study protocol, which included a specific questionnaire and provided recommendations on how to perform the brain and spinal cord MRI, was disseminated through the MS study group of the Spanish Society of Neurology and the Spanish Network of MS (Red Española de Esclerosis Multiple).
The questionnaire included demographic items, associated diseases, description of the acute illness (characteristics of the motor/sensory symptoms, spinal sensory level, bladder dysfunction), laboratory data (cerebrospinal fluid (CSF) white blood cell counts and oligoclonal IgG bands, standard PCR and serological studies), description of the brain and spinal cord MRI, treatment at relapse, and type of chronic therapy if applicable. The type of therapy was not included in the protocol and the therapeutic decision was based on the judgment of the neurologists. The centralized laboratory analysis included antinuclear antibody (ANA), ds-DNA, anti-Ro and anti-La antibodies. HLA-DRB1 genotype, onconeuronal antibodies (Hu, Yo, Ri, CV2, Ma2, amphiphysin, Tr) and antibodies against neuronal surface antigens (NMDAR, GABABR, AMPAR, LGI1, Caspr2) were analyzed as previously described. 5,6 NMO-IgG were evaluated by immunohistochemistry and confirmed by a commercial cell-based assay (Euroimmun, Germany). 7 A neuroradiologist (AR) with more than 20 years of experience read all the MRI scans without knowledge of the clinical data.
Assessment of function
Ambulatory ability was assessed using the modified Hughes Functional Disability Scale (HFDS; 0=normal, 1=minor symptoms, 2=able to walk more than 30 ft without assistance, 3=able to walk more than 30 ft with assistance, 4=bed bound/wheelchair bound, 5=requires assisted ventilation, 6=death), 8 and measured on the Expanded Disability Status Scale (EDSS). All patients were followed for a minimum of 3 months.
Standard protocol approvals, registrations, and patient consents
The study was approved by the Ethic Committee of the Hospital Clinic, and written informed consent was obtained. Samples were deposited in the collection of biological samples named ‘neuroinmunologia’ registered in the Biobank of Institut d’Investigació Biomèdica August Pi i Sunyer (IDIBAPS), Barcelona, Spain.
Statistical analysis
Comparisons between categorical and continuous variables were performed using chi-squared test or Fisher’s exact test, and Wilcoxon’s rank test respectively. The Kruskal–Wallis test was used for multiple comparisons in case of continuous variables. Functional outcome was evaluated using the definition of recovery at 3 months from the initial event, and by the EDSS score at last follow-up. Good outcome was defined as minimal disability (EDSS score <3.0) at the last visit. The analysis of prognostic factors was done by logistic regression model to asses the adjusted association. Kaplan–Meier analysis and Cox regression was used to estimate cumulative survival probabilities and the effect of covariables on the time to recurrence. Variables included in both analyses were: age at onset, EDSS at onset, vertebral segments affected, sphincter impairment, localization and gadolinium enhancement of the spinal cord lesion, NMO-IgG status, ANA seropositivity, recurrent myelitis status and therapy. All statistical analyses were performed by SPSS 18.0 version. Significant p-values were set at 0.05 level.
HLA-DRB1 genotypic frequency was compared with that of 225 normal healthy controls, 228 definite MS patients according to the McDonald criteria 9 and 22 patients who fulfilled the criteria for the diagnosis of NMO according to the 2006 criteria 10 by logistic regression (odds ratios (OR), calculation with a 95% confidence interval (CI)). All significant results were set at corrected (correction factor was number of alleles -1) two-tailed p-value <0.05.
Results
Patients
In total, 23 patients from nine centres were included in the study. The clinical characteristics are summarized in Table 1. The median age of presentation was 44.5 years (range: 20–77 years). Of the patients, 16 (69.5%) patients were women; two were Latin American and the rest (91%) of Caucasian origin. Only one patient had a past history of coexisting autoimmune disease (thyroiditis). Two patients had suffered one remote isolated LETM episode 46 and 48 months earlier, with an almost complete recovery. The new episode was considered as the index event, and in the follow-up period the initial episode was only considered for analysis of the time to second event. Most (74%) patients had moderate–severe motor impairment at nadir, 11 (48%) were bed bound/wheelchair bound or required assisted ventilation. The median EDSS score was 7.0 (range 3.0–9.0) (Table 1). All patients received intravenous (IV) steroids during the acute episode. In addition, six patients were treated with plasma exchange, two with IV immunoglobulins and one with cyclophosphamide. At 3 months 39% (9/23) of patients had a complete or almost complete recovery. However, at the last visit (median 32 months; interquartile range 26–37 months), 52% (12/23) of patients had minimal disability (EDSS score
Demographic and clinical characteristics.
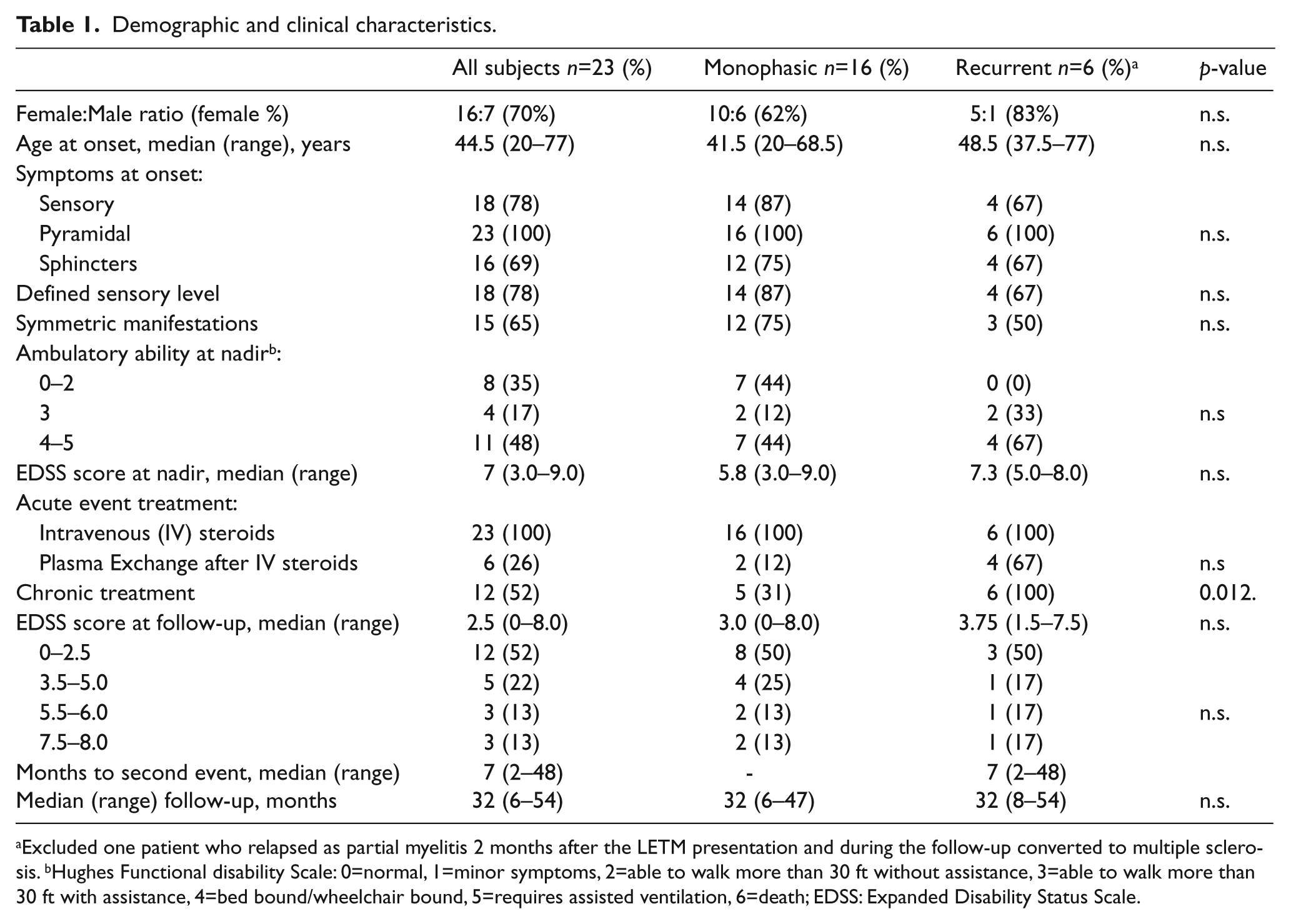
Excluded one patient who relapsed as partial myelitis 2 months after the LETM presentation and during the follow-up converted to multiple sclerosis. bHughes Functional disability Scale: 0=normal, 1=minor symptoms, 2=able to walk more than 30 ft without assistance, 3=able to walk more than 30 ft with assistance, 4=bed bound/wheelchair bound, 5=requires assisted ventilation, 6=death; EDSS: Expanded Disability Status Scale.
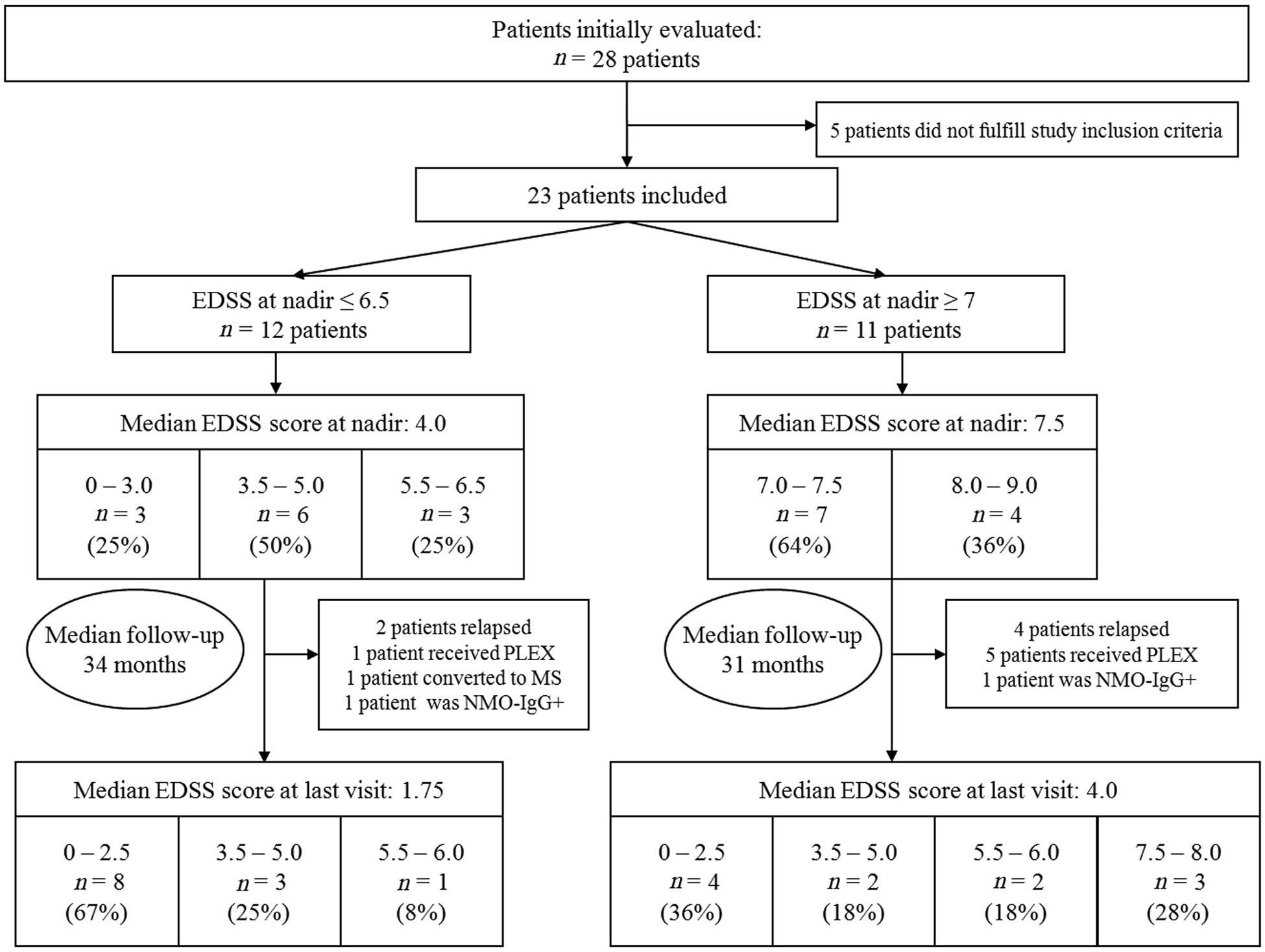
Flow diagram demonstrating evolution and ultimate outcome of patients with greater impairment at nadir (EDSS ≥7) versus patients with ambulatory ability at nadir (EDSS ≤6.5); EDSS: Expanded Disability Status Scale; PLEX: Plasma Exchange.
Laboratory data
A summary of laboratory data is shown in Table 2. Elevated CSF cell count (>5) was found in 45% (10/22) of patients, six of them with >50 cells/mm3, and oligoclonal IgG bands in 24% (5/21). ANA were found in 70% of patients, and anti-Ro antibodies in one. NMO-IgG were present in two (9%) patients (17 patients had at least two serological testings and the median number of NMO-IgG analyses of the whole series was 2, range 1–4). One of the seropositive patients had a previous LETM episode. The available serum sample of the remote episode was retrospectively tested and was also found positive.
Paraclinical data.
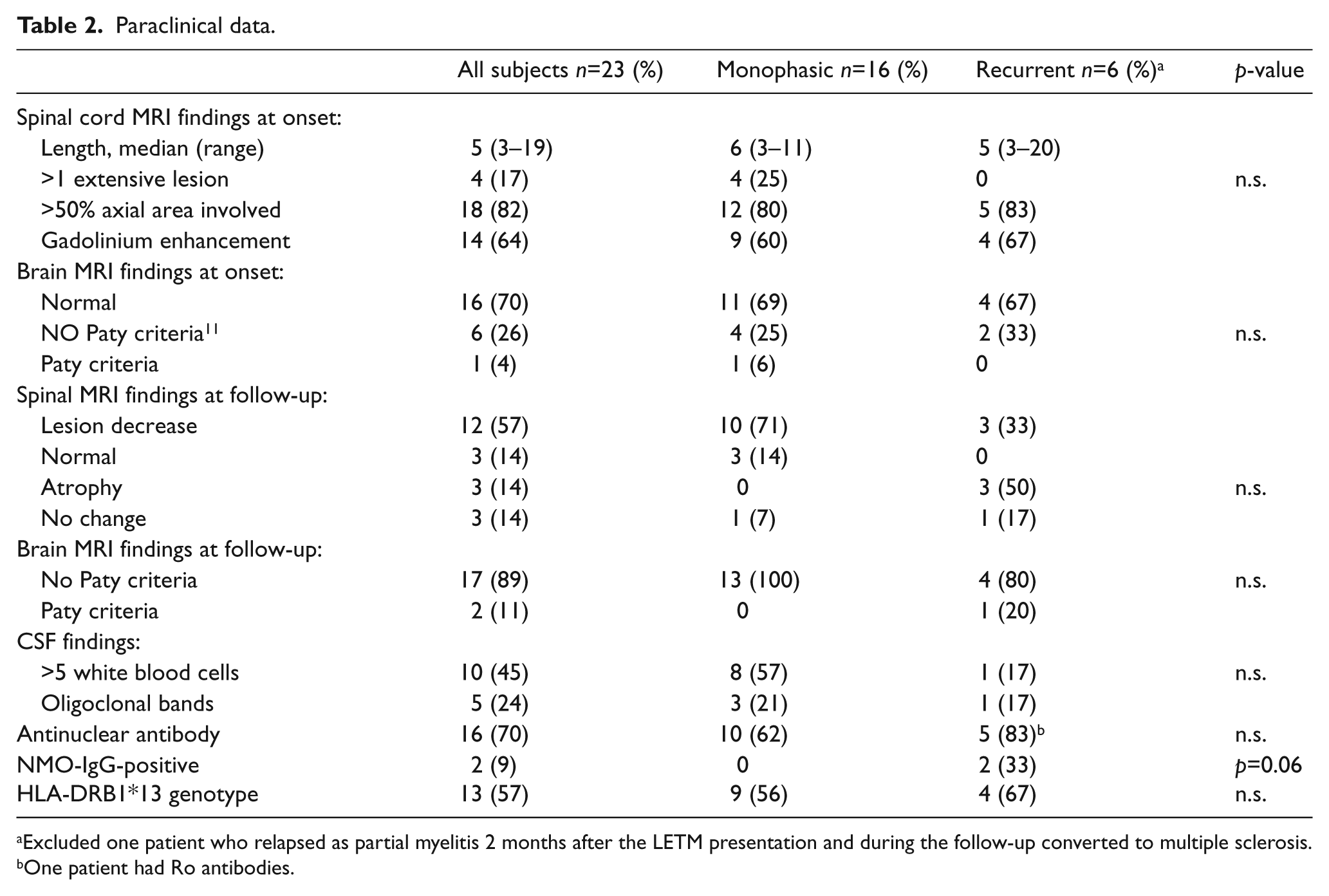
Excluded one patient who relapsed as partial myelitis 2 months after the LETM presentation and during the follow-up converted to multiple sclerosis.
One patient had Ro antibodies.
Onconeuronal antibodies and antibodies against neuronal surface antigens were negative in all patients. The HLA-DRB1 analysis showed that DRB1*13 was the genotype more frequently found in theses patients (13/23; 57%) (Table 2). LETM was associated with a higher frequency of DRB1*13 genotype compared with controls (OR 3.92, 95% CI 1.66–9.44, p=0.002), with MS (OR 4.63, 95% CI 1.92–11.18, p=0.001) and with NMO patients (OR 13.00, 95% CI 2.44–69.13, p=0.003).
Radiological data
Spinal cord MRI performed in the acute phase showed a lesion extending over a median of five (range: 3–19) vertebral segments. In five patients the length of the lesion was >10 vertebral segments. T2 signal abnormalities were identified at cervical levels in seven patients, thoracic levels in seven and both cervical and thoracic levels in nine patients. Seven patients had multifocal lesions, and four of them more than one lesion extending over at least three vertebral segments. The lesion occupied more than half of the cross-sectional area of the spinal cord in 82% (18/22) of patients with gadolinium enhancement in 64% (14/22) of them. Brain MRI at onset was normal or did not fulfil Paty criteria 11 in 96% (22/23) of the patients at the onset of the disease and in 89% (17/19) at last visit. The spinal cord MRI demonstrated an improvement of the LETM in 71.4% (15/21) of patients. The follow-up study (median 12 months; range: 2–39 months) was normal in three (14%) patients and the lesion decreased to <3 vertebral segments in six other (29%) patients (Table 2).
Predictive factors associated with outcome
The EDSS score at nadir correlated with the EDSS score at the end of the study (r=0.594; p=0.003). In the multivariate analysis the EDSS at nadir remained as the only significant variable associated with clinical outcome (OR=0.564, 95% CI 0.33–0.96, p=0.035). No other demographic, clinical or laboratory data was associated with the outcome.
When we compared the recurrent and monophasic LETM groups (Table 1 and 2) we did not find significant differences except for a trend for recurrences to be associated with NMO-IgG seropositivity (Fisher’s exact test; p=0.06). In the multivariate analysis, the number of vertebral segments involved was associated with the risk of recurrence (HR=1.21, 95% CI 1.01–1.45, p=0.042).
Discussion
Studies on isolated inflammatory LETM are relatively rare. Most have the limitation of being retrospective, included in reports of TM or NMO patients, and present limited information on clinical outcome and prognostic factors. 4,12 –17 In this prospective study we report the clinical, paraclinical and outcome features of 23 adult patients who presented with inflammatory LETM.
There was a predominance of middle-aged women with moderate–severe disability at nadir (48% unable to walk). Half of them had an almost complete recovery with minimal disability (EDSS ≤2.5) after a median follow-up of 32 months. The EDSS at nadir was predictive of the final outcome, but only three (13%) of the patients remained wheelchair dependent. This is in contrast to that reported in a retrospective series of 45 patients with idiopathic TM patients in which 15 (33%) had a poor outcome. 18 An important difference between both studies is that we only included patients with LETM. In addition, differences in both the acute and chronic immunotherapy might explain this discrepancy. 18
We found a significant overrepresentation of the genotype HLA-DRB1*13 in LETM patients compared with controls, MS and NMO patients. Several studies indicate that the HLA-DRB1* profile of patients with NMO is different from that observed in MS patients. While HLA-DRB1*15 is consistently associated with MS, HLA-DRB1*03 appears to be associated with NMO-IgG seropositivity. 5,19 –22 To our knowledge, the current study is the first to report this analysis in LETM patients. Although the functional role is not well known, it seems that HLA-DRB1*13 alleles play a role in determining which peptides from an antigenic protein are presented to the T cell. 23 HLA-DRB1*13 alleles may play a protective role for some infections. 23,24 In addition the HLA-DRB1*13 allelic group has been negatively associated with MS in two northern European MS populations, as a part of its corresponding haplotype. 25,26
The rate of conversion to MS or positive NMO-IgG antibodies (NMO spectrum disorder) was low in this series. Up to 87% remained as idiopathic LETM with a 20% frequency of recurrences, similar to that found in retrospective studies in which NMO-IgG were not tested. 18,27 In the only prospective study of LETM, 11 of 29 (38%) patients were positive for NMO-IgG and 56% of them relapsed within 1 year, whereas none of the seronegative patients experienced a second event after a median follow-up of 27.5 months. 4 These findings are in contrast with a much lower frequency of NMO-IgG positivity in our and other retrospective studies. 15,28 The cause of this discrepancy is unclear, but probably is explained in part by referral bias. In the retrospective study from Korea, three out of 20 (15%) patients with first LETM had NMO-IgG antibodies, and 40% of them had recurrent myelitis. The authors suggested that ethnicity could explain the low numbers of LETM patients with a limited form of NMO because in Asians with the opticospinal form of MS the frequency of NMO-IgG antibodies is low. 15 However, we and the study from West Australian 28 found a similar low frequency of NMO-IG antibodies, suggesting that ethnicity is not the only issue.
The frequency of ANA (70%) was higher than that reported in series of patients with MS and NMO spectrum disorders. 14,29 Moreover, one of our patients with recurrent LETM had anti-Ro antibodies, but none of the patients were diagnosed with systemic connective tissue disease. In one study, anti-Ro antibodies were found associated with recurrent TM, but the MRI characteristics were not described and so far confirmatory studies have not been reported. 30 The high coexistence of non-organ-specific autoantibodies in idiopathic LETM as well as in NMO spectrum disorders would support the autoimmune background of these patients.
In the present series, initial brain MRI was normal or non-diagnostic of MS in most patients, including the only patient who converted to MS. This result is in agreement with previous reports on the low rate of conversion to MS in adult patients with LETM, 28 and is in contrast with that reported in children with this disorder. 31 A finding not previously emphasized is that the length of the spinal cord lesions was not associated with the outcome, and the extension of the lesions evolved to less than three vertebral segments in 29% and vanished in another 14% of the patients at follow-up. However, the extension of the spinal cord MRI lesion at onset was an independent predictor for relapse. Our study indicates that all patients who relapsed had a new episode of LETM, relapses may occur many years after the initial event, and the recurrences were not associated with worse final outcome.
This study has several limitations. The follow-up is relatively short and we cannot rule out that monophasic patients present a relapse in the future and increase the frequency of this complication that could be associated with a worse prognosis. In addition, our study was not designed to evaluate the efficacy of immunotherapy in this setting, and the type of therapy was not included in the protocol. Therefore, the role of acute and chronic immunotherapy in the outcome will only be answered with randomized clinical trials.
Footnotes
Acknowledgements
Dr M Rosenfeld for critical review of the manuscript.
Funding
Supported in part by Red Española de Esclerosis Múltiple (REEM) (RD07/0060/001; RD07/0060/0012; RD07/0060/0020; RD07/0060/002), Instituto de Salud Carlos III, Madrid, Spain, and Fundació La Marató de TV3 (A.S., 101610).
Conflict of interest
Dr Sepúlveda reports no disclosures. Dr Blanco reports no disclosures. Dr Rovira serves on scientific advisory boards for NeuroTEC and on the editorial board of the American Journal of Neuroradiology and Neuroradiology, has received speaker honoraria from Bayer Schering Pharma, Sanofi-Aventis, Bracco, Merck Serono, Teva Pharmaceutical Industries Ltd. and Biogen Idec, receives research support from Bayer Schering Pharma, and serves as a consultant for Novartis. Dr Rio has received compensation for consulting services and speaking from Bayer-Schering, Merck-Serono, Biogen-Idec, Sanofi-Aventis, Teva Pharmaceutical Industries Ltd, Novartis and Almirall. Dr Mendibe has received compensation for consulting services and speaking from Bayer-Schering, Biogen-Idec, Merck-Serono, Novartis, Sanofi-Genzyme and Teva Pharmaceutical Industries Ltd. Dr Llufriu has received compensation for consulting services and speaking from Merck-Serono, Biogen-Idec and Teva Pharmaceutical Industries Ltd. Dr Gabilondo reports no disclosures. Dr Villoslada has received consultancy fees from Novartis, Roche, Neurotek, Heidelberg Engineering, Digna Biotech, Bionure and TFS and research grants from Novartis, Roche and Digna Biotech, and is founder and holds stocks in Bionure. Dr Castilló reports no disclosures. Dr Corral reports no disclosures. Dr Ayuso has received speaker honoraria from Merck-Serono, Biogen-Idec, Sanofi-Aventis, Teva Pharmaceutical Industries Ltd and Novartis. Dr Iñiguez reports no disclosures. Dr Santos reports no disclosures. Dr Guijarro has received compensation for consulting services from Bayer-Schering, Biogen-Idec and Teva Pharmaceutical Industries Ltd. Dr Ramió-Torrentà has received compensation for speaking from Bayer-Healthcare, Biogen-Idec, Merck- Serono, Novartis, Sanofi-Aventis, Teva Pharmaceutical Industries Ltd, Almirall and Medtronic; received research support from Biogen-Idec, Merck-Serono, Sanofi-Aventis and Teva Pharmaceutical Industries Ltd; serves on scientific advisory board for Biogen-Idec. Dr Sempere has received speaker honoraria from Bayer-Schering, Biogen-Idec, Merck-Serono, Novartis, Sanofi-Aventis and Teva Pharmaceutical Industries Ltd. Dr Olascoaga has received compensation for consulting services and speaking from Bayer-Schering, Biogen-Idec, Merck-Serono, Novartis, Sanofi-Genzyme and Teva Pharmaceutical Industries Ltd. Dr Graus reports no disclosures. Dr Montalban has received speaking honoraria and travel expenses for scientific meetings, has been a steering committee member of clinical trials or participated in advisory boards of clinical trials in the past years with Bayer Schering Pharma, Biogen Idec, EMD Merck Serono, Genentech, Genzyme, Novartis, Sanofi-Aventis, Teva Pharmaceuticals and Almirall. Dr Saiz has received compensation for consulting services and speaking from Bayer-Schering, Merck-Serono, Biogen-Idec, Sanofi-Aventis, Teva Pharmaceutical Industries Ltd and Novartis.